ORIGINAL RESEARCH ARTICLE
Breast volume in non-obese females is related to breast adipose cell hypertrophy, inflammation, and COX2 expression
Silvia Gogg, PhDa, Annika Nerstedt, PhDa, Ulf Smith, MD, PhDa and Emma Hansson, MD, PhDb,c
aThe Lundberg Laboratory for Diabetes Research, Department of Molecular and Clinical Medicine, Institute of Medicine, the Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden; bDepartment of Plastic Surgery, Institute of Clinical Sciences, the Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden; cRegion Västra Götaland, Sahlgrenska University Hospital, Department of Plastic Surgery, Gothenburg, Sweden.
ABSTRACT
Background: Breast hypertrophy seems to be a risk factor for breast cancer and the amount and characteristics of breast adipose tissue may play important roles. The main aim of this study was to investigate associations between breast volume in normal weight women and hypertrophic adipose tissue and inflammation.
Methods: Fifteen non-obese women undergoing breast reduction surgery were examined. Breast volume was measured with plastic cups and surgery was indicated if the breast was 800 ml or larger according to Swedish guidelines. We isolated adipose cells from the breasts and ambient subcutaneous tissue to measure cell size, cell inflammation and other known markers of risk of developing breast cancer including COX2 gene activation and MAPK, a cell proliferation regulator.
Results: Breast adipose cell size was characterized by cell hypertrophy and closely related to breast volume. The breast adipose cells were also characterized by being pro-inflammatory with increased IL-6, IL-8, IL-1β, CCL-2, TNF-a and an increased marker of cell senescence GLB1/β-galactosidase, commonly increased in hypertrophic adipose tissue. The prostaglandin synthetic marker COX2 was also increased in the hypertrophic cells and COX2 has previously been shown to be an important marker of risk of developing breast cancer. Interestingly, the phosphorylation of the proliferation marker MAPK was also increased in the hypertrophic adipose cells.
Conclusion: Taken together, these findings show that increased breast volume in non-obese women is associated with adipose cell hypertrophy and dysfunction and characterized by increased inflammation and other markers of increased risk for developing breast cancer.
Trial registration: Projektdatabasen FoU i VGR, project number: 249191 (https://www.researchweb.org/is/vgr/project/249191)
KEYWORDS: Breast cancer; breast volume; risk factors; adipocyte hypertrophy; inflammation; cell senescence
Citation: Journal of Plastic Surgery and Hand Surgery 2024; 59: 83–88. DOI: https://doi.org/10.2340/jphs.v59.40754.
Copyright: © 2024 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 11 January 2024; Accepted: 29 April 2024; Published: 15 May 2024
CONTACT Emma Hansson emma.hansson.2@gu.se Department of Plastic Surgery, Röda Stråket 12, SE-413 14 Gothenburg, Sweden
Supplemental data for this article can be accessed online at https://doi.org/10.2340/jphs.v59.40754
Competing interests and funding: The authors declare that they have no competing interests.
EH’s university position is funded by the Swedish Cancer Society [21 0279 SCIA].
Background
Obesity is an established risk factor for breast cancer and the adipose tissue is considered to play a crucial role through its tissue secretion of oestrogens as well as increased local tissue chronic inflammation and secretion of leptin and several different cytokines [1, 2]. Importantly, breast size, which also can be positively correlated with body weight [3], is considered a risk factor for breast cancer [4]. However, large breasts seem to remain a risk factor for cancer also when adjusted for body mass index (BMI) [5]. A prospective study [5] on self-reported cup size and cancer risk among 89,268 women concluded that a D cup or larger is a risk factor for breast cancer in women with a BMI under 25 (hazard ratio [HR] = 1.80, 95% confidence interval [CI]: 1.13–2.88, p = 0.01). Furthermore, one study [6] comprising 79,124 women found that self-reported cup size is a predictor for breast cancer mortality also when adjusted for BMI (HR = 1.58, 95% CI: 1.27–1.97, p < 0.0001). Another study [7], including 772 breast cancer patients, demonstrated that a breast volume of more than 850 millilitres (ml) is a risk factor for a shorter disease-free survival (HR 3.64, 95% CI: 1.42–9.35, p = 0.007) and distant metastasis-free survival (HR 6.33, 95% CI: 1.36–29.43, p = 0.019) in women with oestrogen receptor positive tumours, when adjusted for BMI. Interestingly, a genome wide-association study [8] concluded that some single-nucleotide polymorphisms (SNPs) are associated with both breast size and breast cancer. Hence, the total amount of body fat itself might not be the sole contributor to risk of breast cancer, as the local amount of breast adipose tissue and its characteristics may play important roles [9].
