ORIGINAL RESEARCH ARTICLE
Animation of latissimus dorsi flap in breast reconstruction: a retrospective analysis based on 203 cases
Yoshihiko Fujita, MDa,b, Noriko Matsunaga, MDa, Maiko de Kerckhove, MD, PhDa, Shoichi Tomita, MD, PhDa, Miwako Fujii, MDa and Yasunobu Terao, MD, PhDa
aDepartment of Plastic and Reconstructive Surgery, Tokyo Metropolitan Cancer and Infectious Diseases Center, Komagome Hospital, Tokyo, Japan; bDepartment of Plastic and Reconstructive Surgery, The Jikei University Kashiwa Hospital, Chiba, Japan
ABSTRACT
Background: Breast animation is a common postoperative complication of breast reconstruction surgery. This study investigates the factors affecting the onset and degree of animation to suggest an ideal treatment strategy for this complication.
Methods: This study included patients who underwent latissimus dorsi reconstruction at Tokyo Metropolitan Cancer and Infectious Diseases Center, Komagome Hospital, between 2009 and 2020 and had an outpatient visit after July 2020. Statistical analysis was performed and the patients’ background and surgical factors were examined to determine whether they affected the animation incidence rate.
Results: The animation incidence rate was 69.6%. There was no significant relationship between animation incidence and any patient background or surgical factors, except for the complete dissection of insertion into the humerus of the latissimus dorsi muscle (p = 0.0039). The rate of uncomfortable animation was 4% and recurrence of animation was observed in one of the two patients who underwent denervation.
Conclusion: Prophylactic denervation is not considered necessary and should be offered only for persistent discomfort with animation. Instead, the muscle insertion must be dissected during flap elevation to prevent animation, and the thoracodorsal nerve must be preserved to avoid muscle atrophy.
KEYWORDS: Animation deformity; twitching; latissimus dorsi flap; breast reconstruction; thoracodorsal nerve; denervation.
Citation: Journal of Plastic Surgery and Hand Surgery 2024; 59: 128–131. DOI: https://doi.org/10.2340/jphs.v59.39952.
Copyright: © 2024 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 16 January 2024; Accepted: 26 August 2024; Published: 15 October 2024
CONTACT: Yoshihiko Fujita y.s.h.k.t.n.s.i@gmail.com Department of Plastic and Reconstructive Surgery, The Jikei University Kashiwa Hospital, 163-1 Kashiwashita, Kashiwa-shi, Chiba, 277-0004, Japan
Competing interests and funding: The authors report there are no competing interests to declare.
This study was conducted without financial support.
Introduction
The pedicled myocutaneous latissimus dorsi flap is one of the most common breast reconstruction surgeries. The main advantages of this method over free flaps consist of shorter operation times and faster postoperative recovery times. However, this method has several complications. For instance, one of the common complications following breast reconstruction with a latissimus dorsi flap is breast animation. Breast animation is an involuntary contraction of the latissimus dorsi muscle that may occur following reconstruction surgery, causing discomfort to the patient. This complication has been evaluated in only a few studies and the reported incidence rates vary widely (18.3%–100.0%) [1–7]. Moreover, no standard evaluation methods or clear guidelines govern surgical procedures involving the thoracodorsal nerve or insertion of the latissimus dorsi muscle, which have been discussed as possible causes for developing animation [1, 8].
In this study, we investigated the frequency, severity, onset of animation, and the relationship between patients’ background, including age, body mass index (BMI), etc., and surgical technique among patients undergoing reconstruction with a latissimus dorsi flap. We developed our own classification criteria to simplify the method of evaluating animation. Based on previous reports and the findings of this study, we discuss the mechanism of onset, the classification criteria of animation, and the recommended surgical techniques that would limit the incidence of this complication.
