ORIGINAL RESEARCH ARTICLE
Anatomical research and clinical application of multistage advancement in dorsal finger V-Y flap
Qiu Shenqianga, Wang Zengtaoa,*, Chen Jingguob, Zhang Dia, Sun Juna, Kou Weia,c, Hao Liwena and Xu Lanweia
aDepartment of Hand, Foot and Micro Reconstruction Surgery, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, Shandong, 250021, China; bDepartment of Orthopaedic Surgery, Third Hospital of Hebei Medical University, Shijiazhuang, Hebei, 050051, China; cDepartment of Hand and Foot Surgery, Guang’anmen Hospital Jinan China Academy of Chinese Medical Sciences, Jinan, Shandong, 250021, China
ABSTRACT
Objective: To investigate the anatomical basis and clinical efficiency of the advancement distance in dorsal digital V-Y advancement flap.
Materials and methods: Thirty-four fingers in 11 fresh adult hand specimen were selected, V-Y flap was performed with the digital artery as vascular pedicle, and the advancement distance was measured. The relationship between the distance and extensibility of skin, sliding degree of subcutaneous superficial fascia, angular displacement of digital arterial dorsal branch, elasticity of digital artery was discussed. Two cases were provided to demonstrate the feasibility and importance of this flap.
Results: In the dorsal digital V-Y advancement flap simulated on fresh adult hand specimens, the mean advance distance of the middle segment flap and proximal segment flap is 18 ± 0.8 mm and 34 ± 1.7 mm, respectively, and the maximum can reach 24 and 45 mm, respectively. Two cases of dorsal digital V-Y advancement flaps were designed and performed in the dorsal side of the ring finger middle segment and the thumb proximal segment, respectively. The advancement distances were 25 and 26 mm, respectively. All flaps survived completely and the incisions healed by first intention. The flap texture was good, the affected finger was symmetrical, and the activity and sensation restored well.
Conclusion: The dorsal digital V-Y advancement flap with the digital artery as the main vascular pedicle can exert four factors for advancement effect, and significantly increase the advancement distance. The operation is simple, the blood supply is reliable, and the postoperative sensation is normal. It is an ideal flap for repairing the digital dorsal defect.
KEYWORDS: Dorsal digital V-Y advancement flap; advancement distance; digital artery
Citation: Journal of Plastic Surgery and Hand Surgery 2024; 59: 132–140. DOI: https://doi.org/10.2340/jphs.v59.41373.
Copyright: © 2024 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 5 July 2024; Accepted: 9 August 2024; Published: 24 October 2024
CONTACT Wang Zengtao wzt@sdu.edu.cn Chief Physician, Department of Hand, Foot and Micro Reconstruction Surgery, Shandong Provincial Hospital Affiliated to Shandong First Medical University, No. 324 QingwuWeiqi Road, Jinan 250021, Shandong Province, China.
Competing interests and funding: The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The article is supported by Shandong Provincial Natural Science Foundation, No. No.ZR2021MH165 and Shandong Provincial Natural Science Foundation, No.ZR2022MH144.
Objective
The V-Y advancement flap is a classic surgical method for repairing finger defects. It can pull the skin with similar proximal characteristics to the distal wound. which is a simple operation with good sensory recovery and high success rate, and it is more common in the repair of ventral digital defects and fingertip defects [1–5]. However, the dorsal digital V-Y advancement flap is rare, which may be related to the limited advancement distance [6]. To this end, we designed a dorsal digital V-Y advancement flap with the digital artery as the main vascular pedicle, utilizing the linkage superimposition of four factors: the extensibility of skin, sliding degree of subcutaneous superficial fascia, angular displacement of digital arterial dorsal branch and elasticity of digital artery, to form a ‘multistage linkage’ similar to a multi-stage sliding door, which greatly increases the advancement distance. In this article, we report the anatomical study and clinical application of the dorsal digital V-Y advancement flap. The anatomical part studies four factors: the ductility of the skin, the sliding degree of the subcutaneous superficial fascia, the angular displacement of the dorsal branch of the finger artery and the elasticity of the finger artery, and we measure the advancement distance to the distal end. Two cases were provided to demonstrate the application of this flap.
Materials and methods
Materials
Eleven fresh adult hand specimens were perfused with red latex through the artery, and then placed in a refrigerator at -30°C for 3–4 days until the latex was completely solidified. The dorsal digital V-Y advancement flap was designed and performed in the thawed finger, including 6 index fingers, 9 middle fingers, 10 ring fingers and 9 little fingers.
