REVIEW ARTICLE
Collagenase clostridium histolyticum for Dupuytren’s disease: a comprehensive systematic review and comparative analysis against percutaneous needle aponeurotomy and limited fasciectomy
Jevan Cevika,b, Rohan Rajarama,b, Michaela Pollocka,b, Ishith Setha,b and Warren M. Rozena,b
aDepartment of Plastic and Reconstructive Surgery, Peninsula Health, Victoria, Australia; bPeninsula Clinical School, Central Clinical School, Faculty of Medicine, Monash University, Victoria, Australia
ABSTRACT
This systematic review compared the efficacy of collagenase clostridium histolyticum (CCH) against percutaneous needle aponeurotomy (PNA) and limited fasciectomy (LF) for Dupuytren’s contracture. Searches were conducted in PubMed, Embase, and Web of Science databases to March 2024. Randomised controlled trials (RCTs) were included. Primary outcomes included successful contracture correction as defined by included studies. Secondary outcomes included recurrence rates, patient-reported outcomes, and adverse events. A total of 11 studies (969 patients) were included. Meta-analysis showed no difference in efficacy between CCH and PNA (Relative Risk [RR]: 1.01, 95% Confidence Interval [CI]: 0.93–1.09). Recurrence rates were also similar (RR: 1.18, 95% CI: 0.95–1.48). Data suggested higher recurrence risk with CCH versus LF (RR: 6.84, 95% CI: 1.59–29.48). In some studies, CCH was associated with higher rates of haematoma, local pain, and oedema. CCH demonstrates comparable efficacy to PNA; however, it may have a higher risk of local complications and recurrence compared to LF. Treatment decisions should be made on a case-by-case basis.
KEYWORDS: Dupuytren’s contracture; collagenase clostridium histolyticum; percutaneous needle aponeurotomy; limited fasciectomy.
Citation: Journal of Plastic Surgery and Hand Surgery 2025; 60: 27–34. DOI: https://doi.org/10.2340/jphs.v60.42750.
Copyright: © 2025 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 12 November 2024; Accepted: 16 December 2024; Published: 13 February 2025
CONTACT Jevan Cevik jevancevik@gmail.com Peninsula Health, 2 Hastings Road, Frankston, 3199 Victoria, Australia
Supplemental data for this article can be accessed online at https://doi.org/10.2340/jphs.v60.42750
Competing interests and funding: The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Introduction
Dupuytren’s disease (DD) is a progressive fibroproliferative disorder involving the palmar fascia of the hand [1]. Characterised by thickening and shortening of the fascia, the condition leads to the gradual development of fixed flexion contractures of the fingers, predominantly affecting the ring and little fingers [2]. This pathological condition, first detailed by Baron Guillaume Dupuytren in 1831, poses significant functional impairment and reduces the quality of life in affected individuals, making effective treatment a crucial area of research in hand surgery [3].
The aetiology of DD is complex and multifactorial, involving genetic predisposition, environmental factors, and microvascular injuries [4,5]. With an ageing population, the incidence of DD is expected to rise, underscoring the need for effective management strategies that can be tailored to the severity of the disease and the specific needs of the patient.
Treatment modalities for DD have evolved significantly over the years, transitioning from invasive techniques to more conservative approaches as understanding of the disease’s pathophysiology advanced [6–9]. The primary aim of treatment is to restore hand function by releasing the fibrotic cords causing contracture. Operative and non-operative treatments are available, with the choice of procedure depending on the stage of the disease, the patient’s functional status, and their personal preferences. While open fasciectomy has previously been considered the gold standard, its associated morbidity and prolonged recovery times have prompted the development and adoption of alternative approaches. Limited fasciectomy (LF), a less extensive version of the traditional open fasciectomy, involves the surgical removal of the diseased fascia while attempting to preserve more of the surrounding healthy tissue [10,11]. This approach aims to balance the need for thorough disease removal with reduced morbidity and faster recovery compared to more radical surgical techniques. However, the invasive nature of surgery, prolonged recovery, and the potential for significant complications such as nerve damage and infection warrant the utilisation of alternative treatment options for many patients.
One treatment, collagenase clostridium histolyticum (CCH) injection has emerged as a notable non-surgical option. CCH is an enzyme derived from Clostridium histolyticum bacteria that specifically targets and breaks down type I and III collagen, the primary components of Dupuytren’s cords [12–14]. The treatment involves injecting CCH directly into the cord, followed by manipulation of the affected finger after 24–72 hours to rupture the weakened cord. This method has shown promise in reducing contracture with a simple, in-office procedure that allows rapid recovery and minimal downtime [15].
