ORIGINAL RESEARCH ARTICLE
Clinical presentation of hemifacial microsomia in a South African population
Peterson M. Atibaa,c, Anil Madareeb and Lelika Lazarus PhDa
aDiscipline of Clinical Anatomy, School of Laboratory Medicine and Medical Sciences, Westville Campus University of KwaZulu-Natal, Durban, South Africa; bDepartment of Plastic and Reconstructive Surgery, School of Clinical Medicine, University of KwaZulu-Natal, Durban, South Africa; cAnatomy Programme, Faculty of Basic Medical and Health Sciences, College of Health Sciences, Bowen University, Iwo, Osun State, Nigeria
ABSTRACT
Background: Hemifacial microsomia (HFM) presentation includes gross distorted ramus, malposition temporomandibular joint, small glenoid fossa, distorted condyle and notch, malformed orbit, cupping ear or absent external ear, and facial nerve palsy. HFM is the second most prevalent congenital deformity of the face, with little literature from the South African population. This retrospective study elucidated the demographic characteristics and clinical presentations of HFM patients in a select South African population and compared it to the literature.
Methods: A retrospective study of HFM patients diagnosed through clinical presentation and confirmed by plain radiograph or computed tomography was conducted. The patient’s charts were reviewed for age, sex, laterality, side, the severity of the deformity, and associated craniofacial and extra-craniofacial anomalies. The clinical presentation of malformations was categorised according to the OMENS classification, using five major craniofacial manifestations of HFM.
Results: Twenty-five patients were included, with a male-to-female ratio of 1:1.78. The population distribution is 60% Black, 32% Indian, 4% White and 4% Coloured. A right-to-left laterality ratio of 1.4:1 and 4% bilateral affectation. This study showed 100% mandibular hypoplasia, 84% ear deformity, 40% orbital deformity, 60% facial nerve defect and 100% soft tissue defect affectation with noticeable facial asymmetry. Other craniofacial anomalies were recorded in 84%, while extracraniofacial anomalies were recorded in 40% of this HFM population.
Conclusion: There is a high degree of variability in the deformities in HFM in the South African population, distinguishing it from the international population. A multidisciplinary approach is required for its treatment and management.
KEYWORDS: Hemifacial microsomia; OMENS+ classification; clinical presentation; South Africa
Citation: Journal of Plastic Surgery and Hand Surgery 2025; 60: 1–6. DOI: https://doi.org/10.2340/jphs.v60.42402.
Copyright: © 2025 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 27 July 2024; Accepted: 30 October 2024; Published: 21 January 2025
CONTACT Lelika Lazarus ramsaroopl@ukzn.ac.za Discipline of Clinical Anatomy, School of Laboratory Medicine and Medical Sciences, Westville Campus University of KwaZulu-Natal, Durban, South Africa.
Competing interests and funding: The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no specific funding for this study.
Introduction
Symptoms of the first and second pharyngeal arch syndrome include otomandibular dysplasias (Hemifacial microsomia [HFM]), mandibulofacial dysostosis, oculoauriculovertebral dysplasias, branchio-oto-renal syndrome, Pierre Robin sequence and Nager acrofacial dysostosis. HFM is the second most prevalent congenital deformity of the face, with an incidence of 1:3,500–5,600 [1–3]. HFM is due to genetic, maternal, and environmental conditions leading to haemorrhage of the stapedial artery, dysgenesis of Meckel’s cartilage and aberrant migration of neural crest cells [2]. The clinical features of HFM include a unilaterally deformed mandible with malformed ear structures comprising of the gross distorted ramus, malpositioned temporomandibular joint (TMJ), small glenoid fossa, distorted condyle and notch, malformed orbit, cupping ear, absent external ear and facial nerve palsy [4]. HFM affects skeletal and overlying soft tissues [5, 6]. The first widely used classification of HFM was by Pruzansky [7] using mandibular hypoplasia; this was further improved upon by Kaban et al. [8], who included the TMJ. Another HFM classification is the skeletal–auricular–soft tissue (SAT) deficiency [9]. Vento et al. [10] introduced the OMENS classification pattern by classifying HFM-associated anomalies, including orbital distortion (O), mandibular hypoplasia (M); ear anomaly (E); nerve involvement (N); and soft tissue deficiency (S). Horgan et al. [11] expanded these anomalies to include extracraniofacial defects, thus making the revised classification system OMENS-Plus (+). In addition, there is an association between HFM and macrostomia, Tessier’s cleft number 7: Treacher-Collins syndrome [12, 13]. Several genes are implicated in the HFM population, such as OTX2, PLCD3, MYT1 and Pde4dip [2, 14]. Although there are large bodies of literature on HFM, most reports are from the international population, with a few reports from the African continent [3, 5, 15–17]. South Africa has a multiracial population, which includes Blacks, Whites, Coloured and Indians [18, 19]. The population distribution of KwaZulu-Natal is 86.8% Blacks, 7.4% Indians (Asian), 4.2% White and 1.4% Coloured. The percentage distribution of males to females is 47.5 and 52.5%, respectively [20]. There is a lack of literature on the clinical presentation of HFM in a South African population [15, 16]. This retrospective study was designed to understand the demographic characteristics and clinical presentations of HFM patients in a South African population and compare it to the literature.
