ORIGINAL RESEARCH ARTICLE
Medial gastrocnemius flap: infection control in megaprostheses
Rana Kapukayaa , Gazi Kutalmış Yaprakb, Asena Ayça Özdemirc and Ahmet Kapukayad
, Gazi Kutalmış Yaprakb, Asena Ayça Özdemirc and Ahmet Kapukayad
aDepartment of Plastic Reconstructive and Aesthetic Surgery, Adana City Hospital, Adana, Turkey; bPlastic Reconstructive and Aesthetic Surgery, Çukurova University, Medical Faculty Hospital, Adana, Türkiye; cDepartment of Medical Education, Mersin University, Mersin, Türkiye; dDepartment of Orthopedics and Traumatology, Adana City Hospital, Adana, Türkiye
ABSTRACT
Introduction: Medial gastrocnemius flaps are commonly employed in conjunction with endoprosthesis implantations for the management of malignant tumors affecting the proximal segment of the tibia. This study aimed to evaluate the effect of the routine transfer of the muscle on the incidence of infections within the surgical field.
Methods: Forty-three patients presenting with a suspected malignant tumor in the proximal segment of the cruris underwent evaluation at our hospital. The enrolled patients were stratified into two cohorts. Patients in Group 1 (n = 16) underwent a combined procedure involving a medial gastrocnemius flap and a megaprosthesis, whereas patients in Group 2 (n = 17) did not undergo flap surgery.
Results: In Group 1, osteosarcoma (OS) was diagnosed in seven patients (43%). Subsequently, oncologic resection with a wide margin was performed on the affected bone region, resulting in an average defect length of mean 12.81 ± 5.05 cm. The patients in this group were followed-up for an average duration of 34.06 ± 13.21 months. Similarly, in Group 2, OS was present in seven patients (41.17%), and they underwent identical oncologic resection procedures. The mean defect length in Group 2 was measured at mean 14.12 ± 4.54 cm. The average follow-up period for patients in Group 2 was 30.41 ± 12.06 months.
Conclusion: Within Group 1, four patients (25%) experienced infections within the surgical site, while within Group 2, five patients (29.4%) exhibited such infections (p > 0.05). The utilization of megaprostheses in osseous defect repair, either alone or in combination with gastrocnemius flaps, did not yield statistically significant differences in infection rates.
KEYWORDS: Gastrocnemius flap; megaprosthesis; infection; proksimal tibia
Citation: Journal of Plastic Surgery and Hand Surgery 2025; 60: 109–113. DOI: https://doi.org/10.2340/jphs.v60.43537.
Copyright: © 2025 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 11 November 2024; Accepted: 31 March 2025; Published: 14 May 2025
CONTACT: Rana Kapukaya dr__rana@hotmail.com Department of Plastic Reconstructive and Aesthetic Surgery, Adana City Hospital, Adana, Turkey
Competing interests and funding: The authors declare that no funds, grants, or other support were received during the preparation of this manuscript. Local ethics committee approval was obtained before the study was conducted. Obtaining patient consent and collecting information were carried out in accordance with the criteria specified in the Declaration of Helsinki. Patients were informed about sharing information regarding their treatment and surgery. The patient has given written and verbal permission (approval) to share information, documents, pictures, and documents related to his treatment and surgery.
Introduction
Surgical site infection represents the most concerning complication in megaprostheses placed in large defects following the resection of tumor tissue located in extremities. Additionally, megaprosthesis infections, which are highly resistant to treatment, constitute one of the most significant undesirable yet preventable causes of amputation. The literature reports that the proximal tibia is the most commonly affected site by infection [1–3].
