ORIGINAL RESEARCH ARTICLE
Translation and validation of the Swedish version of the Appearance Schemas Inventory-Revised and investigation of the modified three subscale structure in patients undergoing breast reconstruction
Linn Weick, MAa,b, Carolina Lunde, PhDc and Emma Hansson, MD, PhDa,b
aDepartment of Plastic Surgery, Institute of Clinical Sciences, The Sahlgrenska Academy, Gothenburg University, Gothenburg, Sweden; bDepartment of Plastic Surgery, Region Västra Götaland, Sahlgrenska University Hospital, Gothenburg, Sweden; cDepartment of Psychology, University of Gothenburg, Gothenburg, Sweden
ABSTRACT
Breast cancer can lead to changes in appearance and subsequent concerns about body image. This study aimed to translate the body investment instrument, Appearance Schemas Inventory-Revised (ASI-R), to Swedish, and perform a validation in women who underwent mastectomy and were awaiting breast reconstruction. The instrument was translated, and its psychometric properties were investigated according to current guidelines. Three hundred and ninety-seven women were eligible for the study, and 215 (54%) participants responded. An exploratory factor analysis (EFA) revealed that a three-factor structure was the most adequate solution. Three new subscales were suggested: body image investment cognition; breast and body image investment emotions; breast reflecting dysfunctional cognitive and emotional patterns of appearance investment and body image investment behaviors; breast reflecting positive ways of investing in body image. Consistent with previous findings, control over appearance is a central theme in women with breast cancer undergoing mastectomy and reconstruction. The obtained factor structure was considered similar to the original structure and three-factor solutions obtained from an American cohort of patients with breast cancer. The ASI-R has shown good psychometric properties in Swedish women undergoing mastectomy and reconstruction. Further studies on convergent validity and confirmatory factor analysis are required.
KEYWORDS: Body image; breast cancer; breast reconstruction; validation; reliability; ASI-R
Citation: Journal of Plastic Surgery and Hand Surgery 2024; 59: 153–161. DOI: https://doi.org/10.2340/jphs.v59.42324.
Copyright: © 2024 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 18 June 2024; Accepted: 21 October 2024; Published: 27 November 2024
CONTACT Emma Hansson emma.hansson.2@gu.se Department of Plastic Surgery, Sahlgrenska University Hospital, Gröna Stråket 8, SE-413 45 Gothenburg, Sweden
Competing interests and funding: The authors declare no conflicts of interest.
This work was supported by The Swedish Cancer Society [21 0279 SCIA] (EH) and the federal government under the ALF agreement [ALFGBG-965161] (EH). Funding sources played no role in the study design, data collection, analysis, interpretation, or writing of the manuscript.
Introduction
Breast cancer and its treatment can lead to changes in the physical appearance that can negatively influence an individual’s body image [1]. Many breast cancer survivors experience body image distress following treatment [2]. However, the relationship between changes in physical appearance owing to cancer, cancer treatment, and body image is complex [3].
Breast reconstruction after mastectomy is performed principally to improve patients’ quality of life (QoL) and body image [4]. However, its actual effect on body image is unclear [5], and many patients still have body image problems several years after breast cancer despite reconstruction [6]. It has been highlighted that body image should be regarded as a primary outcome when evaluating women’s experiences of breast reconstruction, in addition to QoL and patient satisfaction [7]. Body image is also related to several psychosocial core outcomes established for reconstructive breast surgery: overall breast-specific QoL, normality, cosmetic satisfaction (core items for both patients and professionals), self-esteem, emotional well-being, and physical well-being (core items for patients alone) [8]. However, there is no ‘gold standard’ for assessing body image in patients with breast cancer, and different instruments have been used in previous studies [9–11]. Moreover, there is a paucity of validated instruments measuring the dimension of body image investment in the patient group [7, 12–15].
Body image investment constitutes a central dimension of body image attitudes. Body image investment involves the importance of one’s body for self-evaluation [16]. This construct is regarded as a moderating variable for the psychological effects of body image evaluation [17]. It has been conceptualized in a theoretical model of body image among cancer patients as a construct that predisposes them to poor psychological adjustment when experiencing changes in physical appearance [15]. High body image investment predicts body image dissatisfaction [13] and moderates the relationship between body image concerns and psychological distress [18].
One widely used instrument that has been used to measure body image investment in different populations is the Appearance Schemas Inventory-Revised (ASI-R) [14]. The factor structure and psychometric properties of the ASI-R in patients with breast cancer undergoing reconstruction were examined in a previous study [12]. The results differed from the original two-factor solution of the Self-Evaluative Salience (SES) and Motivational Salience (MS) subscales [19], as a three-factor solution was suggested: Appearance Self-Evaluation, which measures an individual’s preoccupation and negative self-evaluation with their appearance; Appearance Standards and Behaviors, which measures an individual’s level of standard and appearance management; and Appearance Power/Control, which measures the extent to which appearance is essential for the individual’s identity, and to what extent it affects the individual’s perceived control of their emotions, thoughts, and behaviors [12]. In brief, the Appearance Self-Evaluation Scale is similar to the original SES subscale, and the Appearance Standards and Behaviors scale is similar to the original MS subscale. In contrast, the Appearance Power/Control scale appeared to be unique to patients with breast cancer undergoing breast reconstruction. Chua et al. concluded that Appearance Power/Control scale may be of special relevance to patients with breast cancer because it reflects their lack of control over appearance changes due to the breast cancer and its treatment, and breast reconstruction might become a way to gain some perceived control [12]. The three-factor structure of patients was not evaluated beyond the initial study.
