ORIGINAL RESEARCH ARTICLE
Conservative treatment of traumatic finger amputations using negative-pressure wound therapy
Yasushi Mizutania, Susumu Tamaib, Toshifumi Nakamurab, Yusuke Hagiwaraa, Takehiko Takitaa and Kenji Kawamurac
aOrthopedic Clinic, Takita Hospital, Yamato-Kohriyama-Shi, Nara, Japan; bNara Hand Surgery Institute, Takita Hospital; cDepartment of Orthopedic Surgery, Nara Medical University, Kashihara-City, Nara, Japan
ABSTRACT
Replantation is widely regarded as the first choice of treatment for finger amputations. However, if the fingertip of a traumatic finger amputation is missing after an injury, the following procedures are often performed to reconstruct this portion: flap surgery, stump surgery, or conservative treatment, including occlusive dressings. To our knowledge, no existing English literature reports using negative-pressure wound therapy (NPWT) to treat traumatic finger amputations.
We postulated that NPWT may be applied as a conservative treatment for traumatic finger amputations, promoting the growth of granulation tissue and achieving early epithelialization of the fingertips.
Among the case series of five patients, we included six injured fingers comprising two index, two middle, and two ring fingers. The fingertip of each traumatic finger amputation was either missing or highly crushed, making replantation impossible. To preserve finger length with conservative treatment, we adapted an NPWT device for finger amputations. It took an average of 22.7 days for the fingertips to epithelialize. Immediately after epithelialization, there was a slight decrease in sensory perception; however, all patients showed good recovery of sensory perception after 3 months. Range of motion remained unrestricted, with no reduction in grip strength. Patients were highly satisfied with their fingertip appearance. The regenerated nail exhibited slight deformation and shortening. No complications were observed.
Our novel study regarding this new conservative treatment and its outcomes revealed that healing was achieved in a relatively short period; therefore, NPWT may serve as a new conservative treatment option in the future.
KEYWORDS: Wound therapy; amputation; negative pressure
Citation: Journal of Plastic Surgery and Hand Surgery 2023; 58: 115–118. DOI: https://doi.org/10.2340/jphs.v58.15298.
Copyright: © 2023 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material for non-commercial purposes, provided proper attribution to the original work.
Received: 1 August 2023; Accepted: 4 September 2023; Published: 20 September 2023.
CONTACT Kenji Kawamura kkenji@naramed-u.ac.jp Department of Orthopaedic Surgery, Nara Medical University, 840 Shijyo-cho, Kashihara, Nara 634-8522, Japan.
Competing interests and funding: The authors report there are no competing interests to declare.
None.
Introduction (including a clear statement of the aim of the study)
Worldwide, replantation of an amputated thumb was first reported in 1965 by Tamai et al. [1] and is widely regarded as the first choice of treatment for finger amputations. However, if the fingertip of a traumatic finger amputation is missing after an injury, the following procedures are often performed to reconstruct this portion: flap surgery, stump surgery, or conservative treatment, such as occlusive dressings. Previous reports on conservative treatment with occlusive dressings have shown that it takes approximately 4 weeks for epithelialization of the reconstructed tissue [2–4]. To the best of our knowledge, there is no existing English literature regarding the treatment of traumatic finger amputations using negative-pressure wound therapy (NPWT).
In this report, we postulated that NPWT may be applied as a conservative treatment for traumatic finger amputations to promote the growth of granulation tissue at the fingertips and achieve early epithelialization.
Materials and methods
From 2019 to 2020, we included six injured fingers among the case series of five patients (three men and two women) that involved two index, two middle, and two ring fingers. The average age of the patients was 29.2 years (21–50 years). Injuries of five of the fingers were caused by mechanical forces and included one injury caused by a planar cutting machine and four crush injuries. The injury of the last finger was caused by a dog bite. The fingertip of the traumatic finger amputation was either missing or highly crushed, making replantation impossible. Our patients desired to preserve their finger length using conservative treatment. To achieve this, we gently debrided the amputated surface on the day of the injury and initiated conservative treatment using an NPWT device a day after the injury.