Materials and methods
A retrospective study identified patients with HFM treated at the Department of Plastic and Reconstructive Surgery, Inkosi Albert Luthuli Central Hospital, from June 2003 to December 2022. Patients were diagnosed by a craniomaxillofacial surgeon through clinical presentation and confirmed by plain radiograph or computed tomography (CT) images and assessed using OMENS classification [10] (Table 1). A differential diagnosis was made to rule out other phenotypic similar syndromes of first and second pharyngeal arches, such as Treacher-Collins, branchio-oto-renal, Miller-Dierker CHARGE, and Parry Romberg. The first author retrieved 35 patients’ medical records from the hospital’s electronic archive, but 10 were excluded due to the incomplete records. Charts, photographs, and radiographs were reviewed to document demographic data and clinical findings in patients presented with HFM. The patient’s charts were reviewed for age, sex, laterality, side involved, deformity severity, and associated craniofacial and extra-craniofacial anomalies using OMENS+ classification [11]. The photographic evaluation included analysis of standardised patient photographs and reviewing any previous photographs during facial growth phases (if available). Imaging studies, including cephalometric films, panoramic films, and CT, were reviewed and analysed to document skeletal elements of the deformity and underdevelopment of soft tissues. The imaging studies for suspected extracraniofacial anomalies, including echocardiography, abdominal ultrasonography, brain magnetic resonance imaging (MRI), and CT spine, were reviewed. Written informed consent or consent permission was obtained for each patient involved in this study. In addition, informed consent was secured from all subjects or their legal guardians to publish images in an online open-access publication. All HFM patients were seen and followed by a multidisciplinary craniofacial team (such as an otolaryngologist, orthodontist, geneticist, audiologist, speech therapist, ophthalmologist, neurologist, clinical psychologist, social worker, paediatrician, maxillofacial and plastics surgeon).
Statistical analysis
The categorical variables were described as counts and percentage frequencies. A Chi-Square test was used to determine the association between categorical variables, and when the distribution of the cross-tabulations contains an expected value of less than five, a Fisher’s exact test was applied. The level of significance was kept at p < 0.05. All statistical analyses were completed using SPSS 28.0 (IBM Corp., Armonk, NY, USA).
Ethics
This study was conducted with the approval of the Biomedical Research Ethics Committee of the University of KwaZulu-Natal (Ref No: BREC/00004225/2022) and the Department of Health in the Province of KwaZulu-Natal (NHRD Ref.: KZ_202206_031). All methods were carried out following the University of KwaZulu-Natal standard-approved guidelines and regulations and all experimental protocols per the declaration of Helsinki.