This study aimed to translate and perform a psychometric evaluation of the ASI-R in Swedish patients who underwent mastectomy, and to investigate the factor structure in patients with breast cancer awaiting breast reconstruction, that is, women who are currently unilaterally or bilaterally without breast. The validation could be a first step towards a ‘gold standard’ for assessing body image in patients with breast cancer.
Material and methods
Study design, protocol, and ethics
This cross-sectional study described the effects of expectations and body image on the breast reconstruction protocol (Clinicaltrials.gov identifier NCT04714463). This study was reviewed and approved by the Swedish Ethical Review Authority (2020-06245). The procedures in this study followed the principles of the Declaration of Helsinki, and all participants provided written informed consent to participate in the study and for the publication of the results. Use of ASI-R, authored by Professor Thomas F. Cash, was obtained under license from Body Images (www.body-images.com), Naples, Florida, USA. Permission to translate and validate the questionnaire was obtained from the participants.
Setting
This study was conducted at the Department of Plastic and Reconstructive Surgery, Sahlgrenska University Hospital, Gothenburg, Sweden. The department performs approximately 350–400 breast reconstructions annually. The Swedish healthcare system is a publicly funded welfare system.
Participants
The participants were identified using the department’s operational planning program. Hence, convenience sampling was used in this study. Inclusion criterion was women aged >18 years on the waiting list for delayed breast reconstruction after mastectomy due to breast cancer. Therefore, all the women who answered the questionnaire had one or two breasts missing. All the participants fulfilled the criteria for breast reconstruction according to the Swedish guidelines (body mass index ≤30 kg/m2 and the American Society of Anesthesiologists classification [ASA] ≤2) [20]. Exclusion criteria were inability to provide informed consent, failure to understand Swedish, and metastasized breast cancer.
Procedures
The patients were sent information about the study, consent forms, and questionnaires. Two reminders were sent after 2 and 4 weeks. After the patients provided informed consent, eligibility was checked, and the patients were included. Clinical background information was collected from medical charts. The first 49 patients who answered the questionnaire received it a second time after 2 weeks.
Instruments
The ASI instrument was developed to assess individuals’ beliefs about the importance of appearance and its influence on their life [21]. Later, an abbreviated version of the instrument was developed, the ASI-R [19]. The ASI-R has 20 items, and respondents rate their answers on a five-point Likert scale, including ‘strongly disagree’, ‘disagree’, ‘neither agree nor disagree’, ‘agree’, and ‘strongly agree’, and contra-worded items are scored in reverse. The instrument’s manual for scoring and data treatment was followed [22]. The composite scale and each subscale are calculated as the mean of the items on each scale. Higher scores indicate stronger body image investment [22]. The instrument does not have any cut-off values [22]. Originally, two subscales were suggested for the instrument: SES, comprising 12 items, and MS, comprising eight items (Table 1). SES refers to an individual’s beliefs about the importance of appearance and its effect on self-worth, whereas MS reflects the management of appearance [14, 19]. For patients with breast cancer undergoing breast reconstruction, three subscales have been suggested: Appearance Self-Evaluation, Appearance Standards and Behaviors, and Appearance Power/Control [12] (Table 1).
| Study | Factor analysis Method Results |
| American original version [19] | Factor 1. Self-Evaluative Salience (SES) Items 2, 5, 7, 8, 9, 11, 13, 14, 15, 16, 19, and 20 Factor 2. Motivational Salience (MS) Items 1, 3, 4, 6, 10, 12, 17, and 18 |
| American women with breast cancer undergoing mastectomy and reconstruction [12] | Factor 1. Appearance Self-Evaluation Items 2, 5, 7, 9, 11, 13, 15, and 16 Factor 2. Appearance Power/Control Items 8, 14, 18, 19, and 20 Factor 3. Appearance Standards and Behavior Items 1, 3, 4, 6, 10, 12, and 17 |
| Present study: Swedish women with breast cancer undergoing mastectomy and reconstruction | Factor 1. Body Image Investment Cognition – Breast Items 2, 5, 7, 9, 11, 13, 14, and 20 Factor 2. Body Image Investment Behaviors – Breast Items 1, 3, 4, 6, 10, 12, 17, and 18 Factor 3. Body Image Investment Emotions – Breast Items 8, 15, 16, and 19 |
Body-Esteem Scale for Adolescents and Adults (BESAA) is a 23-item scale consisting of three subscales: Body-Esteem (BE)-Appearance (10 items), BE-weight (eight items), and BE-Attribution (five items). The participants rated their answers on a five-point Likert scale. The ratings ranged between 0 and 4, and negative items were reverse scored. The composite scores and scores for each subscale were calculated. Higher scores indicate higher body-esteem dimensions [23]. The BESAA was translated and validated in a Swedish population [24].