Another non-surgical technique, percutaneous needle aponeurotomy (PNA), uses a needle to puncture and weaken the cord tissue, allowing the fingers to be manipulated back into extension [8,9,16]. This technique, which can be performed under local anaesthesia, has gained popularity due to its low complication rate and quick recovery time. However, concerns about its long-term efficacy and recurrence rates have led to ongoing debates about its place in the treatment algorithm.
Given the variations in treatment efficacy, safety, and patient-centric outcomes, a review comparing these treatments is warranted. This systematic review aims to compare CCH against the other two primary treatment modalities – PNA and LF – and evaluate the comparative effectiveness, safety, and patient-reported outcomes among these treatments.
Methods
Study identification
This systematic review adhered to the Preferred Reporting in Systematic Review and Meta-Analysis (PRISMA) guidelines (Supplementary Figure 1), and was listed on the International Prospective Register of Systematic Reviews (PROSPERO) [17]. A comprehensive search was conducted to identify relevant studies comparing the use of CCH against PNA and LF for treating DD. PubMed, Embase, and Web of Science databases were searched from their inception until March 2024. The following search terms were used: (‘Dupuytren*’ OR ‘Dupuytren’s contracture’ OR ‘Dupuytren’s disease’ OR ‘palmar fibromatosis’) AND (‘collagenase Clostridium histolyticum’ OR ‘CCH’ OR ‘Xiaflex’ OR ‘Xiapex’) AND (‘percutaneous needle fasciotomy’ OR ‘percutaneous needle aponeurotomy’ OR ‘PNF’ OR ‘PNA’ OR ‘needle fasciotomy’ OR ‘needle aponeurotomy’ OR ‘limited fasciectomy’ OR ‘partial fasciectomy’ OR ‘fasciectomy’). The search was not limited by language to minimise the risk of language bias. The reference lists of all included studies and relevant reviews were screened for any additional studies.
Study inclusion
Inclusion criteria were as follows: studies of human participants, study design was limited to prospective randomised control trials (RCTs), the included outcomes were either the rate of intervention success (as indicated by the study) or the relevant scores on secondary outcome scoring systems utilised (e.g. Quick Disabilities of the Arm, Shoulder, and Hand Score (Q-DASH) [18] or Unité Rhu-matologique des Affections de la Main Score (URAM) [19]. Only studies that provided sufficient data to calculate relative risks (RR), or mean differences with 95% confidence intervals (CI) were eligible for consideration of meta-analysis.
Exclusion criteria included: non-randomised cohort studies, case control studies, case reports, reviews, conference presentations, cross-sectional studies, editorials, letters to the editor, lack of relevant outcomes reported.
Data extraction
Titles and abstracts of all identified articles in the search were reviewed by two independent reviewers (JC/RR), and any discrepancies were resolved through discussion and consensus or the involvement of a third reviewer where necessary. Data were extracted into data extraction tables. These data points included the first author, publication year, country of the study, age, sample size, definition of primary outcome success, number of patients successfully achieving the primary outcome, follow up time, and the secondary outcomes utilised. The latest outcome data were recorded when outcomes were reported at multiple time points in the study.
Risk of bias assessment
The risk of bias for the included studies was evaluated using the Cochrane Risk of Bias (ROB) tool, designed explicitly for RCTs [20]. This tool is extensively utilised to assess the potential for bias within randomised trials and includes seven key domains prone to bias: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessors, completeness of outcome data, selective reporting, and other bias. The assessment was conducted independently by two reviewers (JC/RR). Discrepancies between reviewers were resolved through discussion, and, if necessary, a third reviewer was consulted to reach a consensus. In relation to the blinding of participants and personnel, it is often impractical to blind study participants in such trials; therefore, studies were typically assigned a high risk of bias in this category.
Statistical analysis
A meta-analysis was performed to determine the overall relative effect size for comparing the efficacy of CCH with PNA and LF. The outcome measure of a reduction of joint contracture to <5° was chosen as the primary comparator between studies given that this was the most commonly reported outcome measure among included studies and deemed an outcome measure that is reproducible with a low chance of bias. Furthermore, meta-analyses of the risk of recurrence between treatment modalities at the end of reported follow up times were conducted. Additional meta-analyses evaluated the relative effectiveness of these treatment modalities using the Q-DASH and URAM scoring systems employed across the studies. Heterogeneity among studies was quantified using the I2 statistic, and pooled risk ratios along with 95% CI were calculated employing random-effects models. An I2 statistic greater than 50% was interpreted as indicating high heterogeneity. All statistical analyses were carried out using the Review Manager software version 5.4 [21].
Results
Literature search
From the initial search, a total of 593 studies were identified. After the removal of duplicate records, 522 unique studies were available for further evaluation. These studies underwent an initial screening based on their titles and abstracts. As a result, 65 studies were deemed relevant and were selected for a detailed full-text review. Furthermore, 8 additional studies were screened from citations of relevant articles. Following this, 11 publications ultimately met the criteria for inclusion in the study (Supplementary Figure 1).