In contemporary oncological surgery for musculoskeletal tumors, substantial strides have been achieved owing to advancements in medical science, imaging modalities, megaprosthesis technology, and pharmacotherapy. Nevertheless, despite these advancements, certain preventable complications persist, presenting ongoing challenges to surgeons. The proximal tibia region emerges as one of the areas exhibiting the highest post-oncologic resection complication rates compared to other anatomical regions. Among these complications, surgical site infection, characterized by its recalcitrance to treatment, severe sequelae, and potential for disability, continues to be prominently documented in this region. Surgical site infections typically manifest following megaprosthesis surgeries, with a notable incidence observed within the initial postoperative year. It is noteworthy that surgical site infections account for approximately a quarter of all postoperative complications associated with the aforementioned surgical procedure [4]. This incidence is markedly elevated in cohorts subjected to radiotherapy, after revision surgeries, and among individuals with expandable prostheses, exhibiting rates ranging between 21 and 36% [5–9].
Anatomically, the proximal anteromedial region of the cruris is comparatively weaker than other areas due to its thin skin and limited subcutaneous fat tissue. Surgical interventions for malignant tumors in this area are notably aggressive. Adhering to radical oncological principles, such procedures may result in considerable defects affecting both soft tissue and bone. Literature highlights insufficient soft tissue coverage and inadequate postoperative support as major contributors to heightened rates of surgical site infections. Consequently, diverse surgical approaches have been devised to mitigate these complications. Moreover, clinicians have extensively investigated the impact of well-vascularized pedicled muscle flaps applied to these regions on the incidence of surgical site infections, aiming for optimal soft tissue integration. Among these methodologies, the gastrocnemius flap technique stands out as the most favored and widely endorsed. In the literature, some authors claim a significant decrease in surgical site infection rates, from 36 to 12%, associated with the utilization of this flap technique [10]. On the other hand, some authors have reported contrarily that these flaps do not have a significant effect on surgical site infection rates [11]. However, despite all the different opinions and debates, the effect of gastrocnemius flaps on infection rates has not yet been thoroughly investigated.
Drawing from the perspectives mentioned earlier, this study aimed to assess the impact of gastrocnemius flaps on surgical site infection rates and to analyze the potential influential variables.
Materials and methods
Regional ethics committee approval was obtained before starting the study (Ethics Committee Decision No: 92-21-1624). This study was planned and conducted in accordance with the Ethical Standards specified in the Declaration of Helsinki.
Patient selection and study design
A retrospective analysis was conducted on 43 patients diagnosed with localized malignant tumors in the proximal tibia segment. Among them, thirty-three patients who underwent postoperative follow-up for a minimum of 12 months were enrolled in the study. Ten patients with a follow-up duration of less than 12 months or who died from their primary diseases before this period were excluded. Resection of the extremity regions containing tumors was performed in accordance with oncological principles, ensuring a wide margin. Subsequently, the resected bone areas were reconstructed using appropriate megaprostheses for all patients. The participants were stratified into two groups for comparative analysis. Group 1 (n = 16) received medial gastrocnemius flaps in conjunction with megaprostheses for defect reconstruction, whereas Group 2 (n = 17) did not undergo flap transfer. Additionally, the extra-compartmental aspect of the tumor served as a defining criterion for group allocation, with only patients having tumors confined to the bone being included in Group 2.
Clinical evaluation, comprising discharge, edema, pain, local temperature increase, and redness, constituted the primary method for identifying infection presence. Infection rates and factors influencing infections were subsequently analyzed and compared between the two groups.
This study did not evaluate critical factors that could influence infection risk, such as comorbidities, smoking habits, body mass index (BMI), diabetes, operative time, prior surgical procedures, and vascular status. This limitation represents a significant shortfall in our methodology and warrants careful interpretation of the results. We acknowledge this as a key limitation of the study and emphasize the importance of incorporating these parameters into future research.
Gastrocnemius flap technique
Following oncological resection, the reconstruction of the extremity’s defect adhered to rigorous reconstructive surgical principles. The medial gastrocnemius muscle was accessed by making a medial or posterior midline incision. The muscle was carefully dissected proximally, and its elevation was achieved. The sural artery pedicle was preserved in the popliteal fossa during dissection. A subcutaneous tunnel was created. The flap was rotated and passed through the subcutaneous tunnel. Anteriorly, it was transposed onto the megaprosthesis. It was fixed to the soft tissue in the lateral region with polyglactin sutures [12]). After providing adequate soft tissue support, a negative pressure drain was placed on the megaprosthesis to prevent the hematoma development. The skin was primarily repaired. Antibiotic administration persisted until the commencement of adjuvant therapies, typically spanning up to 14 days, overseen by infectious disease specialists. Isometric exercises were started 24 h later. Patients wore the splint for a duration of 1 week.