Methods
This retrospective study included all the patients who underwent breast reconstruction with the latissimus dorsi flap between 2009 and 2020 at Tokyo Metropolitan Cancer and Infectious Diseases Center, Komagome Hospital. The clinical evaluation was performed by six physicians, all of whom are author or co-authors, with 5 to 30 years of experience as breast reconstructive surgeons. The cases in which both breasts were reconstructed with bilateral latissimus dorsi flaps were counted independently. The patients with no outpatient appointments and those no longer reachable were excluded. The outpatient examination involved strong shoulder adduction in assessing whether the movement of the reconstructed breast could be distinguished from the movement of the pectoralis major muscle. Subsequently, patients were graded based on the presence or absence of findings, subjective symptoms, and level of discomfort. Grade 2 was further classified into Grade 2a and Grade 2b according to the frequency of subjective symptoms (Grade 2a: occasional, Grade 2b: frequent) (Table 1). The patients’ background and surgical factors were considered part of the evaluation criteria in the analysis. Patients’ background included age, BMI, exercise habits, the relationship between the dominant arm and reconstructed side, and the follow-up period since reconstruction. Surgical factors included the volume of mastectomy, the presence or absence of axillary dissection, immediate or delayed reconstruction, whether reconstruction is with a latissimus dorsi flap alone, a fat-augmented latissimus dorsi flap, or a latissimus dorsi flap combined with implant, and whether dissection of muscle insertion was performed or unspecified. We investigated the relationship between these factors and the grade of animation post-operatively. Moreover, following denervation, the frequency of animation recurrence was also assessed.
| Grade | Animation | Subjective symptom | With discomfort |
| 0 | - | - | - |
| 1 | + | - | - |
| 2a | + | + (occasional) | - |
| 2b | + | + (frequent) | - |
| 3 | + | + | + |
Ethics
This study was approved by the ethical review board in Tokyo Metropolitan Cancer and Infectious Diseases Center, Komagome Hospital (The approval number is 2756) and follows the principles of the declaration of Helsinki.
Surgical technique
The thoracodorsal nerve was preserved during the elevation of the latissimus dorsi flap in all patients. Patients were categorized into two groups according to the degree of muscle dissection at the insertion into the humerus: the complete dissection group and the incomplete or no dissection group. In the first group, the completely dissected humeral insertion of the latissimus dorsi muscle was anchored to the pectoralis major muscle (Figure 1). Grade 3 patients were offered secondary denervation if they desired it. This involved transecting more than 4 cm of the thoracodorsal nerve as proximally as possible. Patients who underwent secondary denervation were followed up to assess for animation recurrence.
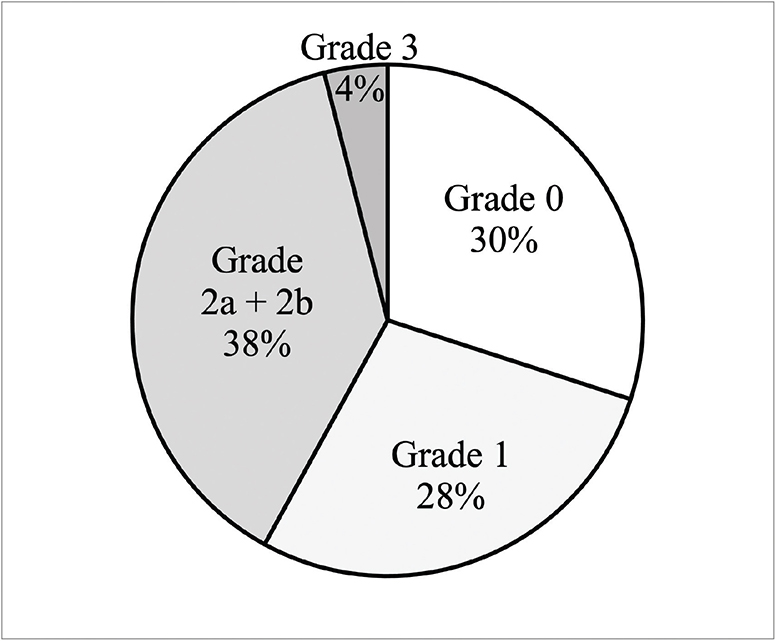
Figure 1. Our grading criteria for animation. The incidence rate of animation was 69.6%. The rate of uncomfortable animation was 4%.