Translation of ASI-R
The original English version of the ASI-R [19] was translated independently by two professional translators who spoke Swedish as their native language. The study team discussed the two versions and agreed upon the Swedish version. Subsequently, a professional translator who spoke English as a native language translated the chosen Swedish version back into English. The original author of the questionnaire provided feedback on the back-translated version (Figure 1).
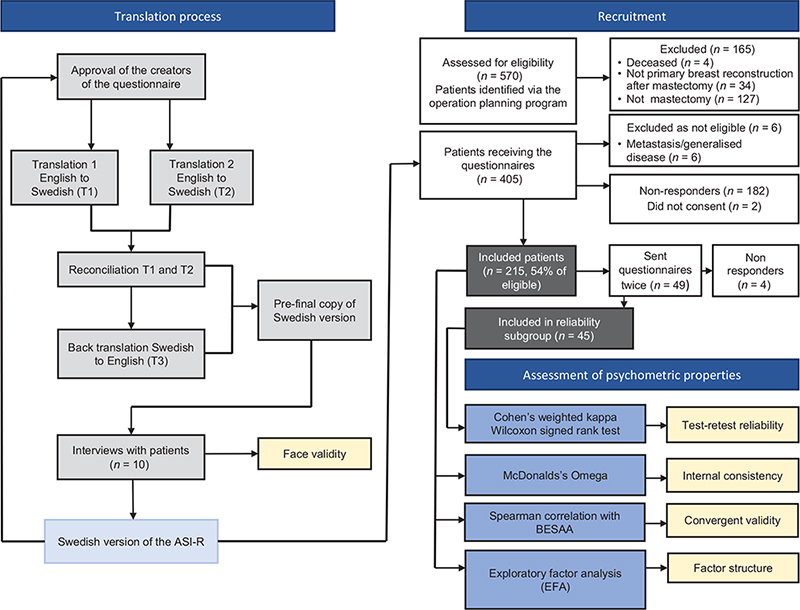
Figure 1. Course of the study.
Face validity
Five preoperative and five postoperative patients were interviewed using a semi-structured interview guide regarding how they experienced the questionnaire. The interviews were performed by a clinical psychologist (LW) with experience in working with the patient group.
Psychometric evaluation of the ASI-R: statistical analyses and hypotheses
Questionnaire scores were treated as ordinal data for all analyses except the EFA. All tests were two-tailed, and a p-value of 0.05 was used to indicate statistical significance. Data are presented as median, minimum, and maximum values and frequencies. Statistical analyses were performed using SPSS software (version 28.0.1.0). The results of these analyses are summarized in Figure 1. Missing data were replaced with the mean of the answered items for each subscale if half or more of the items were present. Scales were excluded if more than half of the items were missing.
Exploratory factor analysis
Before factor analysis was performed, data were examined for outliers, normality (skewness and kurtosis), factorability (the Kaiser–Meyer–Olkin [KMO] measure of sampling adequacy) [25] and the Bartlett’s test of sphericity [26] was used to determine the appropriateness of the factor analysis. Data are considered approximately normally distributed if the skewness and kurtosis (excess) values are between −1 and +1 [27]. In contrast, skewness ≥2.0 and kurtosis ≥7.0 are problematic when conducting factor analysis [28]. However, the Bartlett’s test should be significant, and KMO values should be ≥0.6 [29].
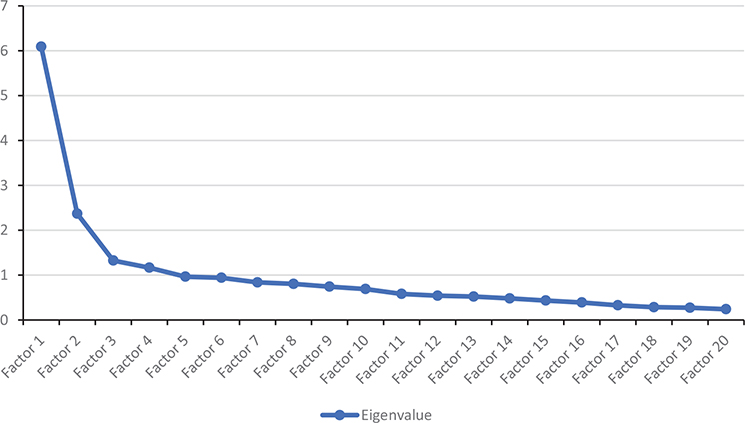
The EFA was conducted to assess the instrument’s underlying factor structure [30]. The EFA was performed using principal axis factoring, as it does not require normally distributed data [31]. To determine the number of factors to be retained, the Kaiser criterion (eigenvalues-greater-than-one-rule) [32] and an examination of the Cattell’s scree plot, ordering the eigenvalues in a downward curve [33] were used. The numbers above the point(s) where there is a break in the data indicate the number of factors to be retained. These criteria were combined with a prior theory [34]. Hence, a different number of factors was retained for further analyses.