Results
Patient characteristics
This study included 25 patients with HFM: 9 males (36%) and 16 females (64%). The following details were based on the medical records, information patients or their families provided and follow-up care. The population distribution among the patients includes 15 (60%) of Black descent, 8 (32%) of Indian descent, 1 (4%) of White descent and 1 (4%) of Coloured descent. Age at first assessment ranged from 9 days to 36 years (mean 5.4 years). Based on their records and follow-up care by the surgeon, eight patients (32%) were considered to have reached full facial growths, while 17 patients (68%) were still growing. The right side was affected in 14 patients (56%), while the left side was affected in 10 patients (40%), and 1 patient (4%) had a bilateral presentation of HFM. There were no significant differences between the sexes (p = 0.27) ratio and right-to-left-sidedness (p = 0.29).
OMENS classification
The clinical presentation was categorised according to the OMENS classification, and the five major craniofacial manifestations of HFM (orbit, mandible, ear, nerve, and soft tissue) were assessed (Figure 1–3). Each anatomic abnormality was graded from 0 to 3 according to the dysmorphic severity by OMENS classification (Table 1). For bilateral cases, each side is considered a separate subject. The 25 patients were considered 26 subjects, and the OMENS score was as follows in Table 2. There was no significant difference when comparing each substrate of the OMENS classification to the affected side: orbit (p = 0.47), mandible (p = 0.27), ear (p = 0.82), nerve (p = 0.44) and soft tissue (p = 0.49). There was no significant difference when comparing each substrate of the OMENS classification to sexes: orbit (p = 0.47), mandible (p = 0.29), ear (p = 0.09), nerve (p = 0.19) and soft tissue (p = 0.06).
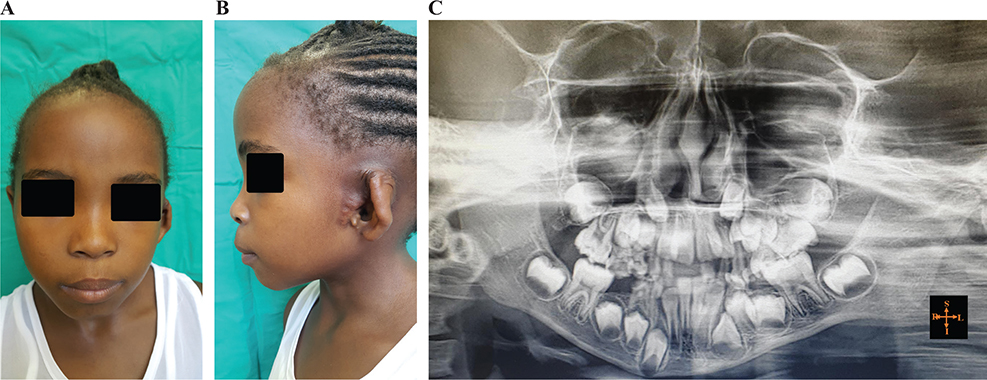
Figure 1. Characteristic features of HFM presentation in a 6-year-old patient based on OMENS classification. (A) A frontal view of a left-sided hemifacial microsomia (HFM) with mild soft tissue defects and a deformed ear. (B) The lateral view shows a mild hypoplasia of the external ear (E1) with most structures intact and mild soft tissue defects (S1). (C) A panoramic radiograph showing a deformed mandible (M2A), crowded teeth. The OMENS classification is O0M2AE1N1S1.

Figure 2. Characteristic features of hemifacial microsomia (HFM) presentation in a 15-year-old patient based on OMENS classification. (A) A frontal view of the face shows a right-sided HFM with marked facial nerve palsy, ear, and lower jaw deformities. (B) Lateral view showing remnant ear lobule and retrognathia. (C) A 3D reconstructed CT showing deformed mandible (M2B) and malocclusion class III with marked facial asymmetry. The OMENS classification is O1M2BE3N3S1.