Methods
Flap design
The dorsal digital V-Y advancement flap was designed and simulated in the middle and proximal segments of the finger. This experiment only explores the advancement distance of the flap, so the shape of the proximal edge of the flap was not specifically designed.
- The dorsal flap of the middle segment (Figure 1A): the junction of the ventral and dorsal skin of the finger was designed as the bilateral edges of the flap, the median line of the dorsal transverse striations of the distal and proximal interphalangeal joints was designed as the distal and proximal edges of the flap, respectively.
- The dorsal flap of the proximal segment (Figure 2A): the junction of the ventral and dorsal skin of the finger was designed as the bilateral edges of the flap, the median line of the dorsal transverse striations of the proximal interphalangeal joint was designed as the distal edge of the flap, and the proximal edge of the flap was located at the dorsal metacarpophalangeal joint.
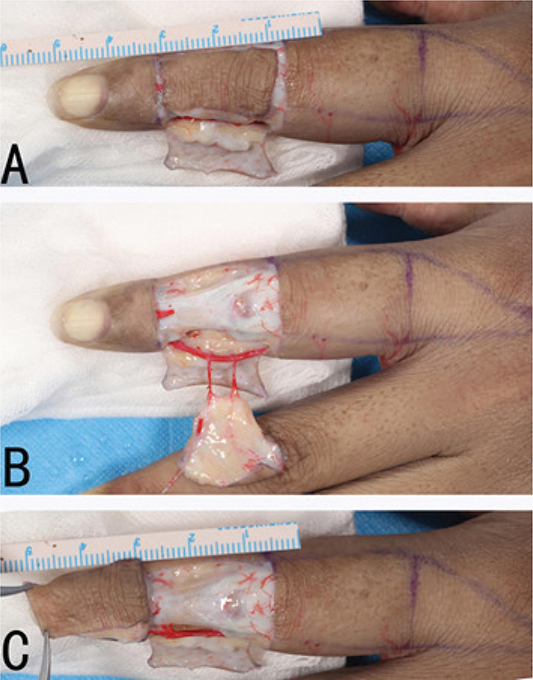
Figure 1. Multistage dorsal digital V-Y advancement flap of the middle segment. (A) Design of the flap; (B) Incision of the flap; (C) Pull the flap to the distal end.
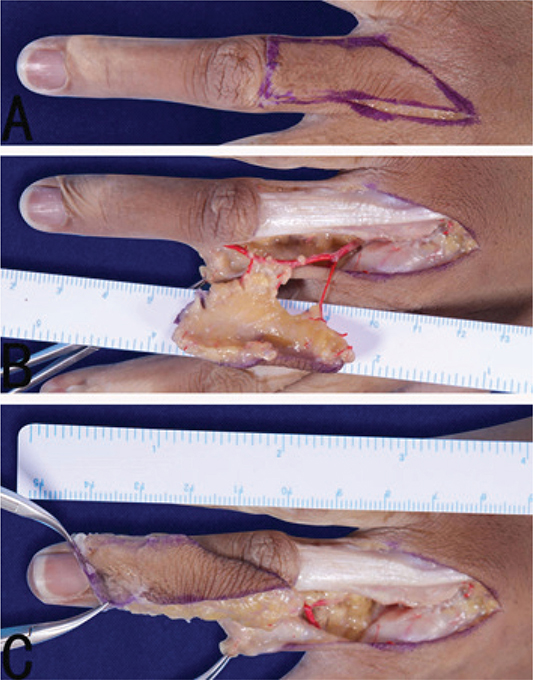
Figure 2. Multistage dorsal digital V-Y advancement flap of the proximal segment. (A) Design of the flap; (B) Incision of the flap; (C) Pull the flap to the distal end.
Flap cutting
The index and middle fingers’ flaps use the ulnar digital artery as the main vascular pedicle, while the ring and little fingers’ flaps use the radial digital artery as the main vascular pedicle.