Initially, we applied a non-adhesive gauze to the amputated surface to prevent adhesion of the wound surface to the device, which could have caused pain. The sponge foam was then cut to an appropriate size to cover the amputated surface, and a film was placed over the sponge to prevent air leakage. We connected the sponge and NPWT device to a tube, applying continuous suction with negative pressure (Figure 1). The NPWT device was applied once to twice a week until the amputated surface of the finger was completely epithelialized. We did not use any routine analgesic regimens during the reapplications of the NPWT device. Analgesics, such as oral non-steroidal anti-inflammatory drugs, were administered as needed.

Figure 1. A non-adhesive gauze is placed on the amputated surface and covered with a sponge foam. The sponge foam is covered by a film and connected to the negative-pressure wound therapy (NPWT) device with a tube.
Ethics
This study was approved by the Ethical Committee and Institutional Review Board at our facility, and all patients provided written informed consent to have their data published.
Results
As per the Tamai classification for fingertip classification [5], using NPWT, we treated six Tamai Zone 1 fingers that took an average of 22.7 days (17–35 days) for the fingertips to epithelialize. Immediately after epithelialization, patients reported a slight decrease in sensory perception. However, they all showed a good recovery of sensory perception 3 months after the injury. In addition, their moving and static two-point discrimination test scores were within the normal range; the range of motion (ROM) remained unrestricted; and there was no reduction in grip strength. We observed slight deformation and shortening of the nail; however, the nail ultimately regenerated very well. No complications, such as wound infection and neuroma, were observed. All patients followed up with us every 4–7 days and returned fully to work 2 months after the injury. Representative cases are presented below.
Case 1: A 21-year-old woman presented with a traumatic amputation of the right ring finger (Figure 2). The distal phalanx was exposed; however, we did not perform bone resection, because we wanted to preserve finger length. We attached the NPWT device the day after the injury, and the amputated surface healed within 35 days of the injury. The exposed distal phalanx was covered with granulation tissue, and epithelialization was complete. The patient was pleased with the appearance of her fingertip.

Figure 2. The exposed distal phalanx is covered with granulation tissue, and epithelialization is complete.
Case 2: A 24-year-old woman presented with a traumatic amputation of the left index and middle fingers (Figure 3). The NPWT device was attached a day after the injury. The index finger healed within 17 days, and the middle finger healed within 25 days. This is the only case in which local anesthesia was administered, because the patient experienced sharp pain during the reapplication of the NPWT device.

Figure 3. The index finger shows healing at Day 17, and the middle finger shows healing at Day 25.
Discussion
In this study, we treated relatively young patients who were expected to have a high wound healing ability. We expected these patients to have good blood supply at the wound site, because they had no underlying diseases. Furthermore, we considered that negative pressure and stimulation of the wound surface promoted angiogenesis and the growth of tissue granulation and assisted with the prevention of infection by sucking away hematomas and exudates. The patients had to spend time on NPWT; however, as the device was handheld, it did not substantially hinder their activities of daily living. Our patients were satisfied because their fingers healed cosmetically and did not require frequent changes of the dressings. It is generally believed that the growth of tissue granulation does not occur in the exposed bone. However, as in Case 1, we confirmed that epithelialization may be achieved even if the distal phalanx is exposed.
NPWT was first reported by Argenta and Morykwas in 1997 [6] and has since been used to treat diabetic foot lesions and tissue defects [7, 8]. To the best of our knowledge, no English literature exists regarding the treatment of traumatic finger amputations using NPWT.
At our facility, we routinely perform finger replantations and flap surgeries on finger amputations. Finger replantation can be performed only when the amputated finger is preserved in good condition and when a free or pedicle flap is obtained for the surgery [9, 10]. After flap surgery, the fingertips tend to be slightly thicker. In addition, ROM may be restricted, and sensory deterioration may occur in some cases. Furthermore, donor-site complications, such as surgical scars, skin discomfort or numbness cannot be ignored.