Adipocytes located in the breast have certain site-specific qualities (reviewed in [10]). They regulate growth and function of the breast epithelium and have a role in the tumour microenvironment [11–13] (reviewed in [14] and [15]). One aspect that affects the characteristics of the adipose tissue is how it expands. Adipose tissue can expand by an increase in the number of differentiated adipocytes (hyperplastic obesity) and/or by enlargement of existing adipocytes (hypertrophic obesity) [16], and the latter has been shown to be particularly important for several obesity-associated disorders including insulin resistance, Type 2 diabetes and cardiovascular disease. Histologically, the inflammation in hypertrophic adipose tissue is characterised by crown-like structures (CLS), composed of dead/dying adipocytes surrounded by macrophages in a crown-like pattern [17–21]. An association between the occurrence of CLS in the breast (CLS-B) and breast cancer has been seen in several studies and also seem to influence the prognosis (reviewed in [22]). Two case-control studies, comparing women with benign breast disease who later developed breast cancer with those who did not, found an association between the occurrence of CLS-B and the development of breast cancer [17, 23]. It is unknown why signs of inflammation occur in breast adipose tissue of some women with a normal BMI. Moreover, it has never been studied if breast adipose tissue can be characterised as hypertrophic adipose tissue in normal weight women with breast hypertrophy.
The main aim of this study was to investigate if there is an association between a breast volume in normal weight women with breast hypertrophy and hypertrophic adipose tissue and inflammation, which could contribute to the increased cancer risk associated with increased breast volume.
Materials and methods
Study protocol and ethics
The study is described in the “Inflammation in breast fat” protocol (Projektdatabasen FoU i VGR, project number: 249191 (https://www.researchweb.org/is/vgr/project/249191)). The Regional Ethical Committee of Gothenburg reviewed and approved the study (559-18). The procedures followed were in accordance with the Helsinki declaration. The participants gave their informed consent to participation in the study and to the publication of the results.
Setting and study population
Participants were recruited between 2019 and 2023, with a pause during the pandemic, among the patients on the waiting list for a breast reduction in the Department of Plastic and Reconstructive Surgery, Sahlgrenska University Hospital. According to national Swedish guidelines [24] a breast reduction can be performed in the public health care system in women with a volume of >800 ml per breast at a BMI of less than 25 if she is under 50 years of age and less than 27 if she is older than 50 years of age. For this study, we defined large volume breasts as >800 ml, in accordance with the Swedish guidelines [24]. Clinical routines were as per the guidelines, that is a mammogram was performed before the operation and pathological anatomical diagnosis after the operation in all patients over the age of 40 years.
Patients were eligible to participate in the study if they were: (1) biological women (2) on the waiting list for a breast reduction (3) BMI ≤ 27 kg/cm2. Exclusion criteria included: (1) inability to give informed consent (2) previous breast surgery (3) cancer history (4) comorbidity that can give rise to inflammation (5) smoking.
Clinical measurements, blood samples, and adipose tissue biopsies
Breast volume was measured in millilitres with plastic cups (Emballageform AB, Limhamn, Sweden). During the measurement, the breast is lifted by the examiner and the rim of the cup is placed in the sub mammary fold, all breast tissue placed in the cup, which is then pushed against the thoracic wall and the volume estimated. Different cups are used until all breast tissue fits into the cup and there is no air in it. The used cup set comprises 14 cups ranging from 125 ml to 2,000 ml. Body weight was measured on scales and rounded to the nearest 0.5 kilogram and body height with a tape ruler and rounded to nearest centimetre. BMI was calculated as kilogram/meter2. Resection weight was measured on scales and rounded to the nearest milligram.