Statistical analysis
Patients were divided into two groups: Grade ≤ 1 and Grade ≥ 2. The Mann–Whitney U test was used for continuous data, and the Chi-squared test was used for categorical data. Statistical significance was reported as p < 0.05 (Table 2). All statistical analyses were performed using EZR [9] (Saitama Medical Center, Jichi Medical University, Saitama, Japan), a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria), which is a modified version of the R commander designed to add the statistical function frequency used in biostatistics.
| Total | Grade 0–1 | Grade ≥ 2 | p | |
| (n = 203) | (n = 118) | (n = 85) | ||
| Age | 48.0 y (26–73) | 47y | 49 y | n.s. |
| BMI | 20.9 (15.5–41.5) | 20.7 | 21 | n.s. |
| Exercise habit | 68 (33.5%) | 38 | 30 | n.s. |
| Dominant side | 109 (53.4%) | 59 | 50 | n.s. |
| Follow-up period | 24.1 m (0.5 m–12 y) | 19.5 m | 25.4 m | n.s. |
| Volume of mastectomy | 258.0 g (63–860) | 257 g | 259 g | n.s. |
| Axillary dissection | 35 (17.2%) | 20 | 15 | n.s. |
| Immediate reconstruction | 167 (82.3%) | 94 | 73 | n.s. |
| fat-augmented LD | 4 (2.0%) | 2 | 2 | n.s. |
| LD+implant | 16 (7.9%) | 12 | 4 | n.s. |
| Complete dissection of humeral insertion of LD | 38 (18.6%) | 30 | 8 | p = 0.0039* |
| BMI: Body mass index; LD: Latissimus dorsi; y: Years; m: Months; n.s.: Not significant; *: Significant. | ||||
Results
This retrospective study enrolled 203 patients aged 48.0 years on average (26–73). The average patients’ BMI was 20.9 (15.5–41.5), the average volume of mastectomy was 258.0 g (63–860), and the follow-up period was 24.1 months (0.5–144). Among the cases, 69.6% had findings consistent with those of animation and were graded accordingly (Grades 1–3). A total of 28% of patients presented with Grade 1, 38% with Grade 2a + 2b, and 4% with Grade 3 animation (Figure 2). Statistical analysis showed a significant difference only in the complete dissection group (p = 0.0039) among the evaluation factors considered in the study (Table 2). For instance, no patient background items showed statistically significant differences, and there was no statistically significant difference between the reconstruction methods, whether a fat-augmented latissimus dorsi flap (p = 0.7393) or combination of latissimus dorsi flap and implant (p = 0.1540). No Grade 3 patients had the latissimus dorsi muscle insertion dissected during breast reconstruction. A total of two out of the eight Grade 3 patients were elected for secondary denervation surgery, and the insertion of the latissimus dorsi muscle was dissected at the same time as the denervation. Only one of these two patients experienced animation recurrence 3 months after secondary denervation.
