REVIEW ARTICLE
Trigger finger and carpal tunnel syndrome: a meta-analysis of co-occurrence and risk
Péter Sallaia,b, Barbara Sebőkc, Luca Hergárd,e and Judit Réka Hetthéssye,f,g
aSt. Pantaleon Hospital, Dunaújváros, Hungary; bSaska-Med Bt. Dunaújváros, Hungary; cDepartment of Pediatric Traumatology, Dr. Manninger Jenő Trauma Center, Budapest, Hungary; dDepartment of Orthopaedics, Semmelweis University, Budapest, Hungary; eCentre for Translational Medicine, Semmelweis University, Budapest, Hungary; fHand Clinic, Budapest, Hungary; gResearch Management Workgroup, Semmelweis University, Budapest, Hungary
ABSTRACT
Carpal tunnel syndrome (CTS) and trigger finger (TF) are two of the most common conditions of the hand. Co-occurrence is mentioned by a number of publications, but there are few high-level evidence studies that summarise the results of large databases to quantify the chances of concurrency in detail making it difficult to gauge clinical significance. We aimed to quantify the impact of CTS, TF and surgery for these conditions on the prevalence of the other condition. Systematic review was based on PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, with registration in the PROSPERO database. TF is clearly more common with CTS and after CTS surgery, so it is important to seek out symptoms of TF, even the initial ones, at every examination performed for CTS. Thus, conservative treatment of TF maybe started in time and TF surgery may be performed in conjunction with CTS surgery. Level of Evidence: IV. Prospero registration number: CRD42022382672
KEYWORDS: CTS; carpal tunnel syndrome; trigger finger; fingers; risk factor
Citation: Journal of Plastic Surgery and Hand Surgery 2025; 60: 102–108. DOI: https://doi.org/10.2340/jphs.v60.43199.
Copyright: © 2025 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 26 December 2024; Accepted: 16 February 2025; Published: 5 May 2025
CONTACT Judit Réka Hetthéssy drhjr612@gmail.com Budapest 1085, Üllői út 26.; 1428 Budapest, Pf.: 2. Hungary
Competing interests and funding: The authors report there are no competing interests to declare.
The authors received no financial support for the research, authorship and/or publication of this article.
Introduction
Carpal tunnel syndrome (CTS) and trigger finger (TF) are considered to be two of the most common conditions of the hand. Incidence of CTS is estimated to be 2.2–5.4% per 1,000 population and has an estimated prevalence of 1–5% [1, 2]. CTS can also occur in the paediatric population, though quite rarely, usually related to genetic diseases, most commonly to metabolic disorders associated with lysosomal overload [3]. TF has been described to have a prevalence of around 2–10% [4–7]. The co-occurrence of these conditions was mentioned by a number of previous publications; however, there are few high-level evidence studies/meta-analyses that summarise the results of large databases to quantify the chances of concurrency in detail.
The more accurate the information we have about this relationship, the better we can optimise the impact of these conditions on the patient’s life. If such conditions are detected early enough, long-term complications can be prevented more effectively; and early conservative treatment may help avoid further surgery and missed or delayed diagnoses may better be avoided [8–10].
The shortest possible duration of treatment is also beneficial for the cost bearer, as the treatment of these patients consumes considerable work load and resources; examinations and treatment tie up considerable health worker capacity and many physician and staff hours go into the treatment of CTS and TF patients [11]. The cost of caring for these patients is not negligible [12–14]. This can be optimised to a significant extent by mapping the co-occurrence of the two conditions well.
The aetiology of CTS and TF is multifactorial [1]. The localisation of both lesions is characterised by a relative lack of space, which may be exacerbated by synovial thickening of the tendons due to possible load [15]; this may lead directly to the development of symptoms [16]. The underlying risk factors are similar. International literature recognises following risk factors: female gender [17–19], obesity, diabetes [19, 20], rheumatoid arthritis and hypothyroidism [17].