Venous blood was drawn on the day of the operation, after overnight fasting. Blood samples were processed and analysed according to standard methods at the central laboratory of Sahlgrenska University hospital and the following tests were performed in plasma : C-reactive protein (CRP) (reference interval < 3 mg/litre [L]), insulin (2.7–17 mU/L), glucose (4.0–6.0 mmol/L), aspartate transaminase (AST) (0.25–0.60 µkat/L), alanine transaminase (ALAT) (0.15–0.75 µkat/L), and bilirubin (5–25 µmol/L).
Open biopsies were taken in a standardised fashion during the participant’s operation. Breast tissue and adipose tissue was resected en bloc and two adipose tissue biopsies were taken from the resected tissue. Another biopsy was taken, using the same technique, from the subcutaneous adipose tissue lateral or caudal of the breast. Tissue biopsies were processed immediately.
Isolation of stromal cells from adipose tissue biopsies
Breast and subcutaneous adipose tissue were obtained from the surgical procedure, estimated weight (300–700 mg). Part of the tissue biopsies was snap-frozen and used for subsequent lysates and ribonucleic acid (RNA) isolation. In addition, mature adipocytes were isolated and used for cell size, RNA, and lysates. Briefly, the fresh biopsies were washed with PBS, cut into small pieces, and digested with 0.28 mg/mL collagenase (Collagenase from Clostridium histolyticum, Sigma-Aldrich) in M199 media (Invitrogen) containing 4% BSA, 25 mM HEPES and 5.6 mM glucose, for 50 min at 37°C in a shaking water bath. The digest was filtered through nylon mesh with a pore size of 250 µm, washed four times with fresh medium and the upper fraction containing the floating isolated adipose cells was collected and snap-frozen.
RNA extraction and quantitative real-time PCR
Frozen intact adipose tissue and frozen isolated adipocytes were first suspended in QIAzol Lysis Reagent (QIAGEN) before homogenization with Mixer Miller (MM400, Retsch GmbH). RNA was separated by addition of chloroform. After separation, the water phase containing RNA was used for isolation with the E.Z.N.A. total RNA kit (Omega Bio-Tek). Quantification of RNA was performed with NANODROP 1000 Spectrophotometer (Thermo Fisher Scientific). Complementary deoxyribonucleic acid (cDNA) synthesis was performed with the High-Capacity cDNA kit (Thermo Fisher Scientific) according to the manufacturer’s recommendations. Gene expression was analysed with the Quant Studio6 sequence detection system (Thermo Fisher Scientific). Gene-specific primers and probes were designed using Primer Express software (Thermo Fisher Scientific) or purchased as custom TaqMan gene expression assays (Thermo Fisher Scientific). Both are listed in Supplementary Table 1. Relative expression was calculated using the ∆∆Ct method with normalization to 18S (endogenous control).
Whole-cell extracts and Western blot analyses
Whole-cell protein lysates were prepared, and Western blot analyses were performed as previously described [25]. Briefly, protein concentration was determined using the Pierce BCA Protein Assay Kit (Thermo Fisher Scientific), and 10 μg whole-cell extracts were loaded on NuPAGE Novex 4% – 12% Bis-Tris protein gels (Thermo Fisher Scientific). The Trans-Blot Turbo Transfer System (Bio-Rad) was used for protein transfer, and to ensure that the procedure had been fully completed, the membranes were stained using 0.5% Ponceau S (Merck Chemicals). For the detection of specific proteins, the following primary antibodies were used: Phospho-p44/42 MAPK(Erk1/2) (Thr202/Tyr204) Cell Signaling #9106 and MAPK 1/2 (Erk1/2) Millipore #06-182. Secondary antibodies: Anti-mouse IgG, HRP-linked, Cell Signaling #7076 and Anti-rabbit IgG, HRP-linked, Cell Signaling #7074.
Statistics
The statistical analyses were performed using GraphPad Prism 10 Statistics software (Dotmatics). Normal data distribution was determined using Shapiro-Wilk and D’Agostino & Pearson tests. To assess correlation between variables, Spearman rank correlations were used. Data analyses are presented as means ± SEM. Statistical evaluation between groups was performed by unpaired Student’s t-test or Mann-Whitney test. A p-value of ≤0.05 was considered statistically significant.