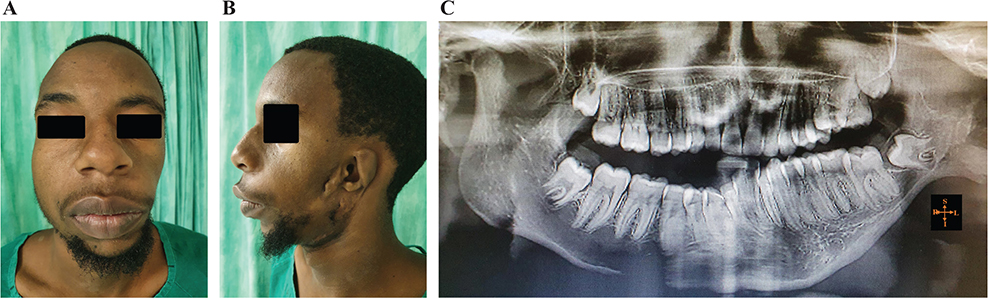
Figure 3. Characteristic features of hemifacial microsomia (HFM) presentation in a 21-year-old patient based on OMENS classification. (A) A frontal view showing a left-sided HFM with prelingual hearing loss, chin deviation, severe soft tissue deformity and facial asymmetry. (B) Lateral view showing ear (E1), retrognathia, and severe soft tissue deformities (S3). (C) A panoramic radiograph showing a deformed mandible (M3), malocclusion class III and chin deviation. The OMENS classification is O1M3E1N2S3.
Other craniofacial anomalies
Other accompanied craniofacial anomalies are malocclusion, ocular defects (such as blindness, nystagmus, telecanthus, hypertelorism, glaucoma, coloboma, cataract, blindness, anophthalmia and lagophthalmos), macrostomia, cranial nerve XI palsy, cleft lip and palate, isolated craniofacial palate, major craniofacial cleft, Treacher Collins syndrome, palatoglossal band, retrognathia, prelingual hearing loss, brachycephaly, craniosynostosis and hypoplastic muscle of mastication. The summary of the frequency of distribution is shown in Table 3.
Extracraniofacial anomalies
Extracraniofacial anomalies were recorded in this study’s 10 (40%) patients. Respiratory anomalies were reported in 9 (36%) patients; these include tracheomalacia, congenital pneumonia accompanied by asthma, sleep dyspnoea, and a blocked nose. Limb anomalies were reported in 4 (16%) patients; these include duplicate thumb, clinodactyly, club foot and achondroplasia. Three (12%) patients reported central nervous system anomalies, including periventricular leukomalacia, neurofibromatosis, hemiparesis, and mental deficit. Anomalies of the neck were reported in 3 (12%) patients, including torticollis and web neck. Vertebral anomalies were reported in 2 (8%) patients, including scoliosis, spinal fusion, hemivertebra, thoracic hyperkyphosis, Spinal bifida of T2–T8 and extranumeral rib. Congenital heart anomalies were reported in 2 (8%) patients, including dextrocardia, murmur and Tetralogy of Fallot with transposition of the great vessel. Genital abnormalities were reported in one patient (4%), including chordee and hypospadias. Renal agenesis was reported in one (4%) patient. Congenital recto-vaginal fistula was reported in one (3.85%) patient. The summary of the frequency of distribution is shown in Table 4.
Discussion
This study was designed to understand the demographic characteristics and clinical presentation of HFM patients in a South African population. The presentation of HFM differs from one individual to another, with or without extracraniofacial deformity [21]. Mandibular hypoplasia with or without ear deformity is the cornerstone for the phenotypic classification of HFM, distinguishing it from other craniofacial anomalies of first and second branchial arches [22]. This study showed 100% mandibular hypoplasia, 84% ear deformity, 40% orbital deformity, 60% facial nerve defect, 100% soft tissue defects, and 100% facial asymmetry. A total of 25 patients were included, with a male-to-female ratio of 1:1.78. The distribution within the included patients is 60% Black, 32% Indian, 4% White, and 4% Coloured. There is a right-to-left laterality ratio of 1.4:1 and 4% bilateral affectation. Other craniofacial anomalies were recorded in 84%, while extracraniofacial anomalies were recorded in 40% of this HFM population, which were not captured by the OMENS classification [10, 11]. The patients received no prior surgical intervention before presentation to our facility.
This study shows no significant difference between the male-to-female ratio and right-to-left-sidedness. Opinions differ about gender and laterality differences in the incidence of HFM. While some authors have reported that HFM is more present in males to females with a ratio of 3:2, respectively, and right-side laterality preponderance [23], others found no correlation between gender or laterality [11,24]. A population-based HFM study in Canada and the United States reported a demographic distribution of 63% White, 26% Hispanic, 5% Black, 4% Asian, and 3% Native American [17]. The differences reported in our study and the above studies could be due to the disparity in the sample size and socio-cultural factors. In addition, international data often lacks detailed racial stratification, emphasising the need for localised studies to understand the epidemiology of HFM better.