The aim of our work was to quantify the impact of CTS, TF and surgery for these conditions on the prevalence of the other condition, the distribution of TF in the fingers when TF alone is present or in the presence of CTS. We also analysed the impact of certain concurrent diseases (DM-diabetes mellitus, RA-rheumatoid arthritis, thyroid disorder) and patient factors (male or female, right or left hand) in the presence of CTS and TF on the prevalence of the other condition.
Our hypothesis is that certain diseases or conditions may play a role as risk factors for the co-occurrence or sequential occurrence of CTS and TF.
Materials and methods
Protocol and registration
This systematic review was conducted according to the guidelines of the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement. Our study protocol was registered in the PROSPERO database.
Eligibility criteria
Eligibility was determined based on our predefined PICO (Population, Intervention, Comparison, Outcomes) framework. We included experimental studies, retrospective and prospective observational studies and randomised controlled studies with the adult population (P). We selected publications with patients who had CTS or TF (I); with group of patients who developed TF after CTS or after CTS release/developed CTS after TF or after TF operation. We compared these groups with those where we experienced the absence of CTS or TF (C). The above incidence rates were compared (O).
We excluded studies of different forms and studies where the number of subjects was under 10, as well as meta-analyses, the systematic reviews, the review articles and guidelines.
Systematic search
We executed a systematic search of the following databases: MEDLINE (via PubMed), Embase and Cochrane Central Register of Controlled Trials (CENTRAL) on the 7th of January 2023. We used the following search key: ([carpal tunnel syndrome OR CTS] AND [trigger finger]). We have not used any restrictions or filters. Reference lists of eligible articles and citing articles (via Google Scholar search engine) have also been screened to capture all relevant studies.
Study selection and data retrieval
Two independent authors screened the titles and abstracts of the studies and selected the ones corresponding to our eligibility criteria. Then the two authors sorted the remaining articles based on full text. In cases of non-agreement, a senior author decided on the inclusion of the study.
For data extraction, we used a standardised data extraction form. One of the reviewers extracted data from all the included studies using Microsoft Excel, which was verified by another author. The following data were extracted: first author, year of publication, study type, country of study, population of the study, inclusion and exclusion criteria, number and gender of patients, mean age. Outcomes included number, age, BMI (body mass index) of patients with TF; number of previous TF surgeries among TF patients; incidence of CTS, diabetes, rheumatoid arthritis and thyroid disorder among TF patients. Outcomes also included number, age, BMI of patients with CTS; number of previous CTS surgeries among CTS patients; incidence and distribution per finger of TF among CTS patients; incidence of diabetes, rheumatoid arthritis and thyroid disorder among CTS patients. Discrepancies were resolved by discussion and the involvement of the senior researcher. Articles where data reporting was inconsistent were excluded from the systematic review.
Statistical analysis
Statistical analysis is performed using the RevMan 5.4 program. We used the inverse variance method to create the weights assigned to the different studies. Because we expect heterogeneity between studies, we use a random effects model to pool effect sizes. We use the DerSimonian–Laird estimator (DerSimonian & Laird 1986) to calculate heterogeneity variance. Knapp–Hartung corrections (Knapp & Hartung 2003) are used to calculate the confidence interval around the pooled effect. The results are plotted on a forest graph.
Risk of bias and applicability
The quality of the included studies was assessed by two independent authors, according to the QUIPS tool. Disagreements were resolved by a third author.
Grade
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to assess the certainty of evidence for each of our outcomes.
Ethics
No ethical approval was required for this systematic review and meta-analysis, as all data were already published in peer-reviewed journals. No patients were involved in the design, conduct or interpretation of our study.
Results
Important articles
The 26 scientific publications included in our meta-analysis included a total of 66,862 cases. Of these, 44,152 were women and 19,442 were men; 3,268 cases were without specification of gender. Thus, based on the number of cases of known sex, 69.43% were female and 30.57% were male. The mean age of the patients was found in 22 publications; the mean age was 54.08 years.