Results
A total of 15 healthy and non-obese participants were included in the study. The average age was 33.9 years (range 18–69 years) and only one individual was above 55 years of age. The average BMI was 23.0 kg/m2 (range 18.7–27 kg/m2), preoperative breast volume was 1,112 ml (range 780–1,900 ml), and resected weight was 575 g (range 255–1,229 g) (Table 1). Plasma levels of CRP, insulin, gulcose, AST, ALAT, and bilirubin were within the normal range for all patients. Thus, this is a group of non-obese and healthy individuals.
As shown in Figure 1A, breast volume was closely correlated to the mammary adipose cell size (r = 0.5677). Interestingly, ambient subcutaneous and breast adipose cell diameters were closely correlated (r = 0.849) (Supplementary Figure 1). However, as shown in Figure 1B, breast adipose cells were around 10 µm larger than the subcutaneous adipose cells. Thus, mammary adipose cells are larger than the ambient abdominal subcutaneous cells and closely correlated with breast volume.
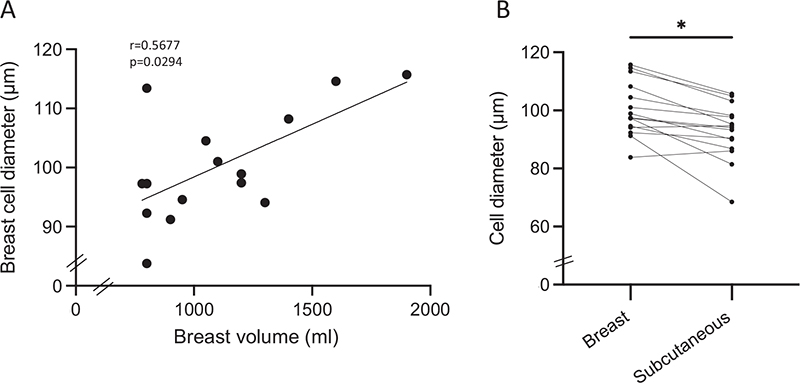
Figure 1. Adipose cell size correlated with breast volume and was larger in breast than in adipose subcutaneous adipose tissue. (A) Spearman rank correlation between breast cell diameter and breast volume (n = 15). Spearman’s correlation coefficient r and p-values are indicated in the graphs. (B) Breast adipose cells were larger than the subcutaneous adipose cells (n = 15). Bars represent mean ± SEM. Statistical significance was determined using Student unpaired t test. *P < 0.05.
We then examined if this hypertrophic enlargement of the mammary adipose cells was related to inflammation. As shown in Figure 2A–E, there was a close correlation between interleukin-6 (IL-6), IL-8, IL-1β, tumor necrosis factor-α (TNF-α), and C-C motive chemokine ligand 2 (CCL2, also known as macrophage colony factor 1 [MCP1]) mRNA (messenger RNA) and mammary adipose cell size indicating increased inflammation in the hypertrophic cells in breast. This was also true for the ambient subcutaneous adipose cells (Supplementary Figure 2A–E) in these non-obese individuals. Interestingly, GLB1 (galactosidase beta), the gene that encodes the protein β-galactosidase, a marker of cell senescence, was also increased in the large adipose cells in both breast (Figure 2F) and subcutaneous cells (Supplementary Figure 2F). Taken together, these data show that individuals with large breasts have expanded and pro-inflammatory cells also characterized by an increased common marker of cell senescence.
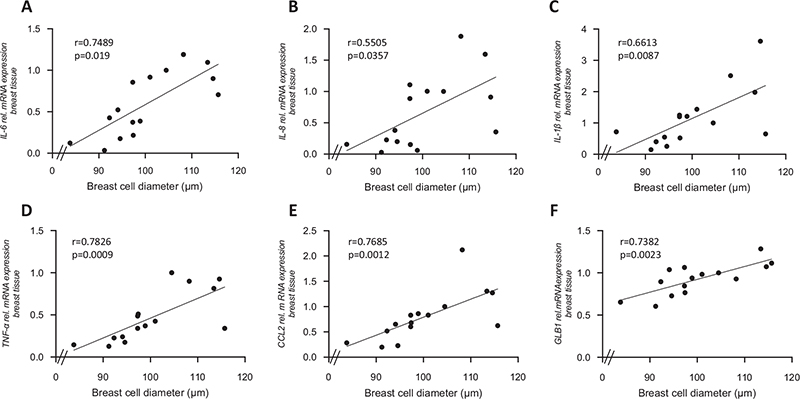
Figure 2. Breast adipose cell diameter positively correlated with inflammation markers and the senescent marker GLB1. (A–E) Correlation between breast adipose cell size and mRNA expression of the inflammation markers IL-6, IL-8, IL-1β, TNF-α and CCL2 (MCP-1) (n = 15), as well as (f): GLB1 in breast tissue (n = 15). mRNA expressions were normalized to endogenous control. Correlations were made using Spearman’s rank correlation. Spearman’s correlation coefficient r and p-values are indicated in the graphs.