Blood tests
Blood tests were performed 1 day before surgery (preoperative) and within 7 days after surgery (postoperative). In these examinations, C reactive protein (CRP), white blood cell (WBC) count, creatinine, and albumin values were examined.
Statistical analysis
Normality control of continuous variables was evaluated with the Shapiro Wilk test. Parametric methods were used for variables that showed normal distribution, and non-parametric methods were used for variables that did not. In comparisons between groups, the Independent Sample t test and the Mann Whitney U test were applied depending on the normality of the data. The Chi-Square test and Fisher’s Exact test were applied to analyze categorical data. Receiver Operating Characteristic (ROC) Analysis was applied for variables that could be discriminatory for infection, and cut-off points were determined. Also for pairwise comparison of ROC curves, the DeLong et al.’s method was used [13]. Data analysis was evaluated in TIBCO Statistica (TIBCO Software Inc., Palo Alto, California, USA), MedCalc Statistical Software (MedCalc Software bv, Ostend, Belgium).
Results
In Group 1 (n = 16), the mean age was 21 years (range 15–28.5), comprising seven females and nine males. Histopathological diagnoses included osteosarcoma (OS) in seven (43.8%) patients, Ewing sarcoma (EWS) in four, undifferentiated pleomorphic sarcoma (UPS) in two, malignant giant cell bone tumor (MGCBT) in one, and synovial sarcoma (SS) in two patients. Thirteen patients underwent chemotherapy, while three received chemoradiotherapy. The tumor tissue length within the bone averaged 10.75 ± 5.13 cm, the width of tumor tissue in the frontal plane was 8.69 ± 3.94 cm, and the width in the sagittal plane was 8.75 ± 4.71 cm. Following resection of tumorous tissue with a wide margin, the mean bone defect length was 12.81 ± 5.05 cm. Patients were monitored for an average of 34.06 ± 13.21 months, during which infection was observed in four (25%) patients within this group.
In Group 2 (n = 17), the mean age was 22 years (min 14.5–max 29.5), consisting of 10 females and seven males. Histopathological diagnoses included OS in seven patients (41.2%), three with EWS, three with SS, two with UPS, and two with MGCBT. The mean tumor tissue length within the bone was 12.24 ± 4.7 cm, the width frontal plane was 9.41 ± 4.35 cm, and the width in the sagittal plane was 9.82 ± 4.17 cm. Fifteen patients received chemotherapy, while two underwent chemoradiotherapy. Following the resection of tumorous tissue with a wide margin, the mean defect length was 14.12 ± 4.54 cm. Patients were monitored for an average of 30.41 ± 12.06 months, during which infection was observed in five patients (29.4%). All patients with OS and EWS underwent neoadjuvant chemotherapy. No additional reconstructive interventions were required in this group, as no soft tissue defects occurred in the anterior region, and primary closure of tissues was achieved (Figure 1).
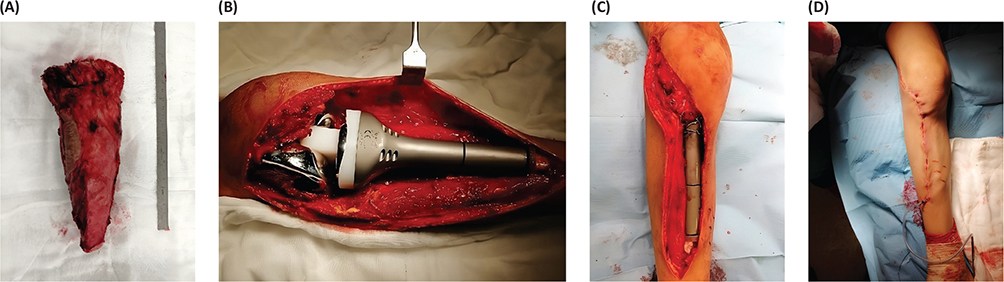
Figure 1. (A) Resected tumor tissue; (B) Repair of proximal tibial defect with megaprosthesis; (C) Soft tissue reconstruction without transferring gastrocnemius flap; (D) Primary repair of skin and subcutaneous tissues.