Study characteristics
The included studies were published between 2016 and 2024. At the end of follow up, sample sizes ranged from 21 to 187 participants, totalling 969 patients across all included studies (Table 1). All studies were conducted in Nordic countries such as Sweden, Denmark, or Finland – except two studies, one by Abe et al. in 2020 which originated from Japan and one by Thoma et al. in 2023 originating from Canada. All studies evaluated the comparative efficacy of CCH with either PNA and/or LF. Ten studies compared CCH with PNA and two compared CCH with LF. Follow-up periods varied from 12 months to 5 years. Outcome measures were varied in the manner in which success was reported; yet, most included studies evaluated the number of patients that reached a reduction of joint contracture to <5°. Several secondary patient reported outcome measures were also assessed among the included studies, including Q-DASH and URAM scores most commonly.
| Author | Year | Country | CCH (n) | PNA (n) | Joints treated | Definition of success | Achieved successful outcome, n (%) | Secondary outcomes | Follow up* | Definition of recurrence | Recurrence rate |
| Scherman (A)** [22] | 2016 | Sweden | 39 | 42 | MCP + PIP | Reduction in total passive extension deficit (TPED) | Median reduction: CCH = 70% PNA = 70% |
Q-DASH Score URAM Score |
12 months | Recurrence of ≥20° of joint contracture | CCH = 4 (10%) PNA = 5 (12%) |
| Stromberg (A) [23] | 2016 | Sweden | 67 | 71 | MCP | Reduction of MCP contracture to <5° | CCH = 60 (90%) PNA = 64 (90%) |
URAM Score VAS |
12 months | Recurrence of ≥20° of joint contracture | CCH = 1 (1%) PNA = 1 (1%) |
| Skov [24] | 2017 | Denmark | 24 | 19 | PIP | Reduction of MCP contracture to <5° | CCH = 0 (0%) PNA = 1 (5%) |
DASH Score | 24 months | Recurrence of ≥20° of joint contracture | CCH = 20 (83%) PNA = 13 (68%) |
| Stromberg (B) [25] | 2017 | Sweden | 20 | 19 | MCP | Reduction of MCP contracture to <5° | CCH = 19 (95%) NF = 18 (95%) |
VAS | 12 months | Recurrence of ≥20° of joint contracture | CCH = 0 (0%) NF = 1 (5%) |
| Scherman (B)** [26] | 2018 | Sweden | 36 | 40 | MCP + PIP | Reduction in total passive extension deficit (TPED) | Median reduction: CCH = 51% PNA = 75% |
Q-DASH Score URAM Score |
36 months | Recurrence of ≥30° of joint contracture | CCH = 12 (33%) PNA = 17 (43%) |
| Stromberg (C)** [27] | 2018 | Sweden | 76 | 76 | MCP + PIP | Reduction of joint contracture to <5° | CCH = 58 (76%) PNA = 60 (79%) |
Q-DASH Score URAM Score VAS |
24 months | Recurrence of ≥20° of joint contracture | CCH = 10 (13%) PNA = 9 (12%) |
| Abe** [28] | 2020 | Japan | 31 | 31 | MCP + PIP | Reduction of joint contracture to <5° | CCH = 31 (100%)† PNA = 31 (100%)† |
Q-DASH Score URAM Score |
36 months | Recurrence of ≥20° of joint contracture | CCH = 8 (26%) PNA = 9 (29%) |
| Bystrom [29] | 2022 | Sweden | 45 | 57 | MCP | Reduction of joint contracture to <5° | CCH = 23 (51%)‡ PNA = 27 (47%)‡ |
Q-DASH Score URAM Score |
60 months | Recurrence of ≥20° of joint contracture | CCH = 36 (56%) PNA = 30 (45%) |
| Jorgensen [30] | 2022 | Denmark | 32 | 36 | MCP | Reduction in total passive extension deficit (TPED) | Median reduction: CCH = 67% PNA = 79% |
Q-DASH Score | 36 months | Recurrence of ≥30° of joint contracture OR reintervention | CCH = 17 (47%) PNA = 6 (19%) |
| Raisanen** [31] | 2024 | Finland | 92 | 95 | MCP + PIP | Reduction of joint contracture to <5° | CCH = 32 (34%) PNA = 23 (24%) |
Q-DASH Score VAS EQ-5D EQ-5D-3L Score |
24 months | Reintervention | CCH = 9 (10%) PNA = 10 (10%) |