Deformities in the orbit size or position were recorded in 40% of patients in this study. This value falls within the range of previous studies (4–43%) in HFM [25, 26]. Ocular anomalies often accompany HFM. The presence of coloboma and epibulbar dermoid, along with features of HFM, is diagnosed as Goldenhar syndrome [27]. Ocular anomalies were present in 6.7–100% of patients [26]. This study had a 20% incidence of ocular defects. Surgical treatment to restore visual acuity is recommended before 5 years of age [25]. Mandibular hypoplasia is present in 73 to 91% of HFM patients [26, 28]. This study recorded higher mandibular hypoplasia in 100% of cases of HFM patients [3]. The hypoplastic mandible is associated with malocclusion, made noticeable by occlusal canting and retrognathia linked to obstructive sleep apnoea, cleft lip and palate, dental hypoplasia, feeding difficulty, speech and language difficulties, and macrostomia. Deformity of the mandible makes facial asymmetry noticeable in the HFM population [29]. Based on Kaban and colleagues’ severity grading and functional requirements [8], the treatment modalities used in the mild hypoplastic mandible (Type 1 and 2A) are osteotomy, distraction osteogenesis and genioplasty for lengthening the shortened mandible. In contrast, severe hypoplastic mandible (Type 2B and 3) involved orthognathic intervention and reconstruction of the mandible using alloplastic materials, costochondral or bone graft [5, 26, 30–33]. There is a lack of consensus on the timing of the treatment modalities. Some advocated an early age, while others elected for a late stage of development. Early treatment may improve facial symmetry and psychosocial acceptance but requires multiple revisional surgeries [5, 26]. In this series of patients, we employed early-age intervention for severe mandibular hypoplasia, while late-age intervention was used for mild cases. The degree of severity and functional requirements determine the mode of surgical intervention in HFM patients [4]. Several reports have suggested an increasing association between the severity of the ear and mandibular deformities. The deformity can affect external, middle, or internal ear structures. This study has a high prevalence of auricular deformity, with mild (46.15%), moderate (7.69%), and severe (30.77%) cases. Other accompanying anomalies, including preauricular tags, hypoplastic mastoid, low-set ears, low hairline, and hearing loss, were noticed. Detection of hearing problems in patients with HFM is vital to mitigate learning difficulties, speech development delay, and impaired social functioning [34]. The derivatives of the second pharyngeal arches (such as stapes, stylohyoid ligament, the lesser horn of hyoid, stapedius, platysma, and muscles of facial expression) are affected by the defect to the facial nerves. Facial nerve palsy affected about 60% of the HFM patients in this study [35]. The incidence of facial palsy in other studies is 22% [36] and 23.9% [37]. Multifactorial factors may cause this disparity compared to our study [2, 14]. Soft tissue defects accentuate facial asymmetry in HFM patients. The modalities include alloplastic implants, microvascular free tissue transfer, the pedicled flap, fat grafting, and functional reconstruction with cross-facial nerve grafting [36]. Mild-to-moderate soft tissue defects require fat grafting. The positive outcomes of fat grafting, the lowest complication rates, and a minor treatment burden make fat grafting a reasonable option for most HFM patients in whom soft-tissue correction is administered. Soft-tissue reconstruction may influence other types of treatment, such as mandible or ear reconstruction, and should, therefore, be coordinated within a multidisciplinary treatment plan [26, 36, 38]. The prevalence of extracraniofacial anomalies in international studies focusing on HFM patients was reported at 35.9% [3], 44% [39], 47% [40], 55% [11], 69% [41], and 85% [34]. In this study, we registered 40% of extracraniofacial anomalies in HFM patients. Noticeably, respiratory deformities account for the highest occurrence (36%). Renkema and co-authors reported only 3% of respiratory deformities (n = 991) [40] in their large population multinational study. We hypothesised that this disparity may be due to genetic or environmental factors. Extracraniofacial anomalies in this study were associated with severe mandibular, facial nerve, and soft tissue deformities. Renkema et al. [40] reported a similar association. The HFM population should be screened by physical examination and diagnostic tools such as electrocardiography, echocardiography, spine radiography, and renal ultrasound for extracraniofacial deformities. Some genes have been linked to the incidence of HFM; this includes mutation of OTX2, which may result in anophthalmia, microphthalmia and brain malformation [2, 14]; PLCD3 may result in aberrant migration of cranial neural crest cells in the development of head and neck [2, 14]; Itgb4 and Pde4dip may result in the inhibition osteogenesis of the mandible and other facial bones [14]. The genetic basis of HFM varies from one individual to another and not all cases of HFM have genetic causes. HFM is multifactorial in origin. Currently, research is still ongoing regarding the suggested genetic basis of HFM in South Africa and other parts of the World [14].