No statistically significant differences were observed between the two groups regarding age (p = 0.763), reoperation (p = 0.958), preoperative tumor size on magnetic resonance imaging (length p = 0.392, width in frontal plane p = 0.709, and width in sagittal plane p = 0.204), and defect size after resection (p = 0.440) (Tables 1 and 2). In blood tests performed after surgery, there was no statistically significant difference: CRP (p:0.184), WBC (p:0.952), albumin (p:0.062), and creatinine (p:0.177) levels between both groups (Table 3).
| Group 1 (n:16) | Group 2 (n:17) | P | |||||
| Mean ± SD | Median [IQR] | Min-Max | Mean ± SD | Median [IQR] | Min-Max | ||
| L | 10.75 ± 5.13 | 10 [6.25–15] | 4–21 | 12.24 ± 4.7 | 11 [8–16.5] | 5–19 | 0.392a |
| WFP | 8.69 ± 3.94 | 7 [6–11] | 4–17 | 9.41 ± 4.35 | 7 [6–14.5] | 5–17 | 0.709b |
| WSP | 8.75 ± 4.71 | 7.5 [6.25–9] | 3–20 | 9.82 ± 4.17 | 9 [7.5–11] | 4–20 | 0.204b |
| Defect after resection | 12.81 ± 5.05 | 12 [8.25–17] | 7–23 | 14.12 ± 4.54 | 13 [10–18] | 7–21 | 0.440a |
| IQR; Interquartile. Group 1: Gastrocnemius flap applied, Group 2: No gastrocnemius flap applied. L: Length of tumor tissue in bone (MRI measurement), WFP: The width of the tumor tissue in the frontal plane (MRI measurement), WSP: The width of the tumor tissue in the sagittal plane (MRI measurement). aIndependent Sample t test, bMann-Whitney U test. |
|||||||
| Demographics | Group 1 (n:16) | Group 2 (n:17) | p |
| Age (years) | 21 [15.0–28.5] | 22 [14.5–29.5] | 0.763b |
| Sex | |||
| Male | 9 (56.3%) | 7 (41.2%) | 0.387c |
| Female | 7 (43.8%) | 10 (58.8%) | |
| Histopathologic diagnosis | |||
| OS | 7 (43.8%) | 7 (41.2%) | 0.958c |
| EWS | 4 (25%) | 3 (17.6%) | |
| APS | 2 (12.5%) | 2 (11.8%) | |
| SS | 2 (12.5%) | 3 (17.6%) | |
| MGCBT | 1 (6.3%) | 2 (11.8%) | |
| Chemotherapy | |||
| Yes | 13 (81.3%) | 15 (88.2%) | 0.656d |
| No | 3 (18.8%)* | 2 (11.8%)* | |
| Reoperation no | 2.13 ± 1.5 [1–5] | 2.12 ± 1.45 [1–3] | 0.958a |
| Follow-up (months) | 34.06 ± 13.21 [17–56] | 30.41 ± 12.06 [15–58] | 0.413a |
| Infection | |||
| Yes | 4 (25%) | 5 (29.4%) | 1.00c |
| No | 12 (75%) | 12 (70.6%) | |
| EWS: Ewing sarcoma; MGCBT: malignant giant cell bone tumor; SS: synovial sarcoma. aIndependent Sample t test (Mean ± Standard Deviation [Minimum-Maximum]), bMann-Whitney U test (Median [Interquartiles], cChi-Square test, dFisher Exact test. *Number of patients who received radiotherapy. |
|||
However, the location of the tumor’s extra-compartmental aspect played a pivotal role in group allocation. Although there was no statistically significant difference in infection rates between the two groups, ROC curve analysis revealed that variables such as preoperative tumor size, resection size, and patient age were significant predictors of infection occurrence compared to patients who remained infection free. ROC analysis revealed statistically significant and high discrimination values for three parameters in comparing with and without infections. These parameters were tumor volume (p < 0.001), bone defect size (p < 0.001), and patient age (p = 0.054). While tumor volume and bone defect size provide high accuracy and reliability in detecting infection, the age parameter shows a lower performance (Table 4).