The different factor solutions were then rotated to aid in interpretation. An oblique promax rotation was used, as it permits factors to correlate [30]. This rotation method produces a pattern and structure matrices, both of which were analyzed [30]. The EFA is highly explorative and aims to find a logical final structure that is conceptually and theoretically meaningful, and empirically supported [30]. A final factor structure should preferably have factors with loadings >0.30, with no or few cross-loadings, a minimum of 3–5 items [35], and an internal consistency of >0.7 [35]. Different factor solutions were compared to determine the best fit solution [34]. The conceptual significance of items with loadings <0.30 was examined, as items with small loadings and little conceptual contribution were removed [36]. Similarly, items with commonalities <0.2 were removed, as they indicate little shared variance [37].
Confirmatory factor analysis
If a sample of limited size is achieved, the EFA will be prioritized according to the guidelines for translated instruments [29].
Convergent validity
Convergent validity was tested against the BESAA. The ASI-R and BESAA measures were related but were not identical constructs; therefore, negative and moderate correlations, ranging between 0.30 and 0.50, were hypothesized [38]. However, it was hypothesized that the first and second factors in the original factor structure [19] correlated more strongly with the BESAA than the second factor from the original structure, as these factors involve more similar constructs, such as cognitive and affective aspects of appearance evaluation, to a greater extent. The Spearman’s correlation coefficient (ρ) was used to examine convergent validity.
Content validity
Content validity can be affected if an instrument lacks extreme items [39]. Therefore, the floor and ceiling effects were examined. Floor and ceiling effects were considered present if >15% of the participants reached the maximum or minimum score [40].
Internal consistency
McDonald’s Omega (ω) was used to examine internal consistency [41]. McDonald’s Omega can range from 0 to 1 [42], and a value between 0.7 and 0.95 indicates a good internal consistency [39].
Test-retest reliability
The weighted Cohen’s kappa coefficient was used to investigate test-retest reliability [39]. Kappa coefficients (κ) of >0.70 were considered good, and >0.80 were regarded as strong agreement [39, 43]. Test-retest reliability was further examined using the Wilcoxon signed-rank test for the subscales and composite ASI-R score, as failure to reject the null hypothesis indicated good reliability [29].
Results
Swedish translation of the ASI-R instrument
One of the Swedish versions, translated by two independent translators, was thought to better mirror the methods of expression in Swedish and was deemed the most appropriate of the two translated versions. For example, the rejected versions contained items that used complicated expressions and did not use everyday language. No changes were considered necessary in the selected version. The original author provided feedback on items 4 and 19 in the back-translated English version. One point of feedback was that the wording of item 4 indicated dislike rather than disinterest. However, the Swedish wording does not imply dislike, but has a connotation of being unbothered (‘har aldrig brytt mig’), and we decided not to make any changes to the Swedish version. The feedback received on item 19 was that the back-translated version referred to ‘keeping a check on’ instead of ‘controlling’, which the author did not find a suitable translation. However, the Swedish version uses the word ‘controlling’ (‘control’); therefore, we did not make any changes to item 19 either.
Face validity of the ASI-R instrument in patients with breast cancer
All five participants thought that the instructions were easy to understand. Most of the participants believed that all the items were relevant and easy to understand. Two participants thought it took a lot of work to answer some items about their appearance, as they did not usually reflect on their appearance in their ordinary lives or had ambivalent feelings towards it. None of the participants believed that items/questions were missing from the theme. Most of the participants thought that the answer options ranging between 1 and 5 were good. In summary, the Swedish ASI-R has a good face validity.
Participants
Three hundred and ninety-seven patients were eligible for the study, and 215 participants responded (54%). To examine test-retest reliability, 49 participants were sent the questionnaire twice, the second time 2 weeks after they had responded to the first questionnaire, and 45 responded (92%) (Figure 1). The median age of the participants was 53 years (range: 34–78 years). All the participants had undergone therapeutic mastectomies for breast cancer and were awaiting delayed breast reconstruction.
For the composite ASI-R score, two participants had missing data on several items and were, therefore, excluded from factor analysis but included in the analysis of psychometric properties. Data were imputed for six participants (3%). The composite scale and one subscale were excluded from analyzes of psychometric properties for one participant. Two participants were excluded from convergent validity analyses due to missing vales on BESAA.
Factor structure in patients with breast cancer undergoing reconstruction
No extreme outliers were found, and skewness and kurtosis values were within normal ranges for all the items except item 8, which had a value of −1.1 for skewness and 1.7 for kurtosis. The result of the KMO was 0.85, and the Bartlett’s test of sphericity was significant (p < 0.001). Hence, the data were considered factorable. The Kaiser criterion alone indicated that the four factors should be retained. Examination of the scree plot (Figure 2) showed that 2–4 factors should be retained. Hence, two, three, and four factors were further examined using oblique promax rotation.
Neither a two-factor nor a four-factor solution was considered most appropriate for the current sample. The two-factor solution was similar to the original factor solution, with only one item (item 8) loaded onto the MS instead of the SES. However, this only accounted for 36.3% cumulative variance. The loading of item eight did not make theoretical sense, as it is highly self-evaluative and almost identical to an item still loading on the SES (item 15). The two-factor solution had an internal consistency of >0.7 for both factors. The four-factor solution accounted for more variance (44.3%), but only had three items on factors three and four, and factor three had an internal consistency of <0.7.