Take the ring finger as an example, the radial digital artery is the main vascular pedicle. Firstly, the radial incision of the ring finger was incised, and the dissection was performed between the dermis and the superficial fascia to expose the digital artery and nerve in the ventral side of the finger. Then the skin and superficial fascia at the ulnar, proximal and distal edges of the flap were incised, the extensor tendon was freed to the radial side of the finger from the superficial side of the extensor tendon to the radial side of the finger, and continued to be freed to the palm side between the superficial fascia and the periosteum or the peritendinous membrane until it was close to the flexor tendon sheath and separated from the ulnar side of the digital artery and nerve. The dorsal branch of the digital artery and its surrounding superficial fascia were retained, and the digital artery and nerve were separated to form a dorsal digital V-Y advancement flap with the radial digital artery and its dorsal branch as the main vascular pedicle (Figures 1B and 2B).
Measurement of finger length and advancement distance of the flap
Finger length: straighten the finger, measure the length from the finger root transverse striation to the fingertip.
Advancement distance of the flap: the dorsal digital flap was pulled to the distal end, then the advancement distance of the distal edge of dorsal digital flap was measured by a ruler (Figures 1C and 2C).

Calculation of advancement ratio: advancement ratio refers to the ratio of the advancement distance of the flap to the corresponding finger length, the calculation formula is as follows:
Results
The length of each finger, the advancement distance of each flap, and corresponding advancement ratio are shown in Table 1. The mean advancement distance of the proximal flap was significantly greater than that of the middle flap and there was a significant difference between them (p < 0.05).
Typical cases
Typical case 1
The patient was a 55-year-old female. The wound on the of the ring dorsal side finger caused by cable crush was accompanied by exposed tendon (Figure 3A). At first, the patient underwent one-stage debridement due to inaccurate blood supply of skin contusion. The wound was covered with VSD and the avulsed skin was retained. After 6 days, the non-vascularized skin was removed, and a 2.6 × 3.0 cm wound was formed on the ring finger dorsal side. A 6.8 × 2.5 cm dorsal digital V-Y advancement flap was designed on the ring finger proximal segment (Figure 3B). The skin was first cut along the designed incision to the subcutaneous tissue layer (Figure 3C). The proximal flap was separated from the ulnar side of the metacarpophalangeal joint of the middle finger at the proximal end of the flap. The finger web artery was carried to the flap, and then separated from the subcutaneous tissue of the ulnar side of the flap and the superficial layer of the extensor tendon to the radial side. The ulnar side of the digital nerve and its dorsal branch of the digital artery was separated from the phalanx to the palm side and the flap was obtained after converging with the digital artery and the palm side of the nerve. The digital nerve and the digital artery were properly separated under the microscope, but their branches to the flap were preserved. The anastomosis branch of the finger webbing artery to the dorsal metacarpal artery was ligated, and the continuity of the superficial vein and the cutaneous nerve at the proximal end of the flap was preserved (Figure 3E). The ulnar digital artery of the middle finger and the common digital artery of the middle ring were dissected and separated. When the flap was pulled to the distal end, the radial digital artery of the ring finger was pulled to the distal end, and the common digital artery of the proximal end and the ulnar digital artery of the middle finger were also pulled to the distal end (Figure 3G). After the flap was sutured, in order to prevent the influence of postoperative finger movement on the flap, the interphalangeal joint of the ring finger was temporarily fixed with a Kirschner wire. The flap advanced 26 mm forward, covering the wound well and having good blood supply (Figure 3H and 3I). The Kirschner wire was removed 2 weeks after operation and functional exercise was started. The appearance of the flap was good at 3 months after operation, and the two-point discrimination was 6 mm, which was consistent with the contralateral ring finger (Figure 3J and 3K).

Figure 3. Typical case 1, a 55-year-old female, dorsal digital V-Y advancement flap on the dorsal ring finger middle segment. (A) Wound surface on the dorsal ring finger middle segment; (B) Preoperative flap design; (C) Skin flap separated into subcutaneous tissue layer; (D) Separation of the flap to the palmar digital nerve; (E) Flap retaining digital artery, superficial vein and cutaneous nerve; (F) The tractive flap shows tortuosity of the digital artery; (G) All three arteries pulled distally when the flap is pulled; (H and I): Postoperative ring finger blood supply; (J and K) follow-up at 3 months after surgery.