Pairwise comparison of ROC curves was performed to determine the differences between the performances of different parameters in detecting postoperative prosthesis infection. The fact that the difference between tumor volume and bone defect is not statistically significant indicates that both parameters are similarly effective in detecting infection (p = 0.126). However, the difference between tumor volume and age parameters is at the significance level, indicating that tumor volume may be a stronger marker (p = 0.094) (Table 5). These three parameters need to be carefully evaluated in clinical applications. It is especially difficult to say that advanced age alone is a risk factor for infection. Using multiple parameters together can contribute to obtaining more accurate and reliable results.
Discussion
Chimeric flaps have been developed to provide well-vascularized soft tissue support for the proximal tibia region to minimize surgical site infection rates [14]. While innovations in implant technologies have been impressive, they alone have not been fully sufficient in preventing surgical site infections. Alongside the advantages provided by multidisciplinary approaches, significant advancements have been made in regaining soft tissue coverage in the defect area and around the implant site through additional reconstructive surgical techniques. The most popular among these reconstructive techniques involves soft tissue reconstruction. This preference stems from the belief that one of the reasons for the high infection rates in this area is the relative deficiency of well-vascularized soft tissue coverage [15]. As widely known, gastrocnemius flaps are one of the most preferred and popular techniques among surgeons for regaining soft tissue coverage in this surgical field. The impact of this versatile technique on infection rates is based on a clinical study conducted by Grimier et al. in the 1990s. In their study, the authors reported a significant decrease in infection rates from 36 to 12% with the use of medial gastrocnemius flaps in 151 patients. There are also other encouraging studies in the literature, indicating that such additional surgical interventions effectively reduce infection rates in practice [16, 17].
Theoretically, while the idea that a well-vascularized soft tissue support could reduce surgical site infections seems logical, there are opposing views in the literature. In the recent comprehensive study by Andreas and colleagues, it was reported that the infection rate was 13.79% in patients without gastrocnemius flap application, whereas it was 11.32% in patients with gastrocnemius flap application. However, most of the mentioned studies are of a general nature. Specific studies focusing on the tibial surgical site in question and those combined with megaprostheses are extremely limited. Therefore, unfortunately, we could not find a large-scale study investigating the impact of gastrocnemius flaps on infection rates for tibial megaprostheses.
Due to the identified gaps in the existing literature and the reasons deliberated upon, our investigation focused exclusively on assessing infection rates and etiological parameters in patients subjected to tibial proximal megaprosthesis surgery at our institution. Our findings unveiled an average surgical site infection rate of 27.2% across the entire patient cohort. Upon subgroup analysis, the infection rate was delineated as 25% in Group 1 (employing gastrocnemius flap) and 29.4% in Group 2 (absence of gastrocnemius flap). Importantly, statistical scrutiny failed to disclose any significant disparity in infection rates between the aforementioned groups (p = 0.885). Furthermore, our analysis detected no statistically significant variances in demographic attributes, including age, gender distribution (p = 0.763), necessity for reoperation (p = 0.958), preoperative magnetic resonance imaging (MRI)-derived tumor dimensions, and post-resection defects (p = 0.440) between the two groups (Table 1). These observations hint at the presence of a potentially intricate scenario, warranting the imperative need for further comprehensive investigations in this domain.