In the present sample, a three-factor solution was considered the most adequate solution (Table 1), accounting for 40.4% cumulative variance. All the factors showed good internal consistency and moderate inter-factor correlations (Table 2). Items 16 and 18 had cross-loadings of >0.3, and item 6 had cross-loadings of <0.3 on the second and third factors (Table 2). Both items 16 (‘fantasizing about looking better’) and 18 (‘appearance being necessary for an individual’s identity’) had considerably stronger loadings on factors 3 and 2 (Table 2), and were therefore kept. Item 6 involved apparent appearance-fixing behavior (checking the appearance in the mirror) and was included in factor 2. Similarly, item 3 (‘trying to be as physically attractive as possible’) had low communality, but was retained as it had a moderate, salient loading and made a theoretical sense on factor 2 (Table 2). As expected, when the factors were correlated, the structure matrix differed from the pattern matrix, showing cross loadings for most items.
These three factors reflect the cognitive, behavioral, and affective dimensions of body image investment. An overview of the new subscales, previously described subscales, and their items is provided in Table 1. We conceptualized the first factor as the Body Image Investment Cognition – Breast subscale. This subscale consists of eight items derived from the original SES subscale [19], and is similar to the Appearance Self-Evaluation subscale in body investment [12]. The second factor was conceptualized as the Body Image Investment Behaviors – Breast subscale, which consists of eight items. It is identical to the original MS subscale [19] and similar to the Appearance Standards and Behavior subscale reported by Chua et al. [12]. The third factor was conceptualized as the Body Image Investment Emotions – Breast scale, which consists of four items derived from the original SES subscale [19] and resembles the Appearance Power/Control subscale in body image investment previously found among patients with breast cancer [12]. For the current factor solution, two items (items 8 and 9) matched the Appearance Power/Control subscale [12]. However, items 15 and 16 differed, as they loaded on the Body Image Investment Emotions – Breast subscale in the current study, but on the Appearance Self-Evaluation subscale in the American cohort [12].
The new three-subscale structure (Table 1) was used for the remainder of the validation: Body Image Investment Cognition – Breast, Body Image Investment Behaviors – Breast, and Body Image Investment Emotions – Breast.
Convergent validity
As hypothesized, the composite ASI-R score, Body Image Investment Cognition – Breast, and Body Image Investment Emotions – Breast scores had moderate negative correlations with the composite BESAA score (Table 3). There was no significant correlation between Body Image Investment Behaviors - Breast and BESAA. The moderate and negative correlations between the Body Image Investment subscales and BESAA indicated that the Swedish ASI-R has acceptable convergent validity.
Internal consistency
The results indicated acceptable internal consistency for the composite ASI-R and all the three factors (Table 3). Omega if the item deleted varied between 0.86 and 0.87 (composite ASI-R), 0.76–0.81 (Body Image Investment Cognition – Breast), 0.75–0.80 (Body Image Investment Behaviors–Breast), and 0.61–0.69 (Body Image Investment Emotions – Breast), and did not therefore result in the deletion of any items.
Test-retest reliability
There was strong agreement between the composite ASI-R and all the three factors. No statistically significant differences were observed between the scales (Table 3).
Floor and ceiling effects
No floor or ceiling effects were observed on the composite scale. For the Body Image Investment Cognition – Breast subscale, 0.5% of the participants received the maximum or minimum score. For the Body Image Investment Behaviors – Breast subscale, 0.9% of the participants obtained the maximum score. For the Body Image Investment Emotions – Breast subscale, 1.4% of the participants obtained a maximum or minimum score.
Discussion
The primary aim of this study was to translate and examine the psychometric properties of the ASI-R instrument in Swedish patients undergoing breast reconstruction. A three-factor solution was an adequate factor solution that showed good overall psychometric properties, similar to previous findings in American patients with breast cancer undergoing reconstruction [12]. As the included items were slightly different from those of the American population (Table 1), the subscales were assigned new names: Body Image Investment Cognition – Breast, Body Image Investment Behaviors – Breast, and Body Image Investment Emotions – Breast.
ASI-R subscales in patients with breast cancer undergoing breast reconstruction
The three factors obtained in this study reflect the main dimensions of body image: cognitive, behavioral, and affective [16]. Body Image Investment Cognition – Breast reflects body image investment manifested in dysfunctional patterns of cognition, distorted beliefs about the importance of appearance (e.g. that appearance is responsible for what happens in life), and covert behaviors (e.g. comparing one’s appearance to others and appearance rumination) triggered by interaction with the environment. Body Image Investment Behaviors – Breast reflects body image investment manifested in overt behaviors, such as monitoring appearance. Body Image Investment Emotions – Breast captures the emotional manifestation of body image investment, as it reflects the influence of appearance evaluation on emotional well-being. Further, it also reflects the belief that appearance can and should be controlled because of its impact on what happens in life and an individual’s well-being.