The 26 scientific publications reviewed included 47,581 patients with CTS and 23,995 patients with TF, so the number of patients with CTS was about twice that of patients with TF. There were 21,675 cases of carpal tunnel release (CTR); of these, 437 cases of TF were detected before CTR (2.02%). On the basis of the 18 articles in which all three data were found, in 19,814 operated cases of CTS, a total of 232 cases of TF were detected before CTR (1.17%) and 2,177 cases after CTR (10.99%).
Number of CTS and TF cases, TF distribution frequency
Based on 19,136 reported cases of TF surgery a total of 635 cases of CTS were detected before TF surgery (3.32%) and 103 cases after the surgery (0.54%). Based on the four articles that included all three data, 18,710 operated TF cases had 635 cases of CTS before TF surgery (3.39%) and 103 cases after (0.55%).
This suggests that CTR increased the incidence of TF; the reverse was not true.
In 11 articles, 1,137 TF cases were identified with 8,007 cases and their exact location is shown in Figure 1a.
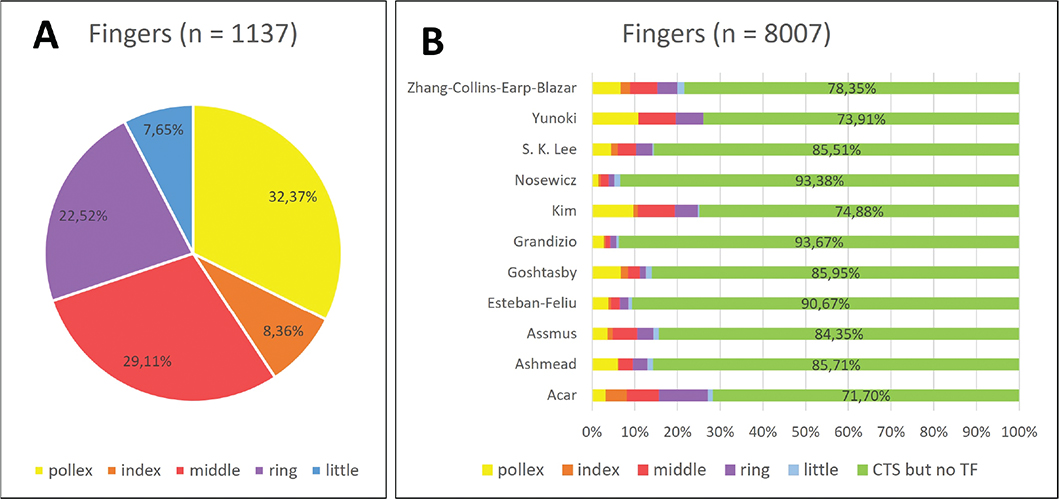
Figure 1. (A) the distribution of TF with CTS in cases with known localisation. (B) the distribution of TF cases with concomitant CTS.
When looking at the distribution of the TF cases in CTS, the TF was most common on the thumb (4.60%), followed by the middle (4.13%) and ring finger (3.20%), the index (1.19%) and little finger (1.09%). The overall incidence rate of TF with concomitant CTS was 14.2% (Figure 1b).
Thus, when looking at the distribution of TF that appeared alongside CTS, the thumb (32.37%) was the most common, followed by the middle (29.11%) and ring (22.52%) fingers, and the index (8.35%) and little (7.54%) fingers were the least common.
Of the selected articles, only Rottger’s communication reported the localisation of a single TF without the appearance of CTS. This showed a 17% incidence on the thumb and index finger, 23% on the middle finger, 24% on the ring finger and 18% on the little finger.
The relationship between CTS and TF
TF as underlying disease, population characteristics, association with CTS
A total of 11 publications approached the association between CTS and TF from the direction of the TF as an underlying disease, with a total of 19,923 cases of TF. Of these publications, four commented on the average age of the subjects, which was 55.54 years out of 3,768 cases. BMI was reported in two articles, 30 out of 1,273 cases (both publications reported a mean BMI of 30). Seven publications reported a total of 928 cases of CTS among the 19,780 patients with TF evaluated in these articles, 4.59%; 19.310 patients with TF, 3,585 DM patients were detected, 18.57%; four publications report a total of 224 RA patients out of 17,035 cases, 1.31% and three articles report 24 thyroid patients out of 571 patients with TF (4.20%).