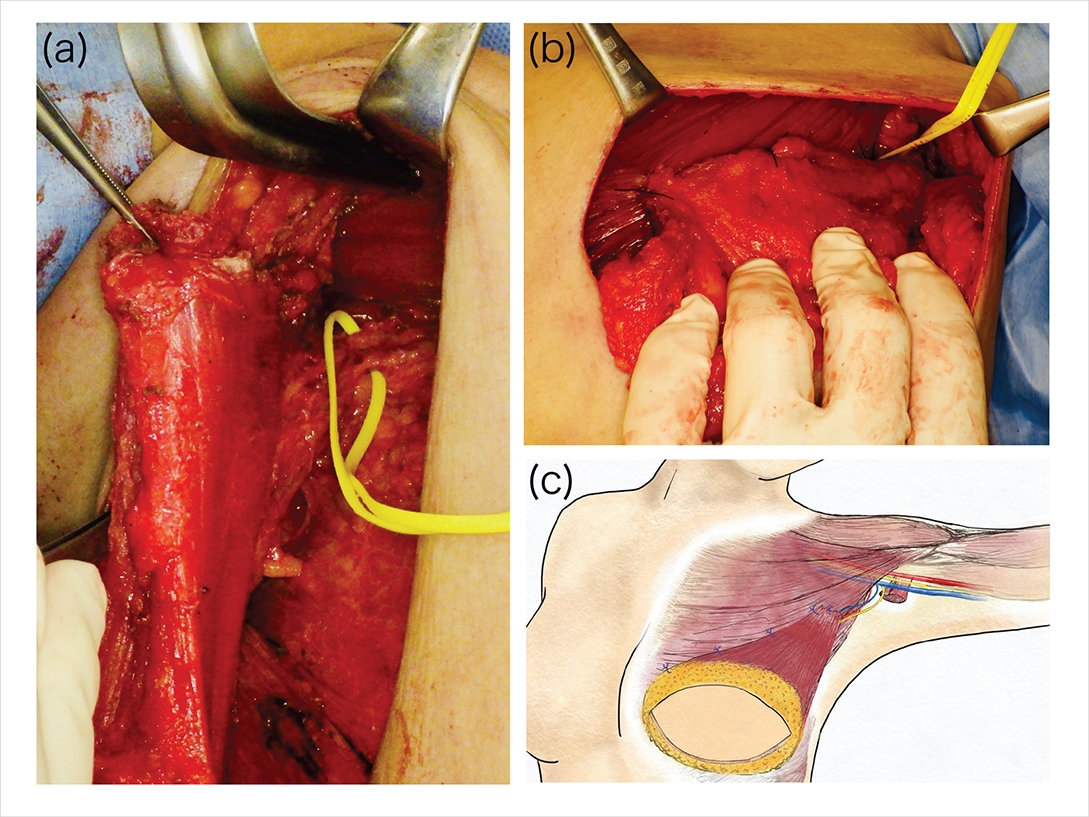
Figure 2. (A) The thoracodorsal artery, vein and the thoracodorsal nerve (taped) were preserved. The insertion of the latissimus dorsi muscle was completely dissected (held with forceps). (B) The humeral insertion and edge of latissimus dorsi muscle were anchored to the pectoralis major muscle in a position that did not put tension on the pedicle of the flap. (C) Illustration of the surgery.
Discussion
Animation was observed in 69.6% of cases and was accompanied by discomfort (Grade 3) in 4% of cases (Figure 2). Although the incidence is high, treatment such as denervation should not be indicated for all patients. Especially, treatment indications for patients without discomfort should be carefully reviewed. Moreover, quantifying the dynamic contraction of muscles is difficult and is considered to be easily influenced by the subjectivity of the evaluator. This is evidenced by the results of previous studies, which were largely inconsistent (Table 3). In future studies on tackling countermeasures against animation, it may be necessary to develop evaluation criteria that are as reproducible and objective as possible. Senger and Wolfri [7] classified late-onset animation following denervation into four grades (Grades 0–3) according to the degree of motion of the reconstructed breast and how it correlates with shoulder motion. Grade 3 is unrelated to shoulder motion and was further classified into three grades according to the degree of motion (Grade 3a: mild, Grade 3b: moderate, Grade 3c: severe). In our study, to eliminate the subjectivity of the evaluator as much as possible, we classified animation according to the presence or absence of motion of the reconstructed breast, subjective symptoms of the patient, and discomfort. Our classification criteria included the presence or absence of discomfort, which can be a clear indicator for initiating treatment.
Statistical analysis of patient backgrounds and surgical factors showed no significant differences, except for the complete dissection group. This correlates well with a study by Kääriäinen et al. [8] evaluating the degree of breast atrophy in patients who underwent breast reconstruction with a latissimus dorsi flap, where it was reported that all patients underwent dissection of the humeral insertion, and this actually prevented early postoperative breast contraction to the axilla and thus less atrophy. Our study demonstrates that the complete dissection of insertion prevents animation and atrophy with statistical significance.