Apart from the increased proinflammatory factors in large mammary adipose cells, we also examined if proliferative signaling was enhanced. As shown in Figure 3 (Supplement 3), phosphorylated mitogen-activated protein kinase (MAPK) increased in the adipose cells from large breasts. In the present study of non-obese women, we found cyclooxygenase 2 (COX2, also known as prostaglandin-endoperoxide synthase 2 [PTGS2]) to be markedly increased in the breast adipose tissue and strongly correlated with degree of inflammation (Figure 4). Taken together, we report that young non-obese women are characterized by large mammary adipose cells which are proinflammatory and express high levels of COX2. These data are consistent with an increased risk of developing breast cancer also in young and non-obese women.
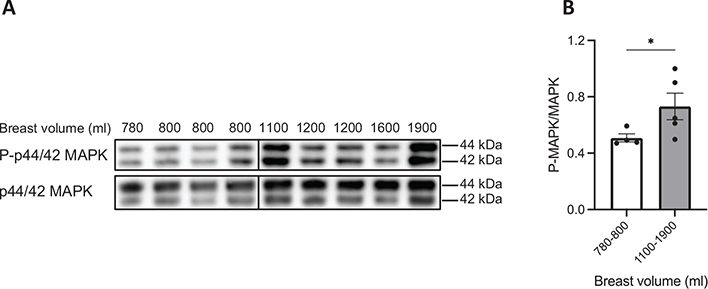
Figure 3. Increased proliferative signal in adipose cells with increased breast volume. (A) Western blots were performed with antibodies for P-MAPK and MAPK. (B) The ratio of phosphorylated to total MAPK (P-MAPK/MAPK) was calculated from images quantified using ChemiDoc imaging system. The relative expressions of the proteins are represented as mean ± SEM (n = 9). Significant difference was determined by Mann-Whitney test. *P < 0.05.
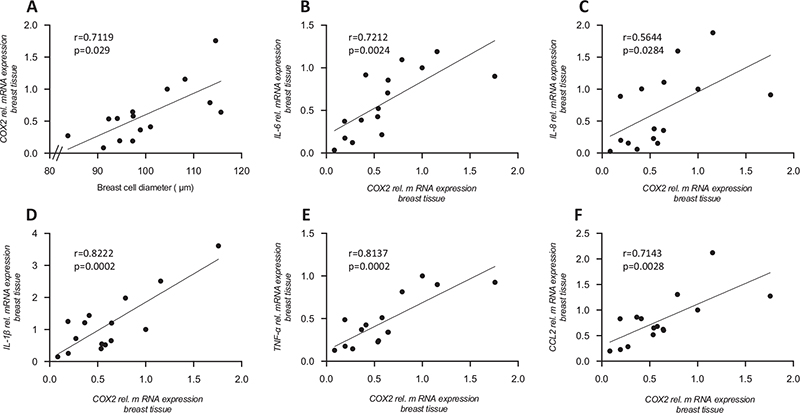
Figure 4. COX2 positively correlated with adipose tissue cell size and inflammation markers. (A) Correlation analysis between COX2 mRNA expression in breast tissue and breast cell diameter (n = 15). (B–F) Correlation between the mRNA expression of COX2 and the mRNA expression of the inflammation markers IL-6, IL-8, IL-1β, TNF-α and CCL2 (MCP-1) in breast tissue (n = 15). mRNA expressions were normalized to endogenous control. Correlations were made using Spearman rank correlation. Spearman’s correlation coefficient r and p-values are indicated in the graphs.