CTS as an underlying disease, population characteristics, correlation with TF
Twenty articles included CTS as a primary disease reporting 41,300 cases. CTS cases were identified. Of these, seven articles stated the average age of the subjects, which was 57.81 years out of 4,542 cases. Data on BMI was reported in three articles, this was 28 out of 3,045 cases. A total of 19 publications mention a total of 4,265 TF occurrences among 41,233 CTS patients evaluated in these articles, representing 10.34%; 4,916 DM patients were detected among 37,088 CTS patients, representing 13.25%; eight publications mention a total of 790 RA patients among 19,054 cases, representing 4.15% and nine articles mention 1,191 thyroid patients among 20,140 CTS patients, representing 5.91%. This is summarised in Table 1.
Prevalence of CTS and TF in the presence of comorbidities and according to patient characteristics
Based on these data, we aimed to investigate whether these comorbidities (DM, RA, thyroid disorder) or individual characteristics (male or female, right or left hand) increase the prevalence of CTS in patients with CTS compared to patients with TF or TF.
Data on a given categorical variable were considered sufficient if they were included in at least three communications. The data set of four correlations met this criterion; the role of DM, RA, thyroid disorder and male/female characteristics in the occurrence of TF in CTS patients could be examined on the basis of these correlations, as well as the effect of the co-existence of CTS and DM on TF in different fingers. The presence or absence of significance of comorbidity or trait was determined by Fisher exact test; a significant association was defined as p < 0.05. For TF, no meaningful association was found for the prevalence of CTS for the listed comorbidities/disease characteristics.
The results of the processing showed that in patients with CTS, DM and female gender increased the rate of TF occurrence; however, there was no significant association between the presence of RA and thyroid disorder (Table 2a-d).
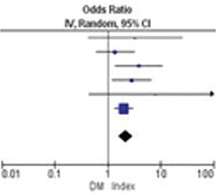
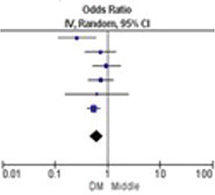
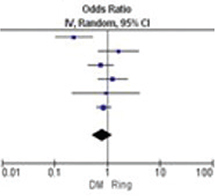
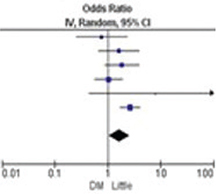
Our results showed that the co-existence of CTS and DM was significantly associated with TF in the pollex, index, middle and little finger, but not in the ring finger. Of the above, the most consistent findings (minimal heterogeneity) were for TF in the index finger (Table 3).
| Study or Subgroup | DM | Odds Ratio | Odds Ratio | Odds Ratio | Odds Ratio | Odds Ratio | ||||||
| Total | Events | Weight | IV, Random, 95% Cl | Weight | IV, Random, 95% Cl | Weight | IV, Random, 95% Cl | Weight | IV, Random, 95% Cl | Weight | IV, Random, 95% Cl | |
| Ashmead, 2020 | 315 | 22 | 16.0% | 0.10 [0.05, 0.21] | 2.3% | 3.30 [0.43, 25.13] | 10.5% | 0.26 [0.12, 0.60] | 15.1% | 0.23 [0.10, 0.52] | 11.6% | 0.77 [0.25, 2.35] |
| Goshtasby, 2010 | 427 | 66 | 17.7% | 0.20 [0.11, 0.35] | 13.7% | 1.38 [0.60, 3.18] | 14.0% | 0.73 [0.37, 1.45] | 13.7% | 1.65 [0.68, 3.98] | 15.7% | 1.65 [0.68, 3.98] |