The obtained factor solution was similar to the three-factor solution found among American patients with breast cancer [12] and the original factor structure [19]. Body Image Investment Behaviors – Breast is a stable factor across different studies and populations; in the current study, American breast cancer cohort [12] and original factor structure [19]. However, MS has a slightly different meaning in women with breast cancer, and it has been hypothesized that it might function as a protective factor against body image problems [44]. The original SES subscale was divided into two-factor solutions in the American breast cancer [12] and the present Swedish breast cancer cohorts. Most items from the SES loaded on the Appearance Power/Control in the American breast cancer population [12] and on Body Image Investment Emotions – Breast in the present population. These two factors regarding the importance of control over appearance and its influence on emotions are similar. However, Body Image Investment Emotions – Breast has a narrower focus on the affective dimension and does not reflect appearance as an essential part of an individual’s identity. Similarly, Body Image Investment Cognition – Breast has a narrower focus on cognition than the original SES [19] and Appearance Self-Evaluation [12] because it consists of affective and self-evaluative items derived from the original SES. These studies were conducted in the United States [12, 19]. Therefore, cultural influences on body image attitudes [16] could explain some of the differences compared to an American cohort of patients with breast cancer regarding the distribution of items and amount of variance explained (95% vs. 40%) [12].
The importance of control as a central body investment theme in the breast cancer population was previously suggested in an American cohort [12]. That MS might be a protective factor for psychological adjustment [44], which is also evident in Body Image Investment Emotions – Breast in the present study. Breast reconstruction can be viewed as a means of controlling changes in appearance changes [12]. Nonetheless, breast reconstruction is an intervention that can help women restore a sense of normality or worsen their body image if expectations are not met [45]. Patients with breast cancer often experience a loss of control over their bodies that goes beyond appearance changes [46].
Methodological considerations
The study has several strengths and limitations that need to be highlighted. The main strengths are that the translation and validation were performed following guidelines in a population of participants missing a breast and all suffering from their flat chest in one way or another, as they have opted for breast reconstruction, which they had not received; this was an appropriate group to use for the validation of body-image instruments for use in breast cancer populations. Another strength is that this study represents the first validation of an instrument outside the USA. As body image is affected by cultural factors, the validation of instruments is necessary in different countries and other languages.
This study’s limitations are principally related to the relatively small sample size, which limits the robustness of the statistical tests. Concerning the factor analysis, a small sample size increases the risk of unstable factor solutions [36]. The limited sample size also necessitated a prioritization between EFA and confirmatory factor analysis (CFA), as the sample was not large enough to be split in half, and the performance of both EFA and CFA in the same sample might have yielded biased results. The EFA was prioritized according to the guidelines for translated instruments [29]. Recommendations regarding sample size when conducting an EFA vary according to the estimation methods [36] and depend on the data [31]. It has been argued that a sample size of 150 is sufficient for initial factor analysis [36]. The small sample size in this study may also explain the relatively low variance (40%), which could be accounted for by the factor solution in this study. Ideally, at least 50% of the variance should preferably be explained by an instrument [36]. A lower explained variance could indicate that the factors are not sufficiently meaningful, or that the instrument does not produce data with a good internal structure that can reflect latent constructs [47]. However, this is unlikely because a higher variance was previously observed for the instrument in another breast cancer population [12].
Another limitation of the study is that only one body image instrument was used to investigate convergent validity [29]. In line with other studies [19], the correlation between the original MS scale, herein referred to as the Body Image Investment Behaviors – Breast, was particularly low.
Clinical implications for the measurement of body image in patients with breast cancer
Validation of the ASI-R in patients with breast cancer allowed for a valid measurement of body investment in the group. Body Image Investment Cognition – Breast and Body Image Investment Emotions – Breast seem to reflect dysfunctional cognitive and emotional patterns (e.g. dysfunctional investment). This could allow the identification of patients with negative body image who require additional interventions, such as cognitive behavioral therapy-based interventions [1], in addition to breast reconstruction, to achieve a healthy body image after breast cancer. Additionally, the instrument enables the measurement of positive body image, as Body Image Investment Behaviors – Breast (originally MS) seems to reflect positive ways of investing in body image among patients with breast cancer [48]. Knowledge of positive body image in patients with breast cancer and its consequences have previously been identified as a field where more studies are needed [11].
Conclusions
In conclusion, the ASI-R instrument has overall good psychometric properties for Swedish women undergoing mastectomy and breast reconstruction, enabling the measurement of body investment for both clinical and research purposes. The factor structure obtained was considered similar to the original factor structure [19] and three-factor solution obtained from an American cohort of patients with breast cancer [12]. Three new subscales have been suggested: Body Image Investment Cognition – Breast, Body Image Investment Behaviors – Breast, and Body Image Investment Emotions – Breast. Control appears to be a central theme in patients with breast cancer undergoing mastectomy and breast reconstruction. Further studies on convergent validity and CFA are required.
Acknowledgments
First, we thank all the participants who contributed to the study. We would also like to thank Akademistatistik, University of Gothenburg, for statistical advice and specialist nurses Ms Clary Andrade and Ms Susanne Meyer, Department of Plastic Surgery, Sahlgrenska University Hospital, for skillful data collection and management.
CRediT roles
Linn Weick: conceptualization, methodology, validation, formal analysis, investigation, data curation, writing–original draft, writing–review, and editing. Carolina Lunde: conceptualization, methodology, validation, formal analysis, investigation, data curation, writing–original draft, writing–review and editing, and supervision. Emma Hansson: conceptualization, methodology, validation, formal analysis, investigation, resources, data curation, writing–original draft, writing–review and editing, supervision, project administration, and funding acquisition.