Discussion
This study investigates adipocyte cell size, proinflammatory markers and proliferative signaling in normal weight women with breast hypertrophy. The results point toward the fact that individuals with large breasts have expanded and pro-inflammatory adipose tissue cells characterized by an increased common marker of cell senescence and a high expression of COX2.
It is interesting to note that the breast adipose cells are larger than the subcutaneous cells in the vicinity and that breast size was an important determinant of this. In fact, the breast adipose cells were around 10% larger than the subcutaneous cells and characterized by markedly increased inflammation and β-galactosidase was also increased. β-galactosidase may contribute to the proinflammatory effect seen in large cells and the development of dysregulated and dysfunctional adipose cells [26].
Cell senescence is increased in large adipose cells [27]. It promotes inflammation and can lead to the increased inflammation in the large breast and subcutaneous adipose cells. We also found the phosphorylation of MAPK to be increased in the breast adipose cells, and this may also contribute to enhancing cell senescence and risk of cancer development [28]. The markedly increased COX2 in the breast adipose tissue and its strong correlation with degree of inflammation could also be associated with a risk of cancer development. A recent study found adipose cell size and expression of the prostaglandin regulator COX2 to be critical for the risk of developing breast carcinoma [29]. It was reported that hypertrophic adipose cells and increased COX2 were associated with 12-fold increase in risk of developing breast cancer [29]. Hence, an increased adipocyte cell size in large breast might explain the increased cancer risk in large breasted women [5, 6], as well as the previously seen increased mortality [6] and shorter disease-free and distant metastasis-free survival [7] in the group, supporting the theory that local adipose tissue characteristics play an important role in cancer development.
Methodologically, it should be emphasized that it is difficult to measure breast volume clinically with a high validity and reliability [30]. In this study, volume was measured with plastic breast cups, which is a well-established method that has been validated and reliability tested previously [31–34]. Nonetheless, the method is bound by some degree of subjectivity [31], like all methods to measure breast volume [30]. However, the volumes measured pre-operatively with the cups differ little from the volume measured from mastectomy specimens and seem to be more accurate than three-dimensional techniques and estimations using Magnetic Resonance Imaging [33]. Moreover, it is more objective and less subjective to variability than cup size [35], which has been used in many previous studies on breast volume [4]. Although the method to measure breasts in the study is not perfect, it is one of the most accurate clinical methods available and the degree of inter-rater variability (±50 ml) [31] should not have affected the overall results of the study.
Taken together, our results show that breast adipose tissue inflammation, cell hypertrophic enlargement, COX2 expression and proliferative signaling through MAPK activation are increased in these non-obese women with breast hypertrophy. This is consistent with an increased risk of breast cancer development seen in women with large breasts. Local characteristics of adipose tissue in the breast and its role in breast cancer development warrant further investigation.
Declarations
Ethics approval and consent to participate
The Regional Ethical Committee of Gothenburg reviewed and approved the study (559-18). The procedures followed were in accordance with the Helsinki declaration. The participants gave their informed consent to participate in this study.
Consent for publication
The participants gave their informed consent to the publication of the results.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Authors’ contributions
SG – formal analysis, data curation, investigation, methodology, project administration, resources, validation, visualization, writing – original draft.
AN - formal analysis, data curation, investigation, methodology, resources, validation, visualization, writing – review and editing.
US – conceptualization, formal analysis, funding acquisition, investigation, methodology, resources, validation, writing – original draft.
EH - conceptualization, funding acquisition, investigation, methodology, resources, writing – original draft.
Acknowledgements
We express our sincere gratitude to the patients who participated in the study. We thank Gudrun Knöll for excellent technical support.