| Grandizio, 2014 | 1217 | 214 | 18.6% | 0.27 [0.17, 0.43] | 9.2% | 3.89 [1.41, 10.77] | 17.0% | 0.96 [0.53, 1.75] | 20.2% | 0.75 [0.43,1.32] | 18.9% | 184 [0.87, 3.88] |
| Nosewicz, 2019 | 967 | 219 | 17.3% | 1.05 [0.57, 1.93] | 13.0% | 2.83 [1.20, 6.65] | 18.3% | 0.75 [0.43,1.32] | 18.2% | 1.27 [0.67, 2.42] | 22.8% | 1.05 [0.57, 1.93] |
| Yunoki, 2019 | 46 | 11 | 10.3% | 0.44 [0.12, 1.67] | 1.1% | 8.10 [0.44, 147.76] | 4.3% | 0.63 [0.16, 2.49] | 7.1% | 0.94 [0.22, 4.11] | 2.3% | 8.10 [0.44, 147.76] |
| Zhang-Collins-Earp-Blazar, 2019 | 1386 | 261 | 20.1% | 0.52 [0.40, 0.69] | 60.7% | 2.01 [1.36, 2.99] | 35.8% | 0.55 [0.41, 0.73] | 25.7% | 0.86 [0.63, 1.16] | 28.7% | 2.67 [1.72, 4.14] |
| Total events | 4358 | 793 | 100.0% | 033 [0.18, 061] | 100.0% | 2.18 [1.60, 2.97] | 100.0% | 0.62 [0.46, 0.84] | 100.0% | 0.81 [0.52, 1.27] | 100.0% | 1.65 [1.05, 2.60] |
| Study or Subgroup | DM | Odds Ratio IV, Random, 95% Cl | Odds Ratio IV, Random, 95% Cl | Odds Ratio IV, Random, 95% Cl | Odds Ratio IV, Random, 95% Cl | Odds Ratio IV, Random, 95% Cl | |
| Total | Events | ||||||
| Ashmead, 2020 | 315 | 22 | 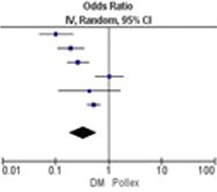 |
 |
 |
 |
 |
| Goshtasby, 2010 | 427 | 66 | |||||
| Grandizio, 2014 | 1217 | 214 | |||||
| Nosewicz, 2019 | 967 | 219 | |||||
| Yunoki, 2019 | 46 | 11 | Heterogenity: Tau2 = 0.45; Chi2 = 35.00, df = 5 (P < 0.00001); I2 = 86% Test for overall effect: Z = 3.59 (P = 0.0003) |
Heterogenity: Tau2 = 0.00; Chi2 = 3.86, df = 5 (P = 0.57); l2=0% Test for overall effect: Z = 4.96 (P < 0.00001) |
Heterogenity: Tau2 = 0.04; Chi2 = 7.49, df = 5 (P = 0.19); I2 = 33% Test for overall effect: Z = 3.13(P = 0.002) |
Heterogenity: Tau2 = 0.18; Chi2=13.75, df = 5 (P = 0.02); I2 = 64% Test for overall effect: Z = 09.2 (P = 0.36) |
Heterogenity: Tau2 = 0.14; Chi2 = 9.43, df = 5 (P = 0.09); I2 = 47% Test for overall effect: Z = 2.18 (P = 0.03) |
| Zhang-Collins-Earp-Blazar, 2019 | 1386 | 261 | |||||
| Total events | 4358 | 793 | |||||
| (a) Pollex, we found a significant association (odds ratio [OR]: 0.33; 95% confidence interval [CI]: 0.18–0.61; p < 0.00003), and I2 = 86% significantly heterogeneous. (b) Index showed a significant correlation (OR: 2.18; 95% CI: 1.60–2.97; p < 0.00001), and I2 = 0% homogeneous. (c) Middle, we found a significant association (OR: 0.62; 95% CI: 0.46–0.84; p = 0.002), and I2 =33% moderately heterogeneous. (d) Ring significant correlation not proven. (e) Little showed a significant association (OR: 1.65; 95% CI: 1.05–2.60; p = 0.03), and I2 = 47% moderately heterogeneous. |
|||||||
Discussion
Our results suggest a correlation between CTS and the appearance of TF. Based on the data from the published patient dataset, the prevalence of CTS in the study population was higher than that of TF; the number of CTS was approximately twice that of TF. The incidence of TF was more frequent with CTS than without; in patients operated on with TF, about six times as many cases of CTS were detectable before TF surgery than after. This suggests that the presence of CTS increases the likelihood of the occurrence of TF.