Typical case 2
A 52-year-old male patient was operated in a local hospital after the machine crush injury of the right thumb. The index finger was amputated and the dorsal wound of the thumb was exposed with tendon. The artificial skin was used to cover the proximal wound of the thumb. More than 50 days after the operation, he came to our hospital for treatment due to poor healing of the thumb wound (Figure 4A). Preoperative CTA examination was used to evaluate the vascular condition of the thumb (Figure 4B, 4C, and 4D). The dorsal digital V-Y advancement flap of the thumb was designed before operation (Figure 4E). The wound area was 3.0 × 2.5 cm, and the flap area was 6.0 × 3.2 cm. The flap was cut from the radial side and separated from the ulnar side of the extensor tendon. The perforating branch from the main artery of the thumb to the flap was retained (Figure 4F), and then separated from the ulnar side of the flap to the radial dorsal side of the second metacarpal. The superficial vein and superficial fascia layer of the first web area were connected to the flap to ensure better blood supply (Figure 4G). The proximal end of the flap retained the continuity of the superficial fascia and the superficial branch of the radial nerve (Figure 4H), and the flap was lifted. A V-Y flap pedicled with the main artery of the thumb and its cutaneous branches and the ulnar digital artery of the thumb was formed (Figure 4I). The flap was pulled 25 mm to the distal end, and the skin was sutured. The blood supply of the flap was good (Figure 4J). After half a year of follow-up, it was found that the flap survived well and the shape and sensation were good (Figure 2K). The two-point discrimination of the flap was 5 mm, which was consistent with the dorsal skin of the contralateral thumb.
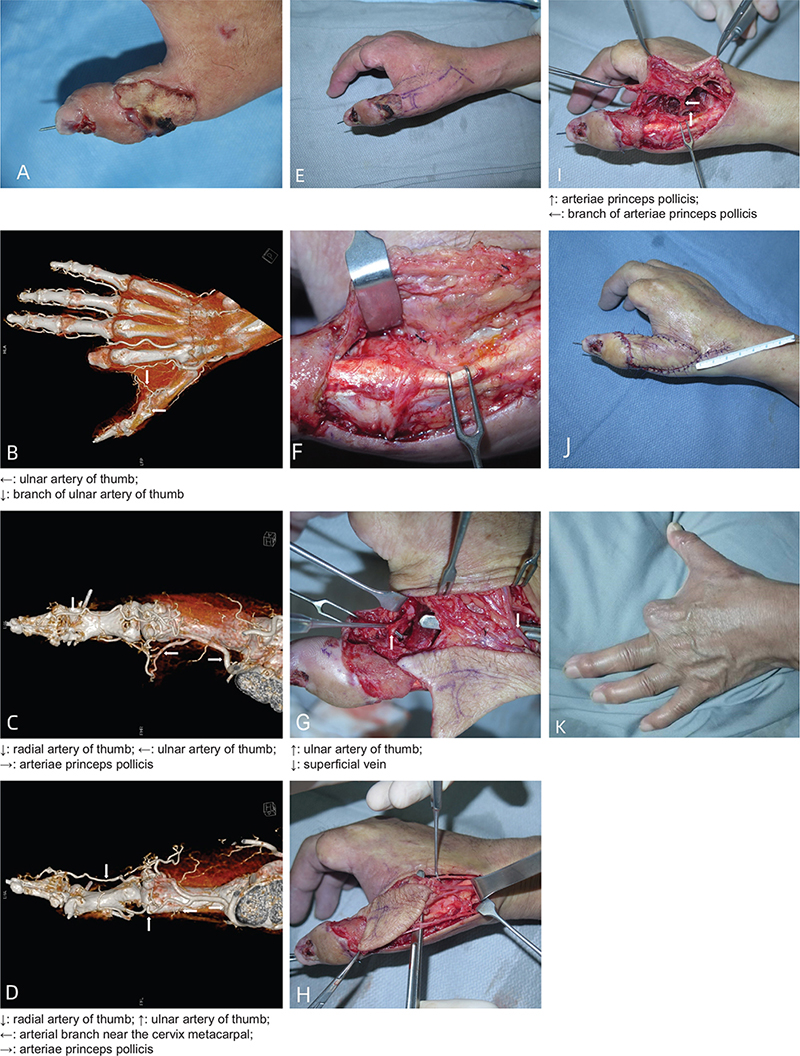
Figure 4. Typical case 2: a 52-year-old man with a dorsal digital V-Y advancement flap on the dorsal thumb proximal segment. (A) The proximal joint wound of the thumb was covered by artificial skin. (B, C, and D) Thumb vascular condition; (E) Preoperative flap design; (F) Perforating branch of major thumb artery; (G) The skin flap carries superficial veins and superficial fascia layer in the first web area; (H) Superficial fascia and superficial branch of radial nerve were retained at the proximal end of the flap. (I) V-Y flap with main thumb artery and its cutaneous branch and ulnar finger artery as vascular pedicle; (J) Postoperative blood supply of thumb; (K) 9-month follow-up.