| CCH: Collagenase Clostridium Histolyticum; PNA: Percutaneous Needle Aponeurotomy; MCP: Metacarpophalangeal joint; PIP: Proximal interphalangeal joint; Q-DASH: Quick Disabilities of the Arm, Shoulder, and Hand Score; URAM: Unité Rhu-matologique des Affections de la Main Score; VAS: Visual Analogue Score; EQ-5D: European Quality of Life 5 Dimensions Score; EQ-5D-3L: European Quality of Life 5 Dimensions 3 Level Version Index Score; TPED: Total Passive Extension Deficit; NR: Not Reported. *Longest follow up time period reported in the included studies is reported here. **Results presented reflect changes to the MCPJ. †Results reported at 30 days of follow up. ‡A number of patients were excluded from final analysis due to re-treatment. Scherman 2018 is a study of the same patients as Scherman 2016 with longer follow up. Stromberg 2017 enrolled a sub-population of patients from Stromberg 2016. |
|||||||||||
Risk of bias
Study quality was assessed using Cochrane Risk of Bias 2 Tool (Supplementary Figures 2 & 3). Randomisation and adherence bias was minimal across the examined studies. All papers used validated methods, either computer generated or manual, to randomise patients to their intervention. Furthermore, given the surgical nature of the interventions, adherence generally was not an issue. Some patients were required to wear night splints; however, across the board, authors report good adherence to this. Attrition bias was also low except in the Thoma et al. 2023 study where 36% of the initial study population (22) were lost to follow up. The largest source of bias within all papers was in blinding of outcome assessors. While some papers attempted to blind investigators to the intervention, other papers either did not attempt this, or made mention of the potential for patients to reveal their intervention to the investigators. Given the nature of the interventions, it was not possible to blind patients to the treatment they had received in the included studies. Thus, all studies scored high risk for this risk of bias.
CCH versus PNA
Ten studies reported the success of CCH treatment compared with PNA (Table 1). Of these, five studies were eligible for quantitative meta-analysis given that they used comparable outcome measures and patient populations. Pooled meta-analysis showed no significant difference in success rates at the end of follow up between CCH and PNA (RR: 1.01, 95% CI: 0.93 to 1.09) (Figure 1). Heterogeneity among the studies was low (I2 = 30%). Similarly, no significant difference in rates of recurrence were observed between the two treatment modalities (RR: 1.18, 95% CI: 0.95 to 1.48, I2 = 0%) (Figure 2). URAM scores were also comparable between the two groups (standardised mean difference [SMD]: 0.12, 95% CI: −0.35 to 0.59, I2 = 74%) (Supplementary Table 1, Figure 3). Lastly, Q-DASH scores were also not significantly different between the two groups among included studies in quantitative analysis (SMD: 0.08, 95% CI: −0.13 to 0.29, I2 = 0%) (Supplementary Table 1, Figure 4).
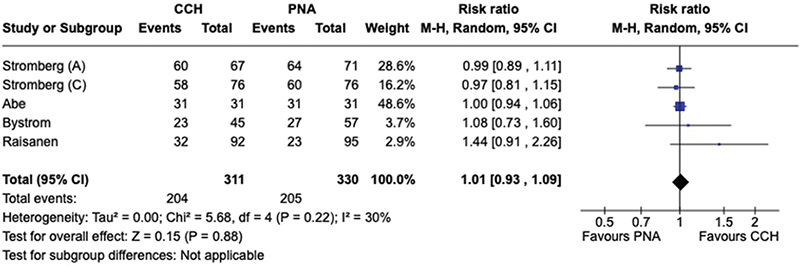
Figure 1. Forest plot displaying meta-analysis of studies comparing collagenase clostridium histolyticum (CCH) with percutaneous needle aponeurotomy (PNA) using a reduction in joint contracture to <5° as a marker of success.
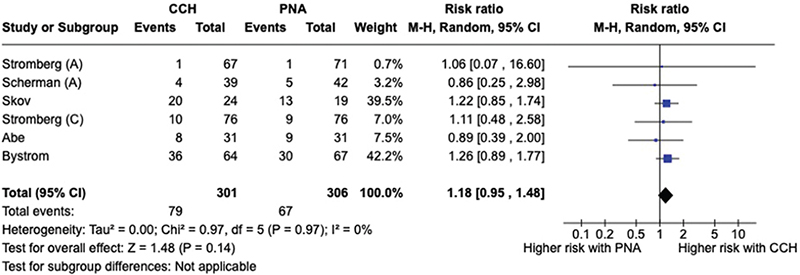
Figure 2. Forest plot displaying meta-analysis of studies comparing risk of recurrence of collagenase clostridium histolyticum (CCH) versus percutaneous needle aponeurotomy (PNA).