Considering the concomitant presence of CTS and TF is especially important in the presence of factors that have been shown to increase the incidence of TF as well as CTS, such as female gender [17, 18] or diabetes [20].
Of particular note are the characteristics of the post-operative appearance of TF following CTS surgery. The incidence of TF after CTS surgery is reported in the literature to be between 4 and 31.3% [18, 20, 21]. Our analysis of the data showed that the incidence of TF in patients who underwent CTS surgery was about 10 times higher after surgery (10.99%) than before (1.17%).
These statistically significant incidence associations (six times more frequent with CTS and 10 times more frequent after CTS surgery than without) point to the need to address the associations at the clinical level; it is important to extend the examination of patients with symptoms of CTS to include those of TF, which may be present at the time of examination with clinically insignificant symptoms. Simultaneous testing is also of particular importance because TF not only increases in number, but may present with clinical symptoms within a relatively short time (6 months) after CTS surgery [22]. Further treatment or surgery at a later date means that the patient is further prevented from working and taking up sports or leisure activities. Consecutive treatments over time also doubles the burden on the healthcare provider in terms of workload and costs. However, if detected early, the patient may receive conservative treatment appropriate for TF or, if justified, TF may be operated on in conjunction with CTS.
However, according to the data examined, TF surgery does not increase the risk of developing CTS; although there is a study in the literature supporting this association [4]. In any case, even in patients presenting with symptoms of TF, it is advisable to pay attention to possible symptoms of CTS, because in addition to the prominent TF complaints, there may be CTS complaints that the patient does not attach importance to. We therefore suggest that the examining physician should ask patients regarding hand numbness or pain outright. We consider it appropriate and simultaneously feasible to investigate the Tinel and Phalen signal and measuring 2-point discrimination in patients with TF. This may ensure the detection of the concomitant presence of CTS, which is essential for the treatment of both diseases.
Several studies address the distribution of TF between the fingers of the hand. Based on these results TF occurs most frequently on the thumb, followed by the middle, ring and index fingers; it has been described to occur most rarely on the little finger [15]. If was found that the presence of CTS leads to the same outcome [22]. This means that we do not have to screen patients regarding location of TF based on whether they have CTS or not. However, it may be seen that the chances of any finger being affected are not negligible in any of these cases, so we recommend the examination of all fingers always.
It should also be borne in mind that the development of both CTS and TF is a process; under both conditions, the same patient may present with different intensity of symptoms at different times. This is particularly true for the different severity of symptoms of CTS and TF in cases where one condition is associated with the other. We also have to take into consideration the fact that TF may also develop in several locations on a hand at different times, even on all fingers at times. It also points out that when examining a patient at any time for any of these conditions, we should expect to see symptoms of any stage of another condition. We also consider it important that patients are aware of the symptoms of both conditions and should be educated about these during the examinations. In agreement with the findings of several studies, we recommend that patients before or after CTS surgery should be informed about the potential risk of TF and its treatment options [17, 20, 23]. The best way to ensure patient follow-up is by involving the patient equipping them with the necessary knowledge regarding their condition.
In processing the data, we also sought to determine whether patients with CTS have comorbidities or other characteristics that increase the incidence of TF. There are sources that show the relevance of thyroid disease [17], while other studies had shown that thyroid disease does not play a role in increasing the risk of TF in addition to CTS [18]. According to some authors [20, 24] the association with diabetes is clear; other authors [17, 18, 25] found that no such relationship could be demonstrated. In our meta-analysis, female gender and diabetes clearly increased the incidence of TF in CTS patients, while rheumatic disease and thyroid disease had no effect.