Our study found that tumor volume and bone defect size were statistically significant factors influencing the risk of infection. These findings highlight the potential impact of larger tumor volumes and defect sizes on surgical site infections. Larger tumors may result in prolonged surgical times, increased dead space, and heightened risk of material contamination. These observations are consistent with previous literature, which supports the association between extensive surgeries and a higher risk of postoperative complications.
As a secondary objective of our study, we aimed to thoroughly examine clinical parameters that could potentially lead to surgical site infection independent of the gastrocnemius flap. Based on our clinical observations, we hypothesized that parameters such as the volumetric size of the tumor, the size of tumor tissue within the bone, the size of the megaprostheses, the histological diagnosis of the tumor, and the patient’s age could be influential. Upon statistical evaluation of these parameters, no significant difference was found in surgical site infection rates between the two groups. However, interestingly, ROC curve analysis revealed some findings parallel to our clinical observations. According to this analysis, it was determined that in patients who developed surgical site infection, the risk of infection increased proportionally with a larger preoperative tumor volume and a larger defect size after resection compared to those who did not develop infection. Actually, this result is not surprising for surgeons practicing in this field intensively, as various complications are expected following extensive surgeries and large defects. Additionally, the age of the patient and the histopathological diagnosis of the tumor were identified as important variables in the occurrence of infection, indicating the need for further in-depth analysis of this issue (Tables 3 and 4).
Every study has its strengths and weaknesses, and ours is no exception. In our study, some limitations were identified. First, the limited number of patients was attributable to the nature of the disease and its anatomical location, making it challenging to extensively generalize our findings. Nonetheless, we believe our study contributes to the literature by focusing on surgical site infections in patients undergoing megaprosthesis, offering insights for future research endeavors. Second, the retrospective nature of our study posed another limitation. However, we contend that the comprehensive documentation of patient data and the single-center design helped mitigate this constraint by facilitating easy and effective access to data. Third, the heterogeneity of tumors in terms of histopathologic diagnosis and stage among the included patients presented another challenge. Nevertheless, no statistically significant differences were observed between the two groups in terms of histopathologic diagnosis, staging, or adjuvant treatment, suggesting a low likelihood of our results being influenced by this variability. It remains unclear whether the observed infections resulted from material contamination or complications related to gastrocnemius flap failure, such as wound dehiscence. Addressing this question requires further investigation and more detailed data. This limitation highlights the need for future studies to specifically analyze the relationship between flap failure and infection development. Another important point to mention is this. In patients with poor soft tissue support parallel to the tumoral tissue size, gastrocnemius muscle flap was used. In other words, randomization was not performed because our study is retrospective. It has been reported that chimeric repairs performed by adding medial sural artery perforator skin flap to gastrocnemius muscle in knee region soft tissue reconstruction offer much higher safety probability in terms of reducing infection compared to patients who only underwent muscle transfer [18]. However, since no large tissue defect occurred after tumor resection in any patient in our study, gastrocnemius musculocutaneous with propeller skin flap repair was required.
Conclusion
In conclusion, the routine use of gastrocnemius flaps to repair post-surgical defects resulting from proximal tibial tumors does not lead to a significant reduction in surgical site infection rates. The application of gastrocnemius flaps carries inherent risks and potential complications. Their widespread adoption may present additional challenges for patients undergoing these procedures. Therefore, it is essential to establish clear-cut indications for the use of gastrocnemius flaps in such cases and to ensure careful patient selection. Surgeons should reconsider the notion that the primary objective of gastrocnemius flap transfer is solely to reduce infection rates. Our subgroup analysis and clinical observations underscore the importance of considering tumor size and the resulting defect size in bone and soft tissue post-resection as critical parameters in the development of surgical site infections.