Discussion
Anatomical research: the principle of multistage linkage advancement
The maximum flap advancement distance is mainly reflected in the flap distal edge advancement distance. On the basis of previous anatomical studies, we believe that the flap advancement distance will be affected by four factors, including extensibility of skin, sliding degree of subcutaneous superficial fascia, angular displacement of digital arterial dorsal branch and elasticity of digital artery. Moreover, the contribution of the angular displacement of digital arterial dorsal branch and elasticity of digital artery to the advancement distance are much larger than that of extensibility of skin, sliding degree of subcutaneous superficial fascia.
- Extensibility of skin: Cut the distal and bilateral margins of the skin, when the skin is pulled by a certain tension, the extensibility of skin can be utilized to pull the flap distal margin to a certain distance (Figure 5).
- Sliding degree of subcutaneous superficial fascia: the subcutaneous superficial fascia on the dorsal finger is loose, incise skin around the flap, and the flap advancement distance can be increased by utilizing the sliding degree of subcutaneous superficial fascia (Figure 6).
- Angular displacement of digital arterial dorsal branch: the digital artery sends a cutaneous branch to the dorsal side, and the angle can be close to 90°. When the flap pulled distally, this angle becomes smaller and even close to 0°. After the angular displacement, the vertical distance from the dorsal branch to the dorsal finger became to the distal end, which increased the flap advancement distance (Figure 7).
- Elasticity of digital artery: after the digital artery is pulled, the flap advancement distance is further increased; the longer the free digital artery, the greater the available elasticity of blood vessels, and the greater the flap advancing distance (Figure 8).
The dorsal digital V-Y advancement flap is essentially achieved by reducing the skin circumference to ‘fill the length with width’ [7]. The traditional finger dorsal digital V-Y advancement flap retains the subcutaneous fascia pedicle, doesn’t cut the digital artery trunk and dorsal branch, mainly uses the extensibility of skin and the sliding degree of subcutaneous superficial fascia to pull flap to the wound. In order to avoid excessive traction, its advancement distance is quite limited, so the clinical practice of dorsal digital V-Y advancement flap is rare [8]. In order to make better use of angular displacement of digital arterial dorsal branch and elasticity of digital artery, our team retained the dorsal branch of digital artery and used its angular displacement to change the vertical distance of the dorsal branch to the dorsal finger into the distance to the distal end. Then dissociate the digital artery, cut off the remaining branches except dorsal branch, and use its elasticity to further increase the advancement distance. Therefore, the dorsal digital V-Y advancement flap with the digital artery as the main vascular pedicle designed by our team makes full use of four factors (extensibility of skin, sliding degree of subcutaneous superficial fascia, angular displacement of digital arterial dorsal branch and elasticity of digital artery), which is similar to the multistage sliding door, forming a multilevel superimposition effect, which can significantly increase the flap advancement distance (Figure 9), cover a larger wound area, and expand the application range of the dorsal digital V-Y advancement flap.

Figure 5. Extensibility of skin: (A) before skin pulling, (B) after skin pulling, (a) V-Y flap, (1) original length of the flap, (2) increased length after skin pulling.

Figure 6. Sliding degree of subcutaneous superficial fascia: (A) before subcutaneous superficial fascia sliding, (B) after subcutaneous superficial fascia sliding, (a) V-Y flap, (b) subcutaneous superficial fascia, (1) original length of the flap, (2) increased length after skin pulling, (3) distance of subcutaneous superficial fascia sliding.