References
[1] Lauby-Secretan B, Scoccianti C, Loomis D, et al. Body fatness and cancer – viewpoint of the IARC Working Group. N Engl J Med. 2016; 375(8): 794-798. https://doi.org/10.1056/NEJMsr1606602
[2] Arnold M, Leitzmann M, Freisling H, et al. Obesity and cancer: an update of the global impact. Cancer Epidemiol. 2016; 41: 8–15. https://doi.org/10.1016/j.canep.2016.01.003
[3] Brown N, White J, Milligan A, et al. The relationship between breast size and anthropometric characteristics. Am J Hum Biol. 2012; 24(2): 158–164. https://doi.org/10.1002/ajhb.22212
[4] Jansen LA, Backstein RM, Brown MH. Breast size and breast cancer: a systematic review. J Plast Reconstr Aesthet Surg. 2014; 67(12): 1615–1623. https://doi.org/10.1016/j.bjps.2014.10.001
[5] Kusano AS, Trichopoulos D, Terry KL, et al. A prospective study of breast size and premenopausal breast cancer incidence. Int J Cancer. 2006; 118(8): 2031–2034. https://doi.org/10.1002/ijc.21588
[6] Williams PT. Breast cancer mortality vs. exercise and breast size in runners and walkers. PLoS One. 2013; 8(12): e80616. https://doi.org/10.1371/journal.pone.0080616
[7] Markkula A, Bromee A, Henningson M, et al. Given breast cancer, does breast size matter? Data from a prospective breast cancer cohort. Cancer Causes Control. 2012; 23(8): 1307–1316. https://doi.org/10.1007/s10552-012-0008-9
[8] Eriksson N, Benton GM, Do CB, et al. Genetic variants associated with breast size also influence breast cancer risk. BMC Med Genet. 2012; 13: 53. https://doi.org/10.1186/1471-2350-13-53
[9] Avgerinos KI, Spyrou N, Mantzoros CS, et al. Obesity and cancer risk: emerging biological mechanisms and perspectives. Metabolism. 2019; 92: 121–135. https://doi.org/10.1016/j.metabol.2018.11.001
[10] Hovey RC, Aimo L. Diverse and active roles for adipocytes during mammary gland growth and function. J Mammary Gland Biol Neoplasia. 2010; 15(3): 279–290. https://doi.org/10.1007/s10911-010-9187-8
[11] Fletcher SJ, Sacca PA, Pistone-Creydt M, et al. Human breast adipose tissue: characterization of factors that change during tumor progression in human breast cancer. J Exp Clin Cancer Res. 2017; 36(1): 26. https://doi.org/10.1186/s13046-017-0494-4
[12] Pistone Creydt V, Fletcher SJ, Giudice J, et al. Human adipose tissue from normal and tumoral breast regulates the behavior of mammary epithelial cells. Clin Transl Oncol. 2013; 15(2): 124–131. https://doi.org/10.1007/s12094-012-0896-x
[13] Zhu Q, Zhu Y, Hepler C, et al. Adipocyte mesenchymal transition contributes to mammary tumor progression. Cell Rep. 2022; 40(11): 111362. https://doi.org/10.1016/j.celrep.2022.111362
[14] Wang YY, Lehuede C, Laurent V, et al. Adipose tissue and breast epithelial cells: a dangerous dynamic duo in breast cancer. Cancer Lett. 2012; 324(2): 142–151. https://doi.org/10.1016/j.canlet.2012.05.019
[15] Choi J, Cha YJ, Koo JS. Adipocyte biology in breast cancer: from silent bystander to active facilitator. Prog Lipid Res. 2018; 69: 11–20. https://doi.org/10.1016/j.plipres.2017.11.002
[16] Arner E, Westermark PO, Spalding KL, et al. Adipocyte turnover: relevance to human adipose tissue morphology. Diabetes. 2010; 59(1): 105–109. https://doi.org/10.2337/db09-0942
[17] Carter JM, Hoskin TL, Pena MA, et al. Macrophagic “Crown-like Structures” are associated with an increased risk of breast cancer in benign breast disease. Cancer Prev Res (Phila) 2018; 11(2): 113–119. https://doi.org/10.1158/1940-6207.CAPR-17-0245
[18] Cinti S, Mitchell G, Barbatelli G, et al. Adipocyte death defines macrophage localization and function in adipose tissue of obese mice and humans. J Lipid Res. 2005; 46(11): 2347–2355. https://doi.org/10.1194/jlr.M500294-JLR200