The advantages of conservative treatment of traumatic finger amputations using NPWT are as follows: (1) the patient can undergo ROM training even when the NPWT device is attached to the finger (Figure 4); (2) ROM is not restricted; (3) no donor site is required; (4) epithelialization can be achieved in a relatively short period; and (5) the finger pad can be regenerated and is cosmetically appealing. Moreover, complications such as infection, neuroma, and decreased grip strength were not observed.
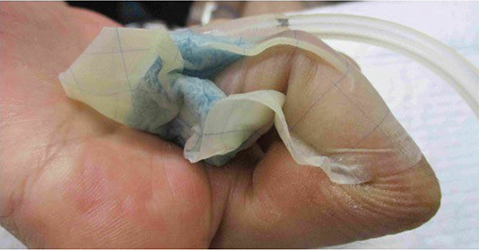
Figure 4. The patient undergoing range-of-motion training, even while the negative-pressure wound therapy (NPWT) device is attached to the finger.
We hypothesize that healing may be achieved without the need for bone resection in young patients, particularly if the bone is exposed.
Our NPWT ensured that epithelialization could be achieved in a relatively short period and may be applied as a new conservative treatment option in the future. Although it is necessary to record similar cases in the future to validate our findings, we can state that conservative treatment using NPWT for Tamai Zone 1 traumatic finger amputations is an effective option for restoring the function of the injured finger.
Acknowledgments
None.
References
[1] Komatsu S, Tamai S. Successful replantation of a completely cut-off thumb. Plast Reconstr Surg. 1968; 42: 374–377. https://doi.org/10.1097/00006534-196810000-00021
[2] Lee LP, Lau PY, Chan CW. A simple and efficient treatment for fingertip injuries. J Hand Surg Br. 1995; 20: 63–71. https://doi.org/10.1016/S0266-7681(05)80019-1
[3] Mennen U, Wiese A. Fingertip injuries management with semi-occlusive dressing. J Hand Surg Br. 1993; 18: 416–422. https://doi.org/10.1016/0266-7681(93)90139-7
[4] Lamon RP, Cicero JJ, Frascone RJ, et al. Open treatment of fingertip amputations. Ann Emerg Med. 1983; 12: 358–360. https://doi.org/10.1016/S0196-0644(83)80465-X
[5] Tamai S. Twenty years’ experience of limb replantation – review of 293 upper extremity replants. J Hand Surg Am. 1982; 7: 549–556. https://doi.org/10.1016/S0363-5023(82)80100-7
[6] Argenta LC, Morykwas MJ. Vacuum-assisted closure: a new method for wound control and treatment: clinical experience. Ann Plast Surg. 1997; 38: 563–576. https://doi.org/10.1097/00000637-199706000-00002
[7] Rys P, Borys S, Hohendorff J, et al. NPWT in diabetic foot wounds-a systematic review and meta-analysis of observational studies. Endocrine. 2020; 68: 44–55. https://doi.org/10.1007/s12020-019-02164-9
[8] Shine J, Efanov JI, Paek L, et al. Negative pressure wound therapy as a definitive treatment for upper extremity wound defects: a systematic review. Int Wound J. 2019; 16: 960–967. https://doi.org/10.1111/iwj.13128
[9] Martin C, González del Pino J. Controversies in the treatment of fingertip amputations. Conservative versus surgical reconstruction. Clin Orthop Relat Res. 1998; 353: 63–73. https://doi.org/10.1097/00003086-199808000-00008
[10] Hirasé Y, Kojima T, Matsui M. Aesthetic fingertip reconstruction with a free vascularized nail graft: a review of 60 flaps involving partial toe transfers. Plast Reconstr Surg. 1997; 99: 774–784. https://doi.org/10.1097/00006534-199703000-00026