The associations shown in our meta-analysis carry substantial clinical relevance. In addition to the above regarding patient assessment and follow-up, special attention should be paid to the symptoms of diabetic patients with CTS and/or women with TF. For people with thyroid disease or rheumatic disease, the meta-analysis did not support the need for increased attention.
The strength of our meta-analysis lies in the fact that the patient population underlying the reviewed publications was large and was treated using standard methodology, applying standard surgical protocols and postoperative care for patients as declared by the publications.
A limitation of our meta-analysis is that individual papers have taken different approaches to the CTS–TF relationship or its sub-issues.
Conclusion
TF is clearly more common with CTS and after CTS surgery, so it is important to pay attention to the symptoms of TF, even the initial ones, at every examination performed for CTS. Thus, conservative treatment of TF maybe started in time, and in justified cases, TF surgery may be performed in conjunction with CTS surgery. However, TF may occur much later after CTS and may develop on different fingers at different times. However, TF does not increase the chance of CTS. The same distribution of TF between the fingers of the hand can be expected without and with CTS, always requiring examination on all fingers. Among the comorbidities and other characteristics, female gender and diabetes are noteworthy; in these cases, the chances of a joint occurrence are even higher.
Authors contribution
Péter Sallai MD, Luca Hergár MD, and Judit Réka Hetthéssy MD, PhD: conceptualisation. Péter Sallai MD, Barbara Sebők: literature search, screening the records, data extraction, assessing the quality of the included studies. Barbara Sebők: statistical analysis. Péter Sallai MD, Luca Hergár MD, Barbara Sebők, and Judit Réka Hetthéssy MD, PhD: writing the first draft of the current manuscript. Judit Réka Hetthéssy MD, PhD, Luca Hergár MD, Barbara Sebők and Péter Sallai MD: critical revision of the manuscript and approving the submitted draft. All the authors provided critical conceptual input and approved the final version of the manuscript. All authors are accountable for all aspects of the work.
Data availability
The datasets used in this study are available in the full text articles included in this systematic review and meta-analysis.
References
[1] Campos-Serna I, Garcia-Espinoza JA, Cahuana-Quispe AI, et al. Diagnosis and treatment of carpal tunnel syndrome in a tertiary care center in Mexico City. World J Plast Surg. 2020;9(2):213–218. https://doi.org/10.29252/wjps.9.2.213
[2] Shen P-C, Chang P-C, Jou IM, et al. Hand tendinopathy risk factors in Taiwan: a population-based cohort study. Medicine (Baltimore).2019;98(1):e13795.https://doi.org/10.1097/MD.0000000000013795
[3] Leti Acciaro A, Pilla F, Faldini C, et al. The carpal tunnel syndrome in children. Musculoskelet Surg. 2018;102(3):261–265. https://doi.org/10.1007/s12306-017-0527-3
[4] Hsieh HH, Wu WT, Shih JT, et al. Incidence of carpal tunnel syndrome requiring surgery may increase in patients treated with trigger finger release: a retrospective cohort study. Clin Epidemiol. 2022;14:1079–1086. https://doi.org/10.2147/CLEP.S383397
[5] Fitch MS, Thiese MS, Wood EM, et al. The Coexistence of carpal tunnel syndrome in workers with trigger digit. Hand (New York, NY). 2021;16(6):753–758. https://doi.org/10.1177/1558944719893048
[6] Patel B, Kleeman SO, Neavin D, et al. Shared genetic susceptibility between trigger finger and carpal tunnel syndrome: a genome-wide association study. Lancet Rheumatol. 2022;4(8):e556–e565.
[7] Shafaee-Khanghah Y, Akbari H, Bagheri N. Prevalence of carpal tunnel release as a risk factor of trigger finger. World J Plast Surg. 2020;9(2):174–178. https://doi.org/10.29252/wjps.9.2.174
[8] Yamazaki A, Matsuura Y, Kuniyoshi K, et al. A1 pulley stretching treats trigger finger: A1 pulley luminal region under digital flexor tendon traction. Clin Biomech (Bristol, Avon). 2020;72:136–140.