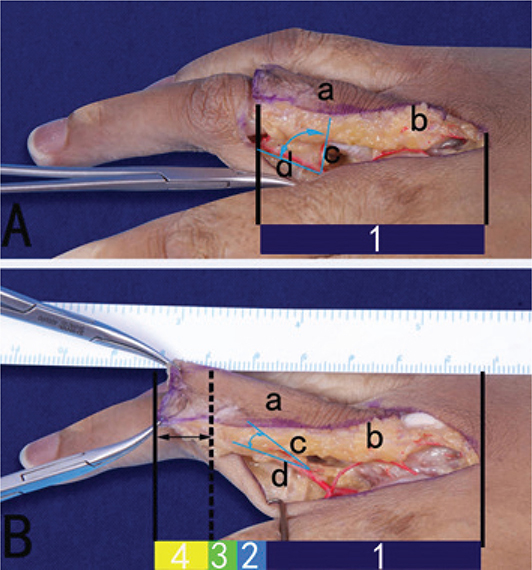
Figure 7. Angular displacement of digital arterial dorsal branch: (A) digital arterial dorsal branch before angular displacement, (B) digital arterial dorsal branch after angular displacement, (a) V-Y flap, (b) subcutaneous superficial fascia, (c) digital arterial dorsal penetrating branch, (d) digital artery, (1) original length of the flap, (2) increased length after skin pulling, (3) distance of subcutaneous superficial fascia sliding, (4) increased length by angular displacement of digital arterial dorsal branch.
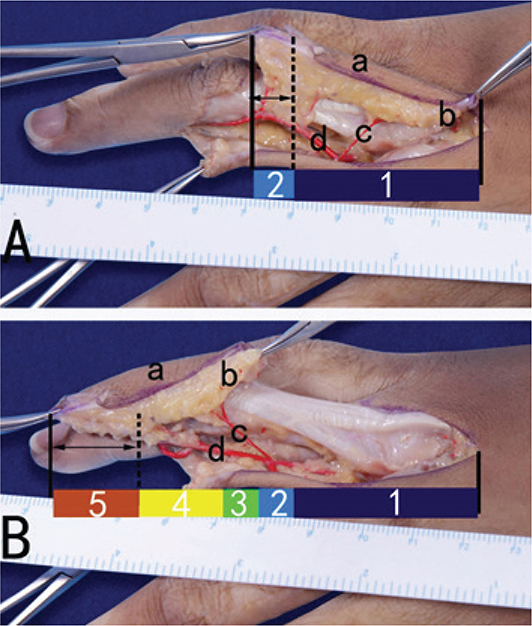
Figure 8. Elasticity of digital artery: (A) digital arteries before pulling, (B) digital arteries after pulling, (a) island flap, (b) superficial subcutaneous fascia, (c) dorsal branch, (d) finger arteries, (1) original length of the flap, (2) increased length after skin pulling, (3) distance of subcutaneous superficial fascia sliding, (4) increased length by angular displacement of digital arterial dorsal branch, (5) increased length using elasticity of digital artery.
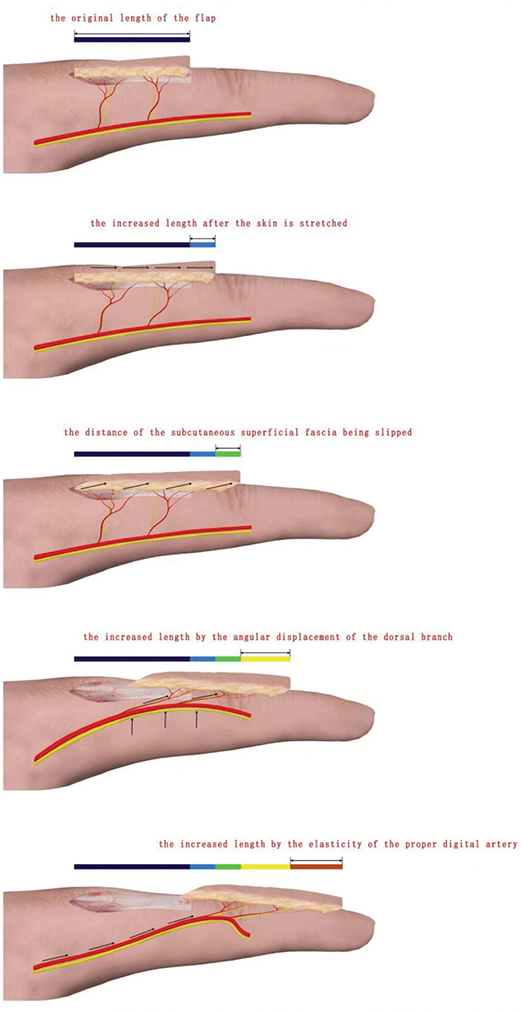
Figure 9. Principal mode of multistage dorsal digital V-Y advancement flap.