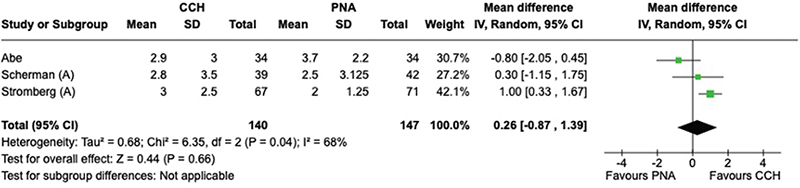
Figure 3. Forest plot displaying meta-analysis comparing Unité Rhu-matologique des Affections de la Main (URAM) scores for collagenase clostridium histolyticum (CCH) versus percutaneous needle aponeurotomy (PNA).
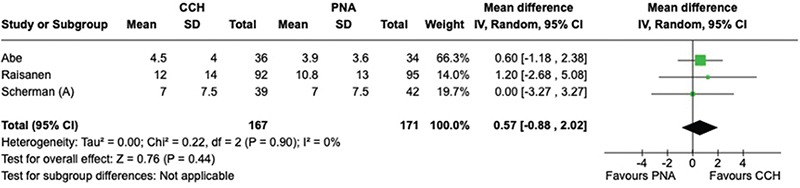
Figure 4. Forest plot displaying meta-analysis comparing Quick Disabilities of the Arm, Shoulder, and Hand Score (Q-DASH) scores for collagenase clostridium histolyticum (CCH) versus percutaneous needle aponeurotomy (PNA).
CCH versus LF
Only two studies reported results comparing CCH to LF (Table 2). Unfortunately, no comparable outcome measure was reported between the two studies to allow for quantitative analysis of the two studies. One study by Thoma et al. in 2023 showed no significant difference scores on the Michigan Hand Questionnaire (MHQ) as their primary outcome [32,33]. Furthermore, they found no difference in URAM scores between the two cohorts (Supplementary Table 2). Another study by Raisanen et al. in 2024 displayed comparable success rates between CCH and LF; however, they reported a statistically significant increased risk of recurrence/reintervention for CCH when compared with LF (Table 2) [31]. A meta-analysis of the risk of recurrence of CCH versus LF was performed which displayed a greater risk of recurrence with CCH compared with LF (RR: 6.84, 95% CI: 1.59 to 29.48, I2 = 0%) (Figure 5).
| Author | Year | Country | CCH (n) | LF (n) | Joints treated | Primary outcome | Achieved primary outcome, n (%) | Secondary outcomes | Follow up* | Definition of recurrence | Recurrence rate |
| Thoma [33] | 2023 | Canada | 8 | 13 | MCP + PIP + DIP | MHQ Score | No difference in MHQ scores between the two groups | HUI-3 Score URAM Score SDSS Score ROM of Digits |
12 months | Reintervention | CCH = 3 (23%) LF = 1 (12.5%) |
| Raisanen [31] | 2024 | Finland | 92 | 97 | MCP + PIP | Reduction of joint contracture to <5° | CCH = 32 (34%) LF = 40 (41%) |
Q-DASH Score VAS EQ-5D EQ-5D-3L Score |
24 months | Reintervention | CCH = 9 (10%)** LF = 1 (1%)** |
| CCH: Collagenase Clostridium Histolyticum; LF: Limited Fasciectomy; MCP: Metacarpophalangeal joint; PIP: Proximal interphalangeal joint; DIP: Distal interphalangeal joint; MHQ: Michigan Hand Questionnaire; URAM: Unité Rhu-matologique des Affections de la Main Score; HUI-3: The Health Utility Index-3; SDSS: Southampton Dupuytren Scoring Scheme. *Longest follow up time period reported in the included studies is reported here. **Statistically significant difference. |
|||||||||||
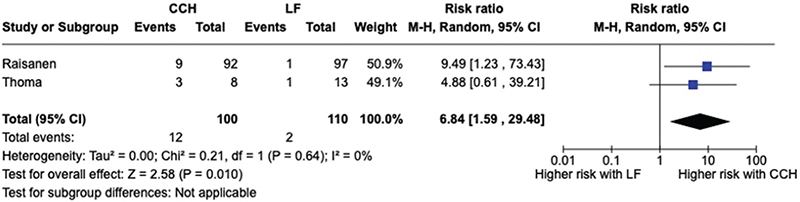
Figure 5. Forest plot displaying meta-analysis of studies comparing risk of recurrence of collagenase clostridium histolyticum (CCH) versus percutaneous needle aponeurotomy (PNA).