To the best of our knowledge, this is the first study in the South African population documenting demographic and clinical presentation in HFM with a higher prevalence in females. In this study, the right side is more affected with a higher incidence of facial nerve palsy. A deformed mandible accentuates facial asymmetry in the HFM population. There is a high degree of variability in the deformities of the mandible, ear, facial nerve, orbit, and soft tissue presentation in HFM in the South African population. Due to multiple deformities associated with HFM, a multidisciplinary (such as an otolaryngologist, orthodontist, geneticist, audiologist, speech therapist, ophthalmologist, neurologist, neurosurgeon, craniofacial surgeon, orthopaedic surgeon, hand surgeon, spinal surgeon, cardiologist, cardiac surgeon, urologist, nephrologist, colorectal surgeon, gynaecologic surgeon, maxillofacial and plastics surgeon) approach is required for its treatment and management.
Acknowledgements
The authors would like to acknowledge Dr O.S. Aladeyelu and Dr B. Omotoso expertise in the manuscript’s proofreading and contribution.
References
[1] Atiba PM, Omotoso BR, Madaree A, et al. Hemifacial microsomia: a scoping review on progressive facial asymmetry due to mandibular deformity. Oral Maxillofac Surg. 2024; 28(4): 1441–1455. https://doi.org/10.1007/s10006-024-01276-5
[2] Chen Q, Zhao Y, Shen G, et al. Etiology and pathogenesis of hemifacial microsomia. J Dent Res. 2018; 97(12): 1297–1305. https://doi.org/10.1177/0022034518795609
[3] Allam KA. Hemifacial microsomia: clinical features and associated anomalies. J Craniofac Surg. 2021; 32(4): 1483–1486. https://doi.org/10.1097/SCS.0000000000007408
[4] Paul MA, Opyrchal J, Knakiewicz M, et al. Hemifacial microsomia review: recent advancements in understanding the disease. J Craniofac Surg. 2020; 31(8): 2123–2127. https://doi.org/10.1097/scs.0000000000006616
[5] Taiwo A. Classification and management of hemifacial microsomia: a literature review. Ann Ibadan Postgrad Med. 2020; 18(1): S9–S15.
[6] Apostolopoulos K, Bous RM, ElNaghy R, et al. Examining the variability of bone and soft tissue morphology in hemifacial microsomia: a case series of 8 patients. J Cranio-Maxillofac Surg. 2021; 49(5): 352–357. https://doi.org/10.1016/j.jcms.2021.02.002
[7] Pruzansky S. Not all dwarfed mandibles are alike. Birth Defect. 1969; 5: 120–129.