In this study, the mean advancement distance of the middle segment dorsal digital V-Y advancement flap was 18 ± 0.8 mm, and the mean advancement distance of the proximal segment dorsal digital V-Y advancement flap was 34 ± 1.7 mm. There was a significant difference between them. The contribution of the angular displacement of digital arterial dorsal branch to the flap advancement distance mainly depends on 2 factors: firstly, the effective length of the dorsal branch pedicle, that is, the distance from the digital arterial starting point to the flap lateral edge; secondly, the degree of angular displacement. In the case of similar angular displacement degree, the flap advancement distance is positively correlated with the effective length of dorsal branch pedicle. Therefore, the lateral margin of the flap should be kept away from the digital artery pedicle as far as possible, so as to increase the effective length of the dorsal branch pedicle as far as possible, so as to increase the advancing distance caused by angular displacement. In anatomical study, we found that the dorsal branch of the proximal segment V-Y flap was longer. In addition, compared with the middle segment V-Y flap, the proximal segment V-Y flap has greater sliding degree of subcutaneous superficial fascia and its advancement distance will be larger. Therefore, the mean advancement distance of the proximal segment dorsal digital V-Y advancement flap is much larger than that of the middle segment.
Since the branch of the digital artery will limit the flap advancement distance, it is necessary to cut off other branches except dorsal branch. The elasticity of the proper digital nerve and its branches is less than that of the digital artery and its branches, so the nerve carried by the vascular pedicle will reduce the flap advancement distance. However, the nerve tissue protects the blood vessels from excessive traction and also contributes to the recovery of postoperative sensory function. Therefore, on the basis of sufficient flap advancement distance to cover the wound, we recommend carrying the nerve as much as possible.
Clinical applications
From the perspective of clinical application, the dorsal digital V-Y advancement flap conforms to the principle of ‘like-with-like’ [9,10] when repairing finger wounds, and can achieve both function and appearance [11], with the following advantages:
- The flap carries unilateral digital artery, with reliable blood supply, high survival rate, and doesn’t affect the blood supply of the finger itself. Due to the protection of the superficial fascia layer between the finger artery and the flap, the blood supply of the flap is still stable even if a greater force is given. The digital artery usually has two accompanying veins, which are slender but sufficient to ensure the venous return of the flap.
- This method does not require complex microsurgical operation, only involves the superficial fascia layer, and does not need to anastomose the blood vessels and nerves under the microscope, and the operation time is short; the accompanying veins of the digital artery are close to the digital artery, so they are not easy to be damaged when separating the digital artery and nerve. These advantages are helpful for the promotion of this operation in outpatient, emergency and primary hospitals, to save medical costs and reduce the burden on patients.
- The sensory function of the flap is good. The flap carries the dorsal cutaneous nerve and can also advance a certain distance without cutting off its proximal end. The branches of the digital nerve to the dorsal side of the finger are also separated (the branches of the nerve are dissected to the proximal end and separated from the trunk) and retained to the flap, so the sensation of the flap is close to normal after operation. At the same time, the nerve trunk and its branches to the ventral side remain intact, so the sensory damage to the finger body is minimized.
- The flap can provide sufficient amount of subcutaneous soft tissue and a soft soft tissue bed, which is extremely important for finger function. Through wound dressing, the wound can achieve scar healing, but it is possible to form bone-sticking scars, causing discomfort such as tenderness [12,13]; skin grafting can also cover the wound, but may damage other parts of the patient’s body and increase the burden on the patient.
- The V-Y flap increases the length by decreasing the circumference. The dorsal digital V-Y advancement flap can make full use of the loose characteristics of the proximal skin, so that the diameter of the finger changes evenly to the distal end with the V-Y advancement of the flap, which is more symmetrical. At the same time, the texture and color of the flap are similar to those of the recipient area, which makes the finger more aesthetically pleasing.
In the two typical cases, the flap advancement distances were 25 and 26 mm, respectively, which exceeded the upper limit of the traditional V-Y flap advancement distance (approximately 20 mm). All flaps survived after operation, and there were no postoperative complications such as vascular crisis, flap infection, flap necrosis, and so on. The wounds of all patients healed in the first stage, and the texture and appearance of the flaps were good. The flap had good sensation, and the two-point discrimination was 5 and 6 mm, respectively, which was consistent with the healthy side. The flexion and extension range of motion was not significantly reduced compared with that before operation. All patients were satisfied with the surgery efficacy.