Complications
Complications were regularly reported among the included studies (Supplementary Table 3). Studies were significantly heterogenous in the manner in which they reported adverse complications from the various treatments. Twenty different complications and their respective rates among the included studies are displayed in Supplementary Table 3. It was deemed that given the significant heterogeneity and lack of standardised assessment between studies, quantitative meta-analysis of these results was not feasible. Skin rupture was the most commonly reported complication among the included studies. Among each study individually, there was no statistically significant difference in rates of skin rupture between CCH and PNA. Yet, in one study by Stromberg et al. in 2016 the size of the skin rupture was significantly larger in the CCH group compared to the PNA cohort [23]. The authors also reported a higher rate of haematoma with the use of CCH when compared with PNA. Another study by Skov et al. in 2017 found a significantly higher rate of complications in the CCH cohort (mainly pain and local oedema) when compared with their PNA cohort [24]. Additionally, Abe et al. displayed significantly greater rates of complications in their CCH group than in PNA [28]. Overall, a narrative for a greater rate of complications (particularly haematoma, local pain and local oedema) has been associated with the use of CCH when compared with PNA. Comparisons between the rate of complications between CCH and LF were much more limited (Supplementary Table 3)
Discussion
This systematic review and meta-analysis compared the efficacy, recurrence rates, and patient-reported outcomes of CCH against PNA and LF for the treatment of DD. The results suggest that CCH has comparable efficacy to PNA in terms of achieving contracture correction, with no significant differences in success rates or recurrence at follow-up. However, CCH appears to have a higher risk of recurrence compared to LF; although data comparing these two modalities was limited.
Meta-analysis demonstrated no significant difference in success rates between CCH and PNA in achieving contracture correction to less than 5° at the end of follow up (RR: 1.01, 95% CI: 0.93 to 1.09). This suggests that both minimally invasive techniques are similarly effective in the short-term management of Dupuytren’s contractures. This finding aligns with previous studies that have shown both techniques to be effective treatment options for diseased [6,8,9,15,16]. Importantly, there was also no significant difference in recurrence rates between CCH and PNA (RR: 1.18, 95% CI: 0.95 to 1.48). This is a key consideration, as the durability of treatment effect is important for decision making and the long-term management of DD. The similar recurrence rates suggest that neither technique offers a clear advantage in terms of long-term efficacy.
In contrast, the comparison between CCH and LF revealed a significantly higher risk of recurrence with CCH (RR: 6.84, 95% CI: 1.59 to 29.48). This finding must be interpreted cautiously due to the limited number of studies (only two) comparing these modalities directly. Nevertheless, it aligns with the general understanding that more invasive techniques like LF may offer more reliable and long-lasting results, albeit at the cost of increased surgical morbidity.
The analysis of patient-reported outcomes using standardised measures like the Quick Disabilities of the Arm, Shoulder, and Hand (Q-DASH) score and the Unité Rhumatologique des Affections de la Main (URAM) score showed no significant differences between CCH and PNA, suggesting that from the patient’s perspective, both treatments result in similar functional improvements and satisfaction levels. The lack of difference in these scores is particularly relevant as it captures the patient’s experience of treatment outcomes, which may not always correlate directly with objective measures of contracture correction.
When looking at complications, this review revealed a trend towards a higher rate of certain adverse events with CCH compared to PNA, particularly haematoma, local pain, and local oedema. However, the heterogeneity in reporting complications across studies made it challenging to perform adequate quantitative comparative meta-analyses of these outcomes. The higher rate of certain complications with CCH may be attributed to its mechanism of action, which involves enzymatic degradation of collagen, potentially leading to more local tissue reactions compared to the mechanical action of PNA. Skin ruptures were commonly reported for both CCH and PNA, with no consistent significant difference between the two treatments. This complication, while generally minor, is an important consideration for patient counselling and post-procedure care. The similar rates of skin rupture may suggest that this risk is inherent to the process of cord disruption, regardless of whether it is achieved enzymatically or mechanically. Some studies reported higher rates of local pain, oedema and haematoma with CCH, which may impact short-term recovery and patient comfort. However, these effects were generally transient and did not appear to significantly affect long-term outcomes or patient satisfaction.
The findings of this review have several important clinical implications. Firstly, the comparable efficacy and recurrence rates between CCH and PNA suggest that both treatments can be considered viable options for the management of Dupuytren’s contractures in appropriate patient populations. The choice between these two modalities may therefore depend on other factors such as physician expertise, patient preference, cost considerations, and specific patient characteristics. The potential for higher recurrence rates with CCH compared to LF highlights the need for careful patient selection. Patients with more severe or recurrent disease may benefit more from LF, while those with milder disease or those prioritising quicker recovery might be better suited for CCH or PNA. The similar patient-reported outcomes between CCH and PNA are reassuring, indicating that both treatments lead to meaningful improvements in hand function and quality of life from the patient’s perspective. This underscores the value of these less invasive approaches in the management of DD.