[8] Kaban LB, Moses MH, Mulliken JB. Surgical correction of hemifacial microsomia in the growing child. Plast Reconstr Surg. 1988; 82(1): 9–19. https://doi.org/10.1097/00006534-198882010-00003
[9] David DJ, Mahatumarat C, Cooter RD. Hemifacial microsomia: a multisystem classification. Plast Reconstr Surg. 1987; 80(4): 525–35. https://doi.org/10.1097/00006534-198710000-00008
[10] Vento AR, LaBrie RA, Mulliken JB. The OMENS classification of hemifacial microsomia. Cleft Palate Craniofac J. 1991; 28(1): 68–76. https://doi.org/10.1597/1545-1569_1991_028_0068_tomens_2.3.co_2
[11] Horgan JE, Padwa BL, Labrie RA, et al. OMENS-Plus: analysis of craniofacial and extracraniofacial anomalies in hemifacial microsomia. Cleft Palate Craniofac J. 1995; 32(5): 405–12. https://doi.org/10.1597/1545-1569_1995_032_0405_opaoca_2.3.co_2
[12] Fan WS, Mulliken JB, Padwa BL. An association between hemifacial microsomia and facial clefting. J Oral Maxillofac Surg. 2005; 63(3): 330–334. https://doi.org/10.1016/j.joms.2004.10.006
[13] Tuin AJ, Tahiri Y, Paine KM, et al. Clarifying the relationships among the different features of the OMENS+ classification in craniofacial microsomia. Plast Reconstr Surg. 2015; 135(1): 149e–156e. https://doi.org/10.1097/PRS.0000000000000843
[14] Wang X, Chai Y, Zhang Y, et al. Exploration of novel genetic evidence and clinical significance into hemifacial microsomia pathogenesis. J Craniofac Surg. 2023; 34(2): 834–888. https://doi.org/10.1097/SCS.0000000000009167
[15] Losken HW, Preston CB, Evans WG. Hemifacial microsomia. A case report. S Afr Med J. 1983; 64(13): 500–502.
[16] Preston CB, Losken HW, Evans WG. Restitution of facial form in a patient with hemifacial microsomia: a case report. Angle Orthod. 1985;55(3):197–205. https://doi.org/10.1043/0003-3219(1985)055<0197:Roffia>2.0.Co;2
[17] Werler MM, Sheehan JE, Hayes C, et al. Demographic and reproductive factors associated with hemifacial microsomia. Cleft Palate Craniofac J. 2004; 41(5): 494–500. https://doi.org/10.1597/03-110.1
[18] Krüger GC, L’Abbé EN, Stull KE. Sex estimation from the long bones of modern South Africans. Int J Legal Med. 2017; 131(1): 275–285. https://doi.org/10.1007/s00414-016-1488-z
[19] Omotoso BR, Harrichandparsad R, Moodley IG, et al. An anatomical investigation of the proximal vertebral arteries (V1, V2) in a select South African population. Surg Radiol Anat. 2021; 43(6): 929–941. https://doi.org/10.1007/s00276-021-02712-x
[20] Madaree A. Epidemiology of clefts in Kwazulu Natal: Comparison with systematic review analysis, similarities, and differences. J Craniofac Surg. 2023; 34(1): 65–69. https://doi.org/10.1097/SCS.0000000000008957
[21] Kuu-Karkku L, Suominen A, Svedström-Oristo A-L. Craniofacial microsomia – more than a structural malformation. Orthod Craniofac Res. 2023; 26(1): 117–122. https://doi.org/10.1111/ocr.12592
[22] Manlove A, Mitchell B, Abramowicz S. Etiology and anatomical variance in craniofacial microsomia. In: Yates DM, Markiewicz MR, editors. Craniofacial microsomia and treacher collins syndrome: comprehensive treatment of associated facial deformities. Cham: Springer; 2022. p. 3–16.