Conclusion
The advancement distance of the multistage dorsal digital V-Y advancement flap is significantly increased. Because the digital artery (constant blood vessel) is the main vascular pedicle, the blood supply of the flap is stable. At the same time, because the flap carries nerve tissue, the postoperative sensory recovery is good. The operation is safe and simple, and it is an ideal choice for repairing small and medium-sized wounds on the dorsal side of the finger.
Defect and deficiency
- In this study, the force of pulling the flap was uneven, because the flap was pulled by the appropriate force applied by hand with experience. Therefore, the data are slightly rough, but they can still be used as a reference.
- Four factors affect the advancement distance at the same time. This study only analyzes the total advancement distance. The specific influence of each factor on the advancement distance is unclear and needs to be further explored.
- The multistage dorsal digital V-Y advancement flap cannot reconstruct the nail.
Consent statement
Written consent was obtained from the patients for the purpose of publication of case details and images.
Institutional review board statement
The study was reviewed and approved by the Biomedical Ethic Committee of Shandong Provincial Hospital (Approval No. 2021-018).
Author contributions
Wang Zengtao and Qiu Shenqiang designed the research study; Qiu Shenqiang, Chen Jingguo, Zhang Di, Kou Wei, Hao Liwen and Xu Lanwei performed the research; Chen Jingguo, Zhang Di and Sun Jun analyzed the data; Qiu Shenqiang, Chen Jingguo and Sun Jun wrote the manuscript.
References
[1] Tranquilli-Leali E. Ricostruzione dell’apice delle falangi ungueali mediante autoplastica volare peduncolata per scorrimento. Infort Traumatol Lav. 1935;1:186–193.
[2] Geissendorf H. Beitrag zur Fingerkuppenplastik. Zentraibl Chir. 1943;70:1107–1108.
[3] Kutler W. A new method for finger tip amputation. JAMA. 1947;133:29–30. doi: https://doi.org/10.1001/jama.1947.62880010007007
[4] Segmuller G. Modifikation des Kutler-Lappens: neuro-vaskuläre Stielung [Modification of the Kutler flap: neurovascular pedicle]. Handchirurgie. 1976;8(2):75–76. [German]
[5] Venkataswami R, Subramanian N. Oblique triangular flap: a new method of repair for oblique amputations of the fingertip and thumb. Plast Reconstr Surg. 1980;66(2):296–300. doi: https://doi.org/10.1097/00006534-198008000-00026
[6] Ozyigit MT, Turkaslan T, Ozsoy Z. Dorsal V-Y advancement flap for amputations of the fingertips. Scand J Plast Reconstr Surg Hand Surg. 2007;41:315–319. doi: https://doi.org/10.1080/02844310701463357
[7] Deal DN, Barnwell J, Li ZY. Soft-tissue coverage of complex dorsal hand and finger defects using the turnover adipofascial flap. J Reconstr Microsurg. 2011;27(2):133–138. doi: https://doi.org/10.1055/s-0030-1268852
[8] Kawakatsu M, Ishikawa K. Dorsal digital perforator flap for reconstruction of distal dorsal finger defects. J Plast Reconstr Aesth Surg. 2010;63(1):e46–e50. doi: https://doi.org/10.1016/j.bjps.2009.05.014
[9] Jin XL, Chung KC. V-Y Advancement, thenar flap, and cross-finger flaps. Hand Clin. 2020;36(1):19–32. doi: https://doi.org/10.1016/j.hcl.2019.08.003
[10] Foo TL, Wan HM. Modification of V-Y flap to preserve fingertip contour. Hand. 2012;7(4):388–390. doi: https://doi.org/10.1007/s11552-012-9451-z
[11] Tellioglu AT, Sensoz O. The dorsal branch of the digital never: an anatomic study and clinical applications. Ann Plast Surg. 1998;40(2):145–148. doi: https://doi.org/10.1097/00000637-199802000-00007
[12] Dölen UC, Koçer U. Innovation in the planning of V-Y rotation advancement flaps: a template for flap design. Arch Plast Surg. 2018;45(1):85–88. doi: https://doi.org/10.5999/aps.2017.00171
[13] Lim JX, Chong AKS, Sebastin SJ. Maximal advancement of homodigital neurovascular island flaps. J Hand Surg Eur Vol. 2019;44(10):1008–1012. doi: https://doi.org/10.1177/1753193419865894