[19] Morris PG, Hudis CA, Giri D, et al. Inflammation and increased aromatase expression occur in the breast tissue of obese women with breast cancer. Cancer Prev Res (Phila) 2011; 4(7): 1021–1029. https://doi.org/10.1158/1940-6207.CAPR-11-0110
[20] Iyengar NM, Morris PG, Zhou XK, et al. Menopause is a determinant of breast adipose inflammation. Cancer Prev Res (Phila) 2015; 8(5): 349–358. https://doi.org/10.1158/1940-6207.CAPR-14-0243
[21] Iyengar NM, Brown KA, Zhou XK, et al. Metabolic obesity, adipose inflammation and elevated breast aromatase in women with normal body mass index. Cancer Prev Res (Phila) 2017; 10(4): 235–243. https://doi.org/10.1158/1940-6207.CAPR-16-0314
[22] Maliniak ML, Miller-Kleinhenz J, Cronin-Fenton DP, et al. Crown-like structures in breast adipose tissue: early evidence and current issues in breast cancer. Cancers (Basel) 2021 May 6;13(9):2222. https://doi.org/10.3390/cancers13092222
[23] Shaik AN, Kiavash K, Stark K, et al. Inflammation markers on benign breast biopsy are associated with risk of invasive breast cancer in African American women. Breast Cancer Res Treat. 2021; 185(3): 831–839. https://doi.org/10.1007/s10549-020-05983-x
[24] Abdiu A, Elander A, Gerdin B, et al. Bröstreduktionsplastik – bröstförminskade kirurgi vid stor byst. Rapport från expertgruppen för plastikkirurgi: Sveriges Kommuner och Landsting; 2008.
[25] Gustafson B, Nerstedt A, Spinelli R, et al. Type 2 diabetes, independent of obesity and age, is characterized by senescent and dysfunctional mature human adipose cells. Diabetes. 2022; 71(11): 2372–2383. https://doi.org/10.2337/db22-0003
[26] Rouault C, Marcelin G, Adriouch S, et al. Senescence-associated beta-galactosidase in subcutaneous adipose tissue associates with altered glycaemic status and truncal fat in severe obesity. Diabetologia. 2021; 64(1): 240–254. https://doi.org/10.1007/s00125-020-05307-0
[27] Ye RZ, Richard G, Gevry N, et al. Fat cell size: measurement methods, pathophysiological origins, and relationships with metabolic dysregulations. Endocr Rev. 2022; 43(1): 35–60. https://doi.org/10.1210/endrev/bnab018
[28] Singh V, Ram M, Kumar R, et al. Phosphorylation: implications in cancer. Protein J. 2017; 36(1): 1–6. https://doi.org/10.1007/s10930-017-9696-z
[29] Almekinders MMM, Schaapveld M, Thijssen B, et al. Breast adipocyte size associates with ipsilateral invasive breast cancer risk after ductal carcinoma in situ. NPJ Breast Cancer. 2021; 7(1): 31. https://doi.org/10.1038/s41523-021-00232-w
[30] Choppin SB, Wheat JS, Gee M, et al. The accuracy of breast volume measurement methods: a systematic review. Breast. 2016; 28: 121–129. https://doi.org/10.1016/j.breast.2016.05.010
[31] Hansson E, Manjer J, Ringberg A. Reliability of plastic cups to measure breast volume. J Plast Surg Hand Surg. 2014; 48(4): 254–258. https://doi.org/10.3109/2000656X.2013.870908
[32] Biorserud C, Fagevik Olsen M, Elander A, et al. Objective measurements of excess skin in post bariatric patients – inter-rater reliability. J Plast Surg Hand Surg. 2016; 50(2): 68–73. https://doi.org/10.3109/2000656X.2015.1089876
[33] Eriksen C, Lindgren EN, Olivecrona H, et al. Evaluation of volume and shape of breasts: comparison between traditional and three-dimensional techniques. J Plast Surg Hand Surg. 2011; 45(1): 14–22. https://doi.org/10.3109/2000656X.2010.542652
[34] Strombeck JO, Malm M. Priority grouping in a waiting list of patients for reduction mammaplasty. Ann Plast Surg. 1986; 17(6): 498–502. https://doi.org/10.1097/00000637-198612000-00011
[35] Ringberg A, Bageman E, Rose C, et al. Of cup and bra size: reply to a prospective study of breast size and premenopausal breast cancer incidence. Int J Cancer. 2006; 119(9): 2242–2243; author reply 2244. https://doi.org/10.1002/ijc.22104