[9] Mifune Y, Inui A, Sakata R, et al. High-resolution ultrasound in the diagnosis of trigger finger and evaluation of response to steroid injection. Skeletal Radiol. 2016;45(12):1661–1667. https://doi.org/10.1007/s00256-016-2485-5
[10] Merry SP, O’Grady JS, Boswell CL. Trigger finger? Just shoot! J Prim Care Community Health. 2020;11:2150132720943345. https://doi.org/10.1177/2150132720943345
[11] Meyer MA, Tarabochia MA, Goh BC, et al. The impact of resident involvement on outcomes and costs in elective hand and upper extremity surgery. J Hand Surg. 2022. https://doi.org/10.1016/j.jhsa.2022.02.006
[12] de Boccard O, Müller C, Christen T. Economic impact of anaesthesia methods used in hand surgery: global costs and operating room’s throughput. J Plastic Reconstr Aesthet Surg. 2021;74(9):2149–2155.
[13] Harris AHS, Meerwijk EL, Kamal RN, et al. Variability and costs of low-value preoperative testing for carpal tunnel release surgery. Anesth Analg. 2019;129(3):804–811. https://doi.org/10.1213/ANE.0000000000004291
[14] Lalchandani GR, Halvorson RT, Rahgozar P, et al. Wide-awake local anesthesia for minor hand surgery associated with lower opioid prescriptions, morbidity, and costs: a nationwide database study. J Hand Surg Glob Online. 2020;2(1):7–12.
[15] Assmus H. Carpal tunnel syndrome and stenosing tenosynovitis. Nervenarzt. 2000;71(6):474–476. https://doi.org/10.1007/s001150050609
[16] Hombal JW, Owen R. Carpal tunnel decompression and trigger digits. Hand. 1970;2(2):192–196.
[17] Goshtasby PH, Wheeler DR, Moy OJ. Risk factors for trigger finger occurrence after carpal tunnel release. Hand Surg. 2010;15(2):81–87. https://doi.org/10.1142/S0218810410004606
[18] Nosewicz J, Cavallin C, Cheng C-I, et al. Factors associated with trigger digit following carpal tunnel release. World J Orthop. 2019;10(12):454–462.
[19] Ferree S, Neuhaus V, Becker SJ, et al. Risk factors for return with a second trigger digit. J Hand Surg Eur Vol. 2014;39(7):704–707. https://doi.org/10.1177/1753193412469129
[20] Grandizio LC, Beck JD, Rutter MR, et al. The incidence of trigger digit after carpal tunnel release in diabetic and nondiabetic patients. J Hand Surg. 2014;39(2):280–285. https://doi.org/10.1016/j.jhsa.2013.10.023
[21] Acar MA, Kütahya H, Güleç A, et al. Triggering of the digits after carpal tunnel surgery. Ann Plast Surg. 2015;75(4):393–397. https://doi.org/10.1097/SAP.0000000000000233
[22] Lin F-Y, Manrique OJ, Lin C-L, et al. Incidence of trigger digits following carpal tunnel release: a nationwide, population-based retrospective cohort study. Medicine (Baltimore). 2017;96(27):e7355. https://doi.org/10.1097/MD.0000000000007355
[23] Ashmead Dt, Okada H, Macknin J, et al. Trigger fingers after open carpal tunnel release. Plast Surg (Oakv). 2020;28(4):192–195. https://doi.org/10.1177/2292550320928554
[24] Chammas M, Bousquet P, Renard E, et al. Dupuytren’s disease, carpal tunnel syndrome, trigger finger, and diabetes mellitus. J Hand Surg. 1995;20(1):109–114. https://doi.org/10.1016/S0363-5023(05)80068-1
[25] Lee HI, Lee JK, Yoon S, et al. Carpal tunnel release can be a risk factor for trigger finger: National Health Insurance data analysis. Int Orthop. 2022;46(4):867–873. https://doi.org/10.1007/s00264-022-05312-5