[23] Cousley RR, Calvert ML. Current concepts in the understanding and management of hemifacial microsomia. Br J Plast Surg. 1997; 50(7): 536–551. https://doi.org/10.1016/s0007-1226(97)91303-5
[24] Xu S, Zhang Z, Tang X, et al. The influence of gender and laterality on the incidence of hemifacial microsomia. J Craniofac Surg. 2015; 26(2): 384–387. https://doi.org/10.1097/SCS.0000000000001336
[25] Rooijers W, Caron C, Loudon S, et al. Ocular and adnexal anomalies in craniofacial microsomia: a systematic review. Int J Oral Maxillofac Surg. 2020; 49(9): 1107–1114. https://doi.org/10.1016/j.ijom.2020.03.003
[26] Renkema RW, Caron CJ, Heike CL, et al. A decade of clinical research on clinical characteristics, medical and surgical treatments for individuals with craniofacial microsomia: what have we learned? J Plast Reconstr Aesthet Surg. 2022; 75(6): 1781–1792. https://doi.org/10.1016/j.bjps.2022.02.058
[27] Singh M, Kaur M, Grewal AM, et al. Ophthalmic features and management outcomes of 30 children having Goldenhar syndrome. Int Ophthalmol. 2020; 40: 667–675. https://doi.org/10.1007/s10792-019-01227-0
[28] Caron C, Pluijmers B, Maas B, et al. Obstructive sleep apnoea in craniofacial microsomia: analysis of 755 patients. Int J Oral Maxillofac Surg. 2017; 46(10): 1330–1337. https://doi.org/10.1016/j.ijom.2017.05.020
[29] Shakir S, Bartlett SP. Modern mandibular distraction applications in hemifacial microsomia. Clin Plast Surg. 2021; 48(3): 375–89. https://doi.org/10.1016/j.cps.2021.02.001
[30] Pluijmers B. On Craniofacial Microsomia shape and surgery [Internet]. PhD thesis. Erasmus University Rotterdam 2019 [cited 2023 Feb 24]. Available from: http://hdl.handle.net/1765/119281
[31] Kaditis AG, Alvarez MLA, Boudewyns A, et al. Obstructive sleep disordered breathing in 2-to 18-year-old children: diagnosis and management. Eur Respir J. 2016; 47(1): 69–94. https://doi.org/10.1183/13993003.00385-2015
[32] Bertin H, Mercier J, Cohen A, et al. Surgical correction of mandibular hypoplasia in hemifacial microsomia: a retrospective study in 39 patients. J Craniomaxillofac Surg. 2017; 45(6): 1031–8. https://doi.org/10.1016/j.jcms.2017.03.016
[33] Meazzini MC, Battista VM, Brusati R, et al. Costochondral graft in growing patients with hemifacial microsomia case series: long‐term results compared with non‐treated patients. Orthod Craniofac Res. 2020; 23(4): 479–485. https://doi.org/10.1111/ocr.12398
[34] Cohen N, Cohen E, Gaiero A, et al. Maxillofacial features and systemic malformations in expanded spectrum hemifacial microsomia. Am J Med Genet. 2017; 173(5): 1208–1218. https://doi.org/10.1002/ajmg.a.38151
[35] Kent RD. Developmental functional modules in infant vocalizations. J Speech Lang Hear Res. 2021; 64(5): 1581–1604. https://doi.org/10.1044/2021_jslhr-20-00703
[36] Zuo KJ, Heinelt M, Ho ES, et al. Dynamic reconstruction of facial paralysis in craniofacial microsomia. Plast Reconstr Surg. 2022; 149(4): 919–929. https://doi.org/10.1097/prs.0000000000008927
[37] Li Q, Zhou X, Wang Y, et al. Facial paralysis in patients with hemifacial microsomia: frequency, distribution, and association with other OMENS abnormalities. J Craniofac Surg. 2018; 29(6): 1633–1637. https://doi.org/10.1097/scs.0000000000004618
[38] Sinclair N, Gharb BB, Papay F, et al. Soft tissue reconstruction in patients with hemifacial microsomia: a systematic review of the literature. J Craniofac Surg. 2019; 30(3): 879–887. https://doi.org/10.1097/scs.0000000000005320
[39] Rollnick BR, Kaye CI, Nagatoshi K, et al. Oculoauriculovertebral dysplasia and variants: phenotypic characteristics of 294 patients. Am J Med Genet. 1987; 26(2): 361–375. https://doi.org/10.1002/ajmg.1320260215
[40] Renkema R, Caron C, Pauws E, et al. Extracraniofacial anomalies in craniofacial microsomia: retrospective analysis of 991 patients. Int J Oral Maxillofac Surg. 2019; 48(9): 1169–1176. https://doi.org/10.1016/j.ijom.2019.01.031
[41] Barisic I, Odak L, Loane M, et al. Prevalence, prenatal diagnosis and clinical features of oculo-auriculo-vertebral spectrum: a registry-based study in Europe. Eur J Hum Genet. 2014; 22(8): 1026–33. https://doi.org/10.1038/ejhg.2013.287