Animation can occur in every patient with thoracodorsal nerve sparing. It is important to realize that every patient has the potential to move, but there are patients with varying degrees of symptoms, depending on the individual. We removed the nerve secondarily in patients with discomfort; however, the recurrence was observed in one of two cases. Otani et al. [10] investigated the relationship between thracodorsal nerve processing methods and atrophy of fat-grafted latissimuss dorsi flap in a study using mice, suggesting that denervation causes atrophy in the muscle flap and grafted fat. Longo et al. [11] also conducted a study on breast reconstruction by a fat-augmented latissimus dorsi flap after total mastectomy and radiation therapy, and preserved the thoracodorsal nerve during elevation of the latissimus dorsi flap to prevent atrophy of the muscle. The risk of muscle atrophy should also be considered, and the thoracodorsal nerve should not be transected during breast reconstruction using a latissimus dorsi flap. Instead, the muscle insertion should be dissected to manage animation at the point of breast reconstruction.
Limitations
A major limiting factor for our study is that long-term follow-up is needed to better understand the factors affecting breast animation incidence following breast reconstruction surgery with a latissimus dorsi flap.
Conclusion
Animation of the breast is a common complication following reconstruction with a latissimus dorsi flap. It has a high incidence but has been a problem only in a few cases. Our study shows that prophylactic transection is unnecessary, and the thoracodorsal nerve must be preserved to prevent muscle atrophy. Alternatively, dissection of the muscle insertion into the humerus at flap elevation significantly prevents animation. If uncomfortable animation occurs, secondary denervation should be performed as treatment.
Acknowledgments
The authors would like to thank Editage [http://www.editage.com] for editing and reviewing this manuscript for English language.
References
[1] Halperin TJ, Fox SE, Caterson SA, et al. Delayed division of the thoracodorsal nerve. Ann Plast Surg. 2007; 59: 23–25. https://doi.org/10.1097/01.sap.0000258975.55090.20
[2] Chang DW, Youssef A, Cha S, et al. Autologous breast reconstruction with the extended latissimus dorsi flap. Plast Reconstr Surg. 2002; 110: 751–761. https://doi.org/10.1097/00006534-200209010-00005
[3] Figus A, Mazzocchi M, Dessy LA, et al. Treatment of muscular contraction deformities with botulinum toxin type A after latissimus dorsi flap and sub-pectoral implant breast reconstruction. J Plast Reconstr Aesthet Surg. 2009; 62: 869–875. https://doi.org/10.1016/j.bjps.2007.07.025
[4] Paolini G, Longo B, Laporta R, et al. Permanent latissimus dorsi muscle denervation in breast reconstruction. Ann Plast Surg. 2013; 71: 639–642. https://doi.org/10.1097/SAP.0b013e31825c0840
[5] Szychta P, Butterworth M, Dixon M, et al. Breast reconstruction with the denervated latissimus dorsi musculocutaneous flap. Breast. 2013; 22: 667–672. https://doi.org/10.1016/j.breast.2013.01.001
[6] Schroegendorfer KF, Hacker S, Nickl S, et al. Latissimus dorsi breast reconstruction: how much nerve resection is necessary to prevent postoperative muscle twitching? Plast Reconstr Surg. 2014; 134: 1125–1129. https://doi.org/10.1097/PRS.0000000000000739
[7] Senger J‐L, Wolfli J. Late animation deformity in the denervated pedicled latissimus dorsi flap. Breast J. 2020; 26: 685–690. https://doi.org/10.1111/tbj.13497
[8] Kääriäinen M, Giordano S, Kauhanen S, et al. No need to cut the nerve in LD reconstruction to avoid jumping of the breast: a prospective randomized study. J Plast Reconstr Aesthet Surg. 2014; 67: 1106–1110. https://doi.org/10.1016/j.bjps.2014.04.029
[9] Kanda Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013; 48: 452–458. https://doi.org/10.1038/bmt.2012.244
[10] Otani N, Tomita K, Kuroda K, et al. Effects of temporary and permanent muscle denervation on fat graft retention in the latissimus dorsi muscle: an experimental study in rats. Aesth Plast Surg. 2022; 46: 1942–1949. https://doi.org/10.1007/s00266-022-02813-x
[11] Longo B, D’Orsi G, Vanni G, et al. Fat-augmented latissimus dorsi flap for secondary breast reconstruction in small to medium-sized irradiated breasts. Plast Reconstr Surg. 2013; 152: 1165–1173.