Data statement
Data can be made available upon reasonable request and necessary permits.
ORCID
Emma Hansson  https://orcid.org/0000-0002-3218-0881
https://orcid.org/0000-0002-3218-0881
Carolina Lunde https://orcid.org/0000-0002-9503-2253
References
[1] Fingeret MC, Teo I, Epner DE. Managing body image difficulties of adult cancer patients: lessons from available research. Cancer: New York. 2014;120:633–641. https://doi.org/10.1002/cncr.28469
[2] Begovic-Juhant A, Chmielewski A, Iwuagwu S, et al. Impact of body image on depression and quality of life among women with breast cancer. J Psychosoc Oncol. 2012;30:446–460. https://doi.org/10.1080/07347332.2012.684856.
[3] Hopwood P, Hopwood N. New challenges in psycho-oncology: an embodied approach to body image. Psychooncology. 2019;28:211–218. https://doi.org/10.1002/pon.4936
[4] Clarke A, Paraskeva N, White P, et al. PEGASUS: the design of an intervention to facilitate shared decision-making in breast reconstruction. J Cancer Educ. 2021;36:508–518. https://doi.org/10.1007/s13187-019-01656-6
[5] Lee C, Sunu C, Pignone M. Patient-reported outcomes of breast reconstruction after mastectomy: a systematic review. J Am Coll Surg. 2009;209:123–133. https://doi.org/10.1016/j.jamcollsurg.2009.02.061
[6] Dempsey K, Mathieu E, Brennan M, et al. The role of breast reconstruction choice on body image patient-reported outcomes at four years post-mastectomy for breast cancer: a longitudinal prospective cohort study. Psychooncology. 2022;31:54–61. https://doi.org/10.1002/pon.5776
[7] Fingeret MC, Nipomnick SW, Crosby MA, et al. Developing a theoretical framework to illustrate associations among patient satisfaction, body image and quality of life for women undergoing breast reconstruction. Cancer Treat Rev. 2013;39:673–681. https://doi.org/10.1016/j.ctrv.2012.12.010
[8] Potter S, Holcombe C, Ward JA, et al. Development of a core outcome set for research and audit studies in reconstructive breast surgery. Bri J Surg. 2015;102:1360–1371. https://doi.org/10.1002/bjs.9883
[9] Harcourt D, Rumsey N. Psychological aspects of breast reconstruction: a review of the literature. J Adv Nurs. 2001;35:477–487. https://doi.org/10.1046/j.1365-2648.2001.01865.x
[10] Paterson CL, Lengacher CA, Donovan KA, et al. Body image in younger breast cancer survivors: a systematic review. Cancer Nurs. 2016;39:E39–E58. https://doi.org/10.1097/NCC.0000000000000251
[11] Brunet J, Price J. A scoping review of measures used to assess body image in women with breast cancer. Psychooncology. 2021;30:669–680. https://doi.org/10.1002/pon.5619
[12] Chua AS, DeSantis SM, Teo I, et al. Body image investment in breast cancer patients undergoing reconstruction: taking a closer look at the Appearance Schemas Inventory-Revised. Body Image. 2015;13:33–37. https://doi.org/10.1016/j.bodyim.2014.12.003
[13] Teo I, Reece GP, Huang SC, et al. Body image dissatisfaction in patients undergoing breast reconstruction: examining the roles of breast symmetry and appearance investment. Psychooncology. 2018;27:857–863. https://doi.org/10.1002/pon.4586
[14] Jarry JL, Dignard NAL, O’Driscoll LM. Appearance investment: the construct that changed the field of body image. Body Image. 2019;31:221–244. https://doi.org/10.1016/j.bodyim.2019.09.001
[15] White CA. Body image dimensions and cancer: a heuristic cognitive behavioural model. Psychooncology. 2000;9:183–192. https://doi.org/10.1002/1099-1611(200005/06)9:3%3C183::AID-PON446%3E3.0.CO;2-L
[16] Cash TF, Smolak L. Body image: a handbook of science, practice, and prevention. Guilford Press; 2011.