This review has several limitations that should be considered. The heterogeneity in outcome measures and follow-up periods across studies made it challenging to combine all available data in meta-analyses. The limited number of studies directly comparing CCH to LF restricts our ability to draw firm conclusions about their relative efficacy and safety. In addition, the follow-up periods in most included studies were relatively short, which may not capture the full picture of long-term recurrence rates and outcomes. DD is a chronic, progressive condition, and longer-term studies are needed to fully understand the durability of treatment effects. Future research should focus on standardising outcome measures and complication reporting to facilitate more robust comparisons between treatment modalities. Long-term follow-up studies are crucial to better understand the recurrence patterns and need for retreatment with different approaches. Additionally, studies examining cost-effectiveness and patient satisfaction over time would provide valuable information for clinical decision-making.
Conclusion
This systematic review and meta-analysis suggest that CCH is comparable to PNA in terms of efficacy, recurrence rates, and patient-reported outcomes for the treatment of Dupuytren’s contractures. While CCH may have a higher risk of recurrence compared to LF, more studies are needed to confirm this finding. The choice of treatment should be individualised based on disease severity, patient preferences, and the balance between efficacy, rates of recurrence and potential complications. As our understanding of DD and its management continues to evolve, ongoing research will be crucial to refine treatment algorithms and improve long-term outcomes for patients with this condition.
Statement of human and animal rights
This article does not contain any studies with human or animal subjects.
Contributorship
Literature review and data collection: J.C., R.R. Writing initial draft: J.C. Critical review and critique: All authors. Data analysis: J.C., R.R., I.S. Conceptualisation: All authors. Supervision: W.M.R. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
References
[1] Hueston J, Tubiana R. Dupuytren’s disease. Churchill Livingstone: Edinburgh; 1974.
[2] Badalamente MA, Stern L, Hurst LC. The pathogenesis of Dupuytren’s contracture: contractile mechanisms of the myofibroblasts. J Hand Surg Am. 1983;8(3):235–243. https://doi.org/10.1016/s0363-5023(83)80150-6
[3] Peltier LF. Guillaume Dupuytren and Dupuytren’s fracture. Surgery. 1958;43(5):868–874.
[4] Sayadi LR, Alhunayan D, Sarantopoulos N, et al. The molecular pathogenesis of Dupuytren disease: review of the literature and suggested new approaches to treatment. Ann Plast Surg. 2019;83(5):594–600. https://doi.org/10.1097/sap.0000000000001918
[5] Riester S, van Wijnen A, Rizzo M, et al. Pathogenesis and treatment of Dupuytren disease. JBJS Rev. 2014;2(4):e2. https://doi.org/10.2106/jbjs.Rvw.M.00072
[6] Hurst LC, Badalamente MA, Hentz VR, et al. Injectable collagenase clostridium histolyticum for Dupuytren’s contracture. N Engl J Med. 2009;361(10):968–979. https://doi.org/10.1056/NEJMoa0810866
[7] Hueston JT. Dupuytren’s contracture: the trend to conservatism. Ann R Coll Surg Engl. 1965;36(3):134–151.
[8] Eaton C. Percutaneous fasciotomy for Dupuytren’s contracture. J Hand Surg Am. 2011;36(5):910–915. https://doi.org/10.1016/j.jhsa.2011.02.016
[9] Foucher G, Medina J, Navarro R. Percutaneous needle aponeurotomy: complications and results. J Hand Surg Br. 2003;28(5):427–431. https://doi.org/10.1016/s0266-7681(03)00013-5
[10] Hueston JT. Limited fasciectomy for Dupuytren’s contracture. Plast Reconstr Surg Transplant Bull. 1961;27:569–585. https://doi.org/10.1097/00006534-196106000-00001
[11] Zachariae L. Dupuytren’s contracture. How limited should a limited fasciectomy be? Scand J Plast Reconstr Surg. 1969;3(2):145–149. https://doi.org/10.3109/02844316909036705
[12] Starkweather KD, Lattuga S, Hurst LC, et al. Collagenase in the treatment of Dupuytren’s disease: an in vitro study. J Hand Surg Am. 1996;21(3):490–495. https://doi.org/10.1016/s0363-5023(96)80368-6
[13] Badalamente MA, Hurst LC. Efficacy and safety of injectable mixed collagenase subtypes in the treatment of Dupuytren’s contracture. J Hand Surg Am. 2007;32(6):767–774. https://doi.org/10.1016/j.jhsa.2007.04.002
[14] Badalamente MA, Hurst LC. Enzyme injection as nonsurgical treatment of Dupuytren’s disease. J Hand Surg Am. 2000;25(4):629–636. https://doi.org/10.1053/jhsu.2000.6918
[15] Watt AJ, Curtin CM, Hentz VR. Collagenase injection as nonsurgical treatment of Dupuytren’s disease: 8-year follow-up. J Hand Surg Am. 2010;35(4):534–539, 539.e1. https://doi.org/10.1016/j.jhsa.2010.01.003
[16] Pess GM, Pess RM, Pess RA. Results of needle aponeurotomy for Dupuytren contracture in over 1,000 fingers. J Hand Surg Am. 2012;37(4):651–656. https://doi.org/10.1016/j.jhsa.2012.01.029
[17] Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. https://doi.org/10.1136/bmj.n71
[18] Gummesson C, Ward MM, Atroshi I. The shortened disabilities of the arm, shoulder and hand questionnaire (QuickDASH): validity and reliability based on responses within the full-length DASH. BMC Musculoskelet Disord. 2006;7:44. https://doi.org/10.1186/1471-2474-7-44
[19] Bernabé B, Lasbleiz S, Gerber RA, et al. URAM scale for functional assessment in Dupuytren’s disease: a comparative study of its properties. Joint Bone Spine. 2014;81(5):441–444. https://doi.org/10.1016/j.jbspin.2014.01.007
[20] Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. https://doi.org/10.1136/bmj.l4898
[21] Review Manager (RevMan) [Computer program] Version 5.4, The Cochrane Collaboration; 2020.