[17] Cash TF, Szymanski ML. The development and validation of the body-image ideals questionnaire. J Pers Assess. 1995;64:466–477. https://doi.org/10.1207/s15327752jpa6403_6
[18] Sherman KA, Woon S, French J, et al. Body image and psychological distress in nipple-sparing mastectomy: the roles of self-compassion and appearance investment. Psychooncology. 2017;26:337–345. https://doi.org/10.1002/pon.4138
[19] Cash TF, Melnyk SE, Hrabosky JI. The assessment of body image investment: an extensive revision of the Appearance Schemas Inventory. Int J Eat Disord. 2004;35:305–316. https://doi.org/10.1002/eat.10264
[20] Bröstcancer, Nationellt Vårdprogram. 2023 [Version 4.3]. Available from: https://kunskapsbanken.cancercentrum.se/globalassets/cancerdiagnoser/brost/vardprogram/nationellt-vardprogram-brostcancer.pdf [cited 2024-06-04]
[21] Cash TF, Labarge AS. Development of the Appearance Schemas Inventory: a new cognitive body-image assessment. Cogn Ther Res. 1996;20:37–50. https://doi.org/10.1007/BF02229242
[22] Cash TF. Manual for the Appearance Schemas Inventory-Revised. 2009. Available from the author’s website www.body-image.com
[23] Mendelson BK, Mendelson MJ, White DR. Body-esteem scale for adolescents and adults. J Pers Assess. 2001;76:90–106. https://doi.org/10.1207/S15327752JPA7601_6
[24] Erling A, Hwang CP. Body-esteem in Swedish 10-year-old children. Percept Mot Skills. 2004;99:437–444. https://doi.org/10.2466/pms.99.2.437-444
[25] Kaiser HF. An index of factorial simplicity. Psychometrika. 1974;39:31–36. https://doi.org/10.1007/BF02291575
[26] Bartlett M. A further note on the multiplying factors for various X2 approximations in factor analysis. J R Stat. 1954;16:296–298. https://doi.org/10.1111/j.2517-6161.1954.tb00174.x
[27] Mishra P, Pandey CM, Singh U, et al. Descriptive statistics and normality tests for statistical data. Ann Card Anaesth. 2019;22:67–72. https://doi.org/10.4103/aca.ACA_157_18
[28] Curran PJ, West SG, Finch JF. The robustness of test statistics to nonnormality and specification error in confirmatory factor analysis. Psychol Methods. 1996;1:16–29. https://doi.org/10.1037/1082-989X.1.1.16
[29] Swami V, Barron D. Translation and validation of body image instruments: challenges, good practice guidelines, and reporting recommendations for test adaptation. Body Image. 2019;31:204–220. https://doi.org/10.1016/j.bodyim.2018.08.014
[30] Osborne J. Best practices in exploratory factor analysis. 2014. CreateSpace Independent Publishing Platform
[31] Fabrigar LR, Wegener DT, MacCallum RC, et al. Evaluating the use of exploratory factor analysis in psychological research. Psychol Methods. 1999;4:272–299. https://doi.org/10.1037/1082-989X.4.3.272
[32] Kaiser HF. The application of electronic computers to factor analysis. Educ Psychol Measur. 1960;20:141–151. https://doi.org/10.1177/001316446002000116
[33] Cattell RB. The scree test for the number of factors. Multivariate Behav Res. 1966;1:245–276. https://doi.org/10.1207/s15327906mbr0102_10
[34] Costello AB, Osborne J. Best practices in exploratory factor analysis: four recommendations for getting the most from your analysis. Pract Assess Res Eval. 2005;10:7.
[35] Watkins MW. Exploratory factor analysis: a guide to best practice. J Black Psychol. 2018;44:219–246. https://doi.org/10.1177/0095798418771807
[36] Beavers AS, Lounsbury JW, Richards JK, et al. Practical considerations for using exploratory factor analysis in educational research. Pract Assess Res Eval. 2013;18:6.
[37] Child D. The essentials of factor analysis. London & New York :A&C Black; 2006.
[38] Prinsen CAC, Mokkink LB, Bouter LM, et al. COSMIN guideline for systematic reviews of patient-reported outcome measures. Qual Life Res. 2018;27:1147–1157. https://doi.org/10.1007/s11136-018-1798-3.
[39] Terwee CB, Bot SD, de Boer MR, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007;60:34–42. https://doi.org/10.1016/j.jclinepi.2006.03.012
[40] McHorney CA, Tarlov AR. Individual-patient monitoring in clinical practice: are available health status surveys adequate? Qual Life Res. 1995;4:293–307. https://doi.org/10.1007/BF01593882
[41] Dunn TJ, Baguley T, Brunsden V. From alpha to omega: a practical solution to the pervasive problem of internal consistency estimation. Br J Psychol. 2014;105:399–412. https://doi.org/10.1111/bjop.12046
[42] Stensen K, Lydersen S. Internal consistency: from alpha to omega? Tidsskr Nor Lægeforen. 2022;142:0112. https://doi.org/10.4045/tidsskr.22.0112
[43] McHugh ML. Interrater reliability: the kappa statistic. Biochem Med. 2012;22:276–282. https://doi.org/10.11613/BM.2012.031
[44] Moreira H, Silva S, Canavarro MC. The role of appearance investment in the adjustment of women with breast cancer. Psychooncology. 2010;19:959–966. https://doi.org/10.1002/pon.1647
[45] Brunet J, Price J, Harris C. Body image in women diagnosed with breast cancer: a grounded theory study. Body Image. 2022;41:417–431. https://doi.org/10.1016/j.bodyim.2022.04.012
[46] Hefferon K, Grealy M, Mutrie N. Transforming from cocoon to butterfly: the potential role of the body in the process of posttraumatic growth. J Hum Psychol. 2009;50:224–247. https://doi.org/10.1177/0022167809341996
[47] Henson RK, Roberts JK. Use of exploratory factor analysis in published research: common errors and some comment on improved practice. Educ Psychol Measur. 2006;66:393–416. https://doi.org/10.1177/0013164405282485
[48] Moreira H, Canavarro MC. A longitudinal study about the body image and psychosocial adjustment of breast cancer patients during the course of the disease. Eur J Oncol Nurs. 2010;14:263–270. https://doi.org/10.1016/j.ejon.2010.04.001