[22] Scherman P, Jenmalm P, Dahlin LB. One-year results of needle fasciotomy and collagenase injection in treatment of Dupuytren’s contracture: a two-centre prospective randomized clinical trial. J Hand Surg Eur Vol. 2016;41(6):577–582. https://doi.org/10.1177/1753193415617385
[23] Strömberg J, Ibsen-Sörensen A, Fridén J. Comparison of treatment outcome after collagenase and needle fasciotomy for Dupuytren contracture: a randomized, single-blinded, clinical trial with a 1-year follow-up. J Hand Surg Am. 2016;41(9):873–880. https://doi.org/10.1016/j.jhsa.2016.06.014
[24] Skov ST, Bisgaard T, Søndergaard P, et al. Injectable collagenase versus percutaneous needle fasciotomy for Dupuytren contracture in proximal interphalangeal joints: A randomized controlled trial. J Hand Surg Am. 2017;42(5):321–328.e3. https://doi.org/10.1016/j.jhsa.2017.03.003
[25] Strömberg J, Vanek P, Fridén J, et al. Ultrasonographic examination of the ruptured cord after collagenase treatment or needle fasciotomy for Dupuytren’s contracture. J Hand Surg Eur Vol. 2017;42(7):683–688. https://doi.org/10.1177/1753193417711594
[26] Scherman P, Jenmalm P, Dahlin LB. Three-year recurrence of Dupuytren’s contracture after needle fasciotomy and collagenase injection: a two-centre randomized controlled trial. J Hand Surg Eur Vol. 2018;43(8):836–840. https://doi.org/10.1177/1753193418786947
[27] Strömberg J, Ibsen Sörensen A, Fridén J. Percutaneous needle fasciotomy versus collagenase treatment for Dupuytren contracture: a randomized controlled trial with a two-year follow-up. J Bone Joint Surg Am. 2018;100(13):1079–1086. https://doi.org/10.2106/jbjs.17.01128
[28] Abe Y. Comparison of treatment outcomes after collagenase injection and percutaneous needle fasciotomy for Dupuytren’s contracture: objective and subjective comparisons with a 3-year follow-up. Plast Reconstr Surg. 2020;145(6):1464–1474. https://doi.org/10.1097/prs.0000000000006828
[29] Byström M, Ibsen Sörensen A, Samuelsson K, et al. Five-year results of a randomized, controlled trial of collagenase treatment compared with needle fasciotomy for Dupuytren contracture. J Hand Surg Am. 2022;47(3):211–217. https://doi.org/10.1016/j.jhsa.2021.11.019
[30] Jørgensen RW, Jensen CH, Jørring S. Three-year recurrence of Dupuytren contracture after needle fasciotomy or collagenase injection: a randomized controlled trial. Plast Reconstr Surg. 2023;151(2):365–371. https://doi.org/10.1097/prs.0000000000009847
[31] Räisänen MP, Leppänen OV, Soikkeli J, et al. Surgery, needle fasciotomy, or collagenase injection for Dupuytren contracture: a randomized controlled trial. Ann Intern Med. 2024;177(3):280–290. https://doi.org/10.7326/m23-1485
[32] Shauver MJ, Chung KC. The Michigan hand outcomes questionnaire after 15 years of field trial. Plast Reconstr Surg. 2013;131(5):779e–787e. https://doi.org/10.1097/PRS.0b013e3182865d83
[33] Thoma A, Murphy J, Gallo L, et al. Randomized controlled trial comparing the clinical effectiveness of collagenase injection (Xiaflex®) and palmar fasciectomy in the management of Dupuytren’s contracture. Plastic Surgery. 2024;32(4):659–666. https://doi.org/10.1177/22925503231161066