References
[1] Gosheger G, Gebert C, Ahrens H, et al. Endoprosthetic reconstruction in 250 patients with sarcoma. Clin Orthop Relat Res. 2006; 450: 164–171. https://doi.org/10.1097/01.blo.0000223978.36831.39
[2] Grimer RJ, Belthur M, Chandrasekar C, et al. Two-stage revision for infected endoprostheses used in tumor surgery. Clin Orthop Relat Res. 2002; 395: 193–203. https://doi.org/10.1097/00003086-200202000-00022
[3] Hardes J, Gebert C, Schwappach A, et al. Characteristics and outcome of infections associated with tumor endoprostheses. Arch Orthop Trauma Surg. 2006; 126(5): 289–296. https://doi.org/10.1007/s00402-005-0009-1
[4] Zeegen EN, Aponte-Tinao LA, Hornicek FJ, et al. Survivorship analysis of 141 modular metallic endoprostheses at early followup. Clin Orthop Relat Res. 2004; 420: 239–250. https://doi.org/10.1097/00003086-200403000-00034
[5] Bus MP, van de Sande MA, Fiocco M, et al. What are the long-term results of MUTARS® modular endoprostheses for reconstruction of tumor resection of the distal femur and proximal Tibia? Clin Orthop Relat Res 2017; 475(3): 708–718. https://doi.org/10.1007/s11999-015-4644-8
[6] Donati D, Colangeli M, Colangeli S, et al. Allograft-prosthetic composite in the proximal tibia after bone tumor resection. Clin Orthop Relat Res. 2008; 466(2): 459–465. https://doi.org/10.1007/s11999-007-0055-9
[7] Gottsauner-Wolf F, Kotz R, Knahr K, et al. Rotationplasty for limb salvage in the treatment of malignant tumors at the knee. A follow-up study of seventy patients. J Bone Joint Surg Am. 1991; 73(9): 1365–1375. https://doi.org/10.2106/00004623-199173090-00012
[8] Henderson ER, Groundland JS, Pala E, et al. Failure mode classification for tumor endoprostheses: retrospective review of five institutions and a literature review. J Bone Joint Surg Am. 2011; 93(5): 418–429. https://doi.org/10.2106/JBJS.J.00834
[9] Henderson ER, O’Connor MI, Ruggieri P, et al. Classification of failure of limb salvage after reconstructive surgery for bone tumours: a modified system including biological and expandable reconstructions. Bone Joint J. 2014; 96-B(11): 1436–1440. https://doi.org/10.1302/0301-620X.96B11.34747
[10] Grimer RJ, Carter SR, Tillman RM, et al. Endoprosthetic replacement of the proximal tibia. J Bone Joint Surg Br. 1999; 81(3): 488–494. https://doi.org/10.1302/0301-620X.81B3.0810488
[11] Mavrogenis AF, Pala E, Angelini A, et al. Proximal tibial resections and reconstructions: clinical outcome of 225 patients. J Surg Oncol. 2013; 107(4): 335–342. https://doi.org/10.1002/jso.23216
[12] Bibbo C. The gastrocnemius flap for lower extremity reconstruction. Clin Podiatr Med Surg. 2020; 37(4): 609–619. https://doi.org/10.1016/j.cpm.2020.07.002
[13] DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988; 44(3): 837–845. https://doi.org/10.2307/2531595
[14] Sapino G, Osinga R, Maruccia M, et al. Role of the gastrocnemius musculocutaneous with a propeller style skin flap in knee region reconstruction: Indications and pitfalls. Arch Plast Surg 2023; 50(6): 593–600. https://doi.org/10.1055/s-0043-1768644
[15] Wittig JC, Villalobos CE, Hayden BL, et al. Osteosarcoma of the proximal tibia: limb-sparing resection and reconstruction with a modular segmental proximal tibia tumor prosthesis. Ann Surg Oncol. 2010; 17(11): 3021. https://doi.org/10.1245/s10434-010-1180-3
[16] Chim H, Tan BK, Tan MH, et al. Optimizing the use of local muscle flaps for knee megaprosthesis coverage. Ann Plast Surg. 2007; 59(4): 398–403. https://doi.org/10.1097/01.sap.0000258955.27987.17
[17] Zhang Y, Yang Z, Li X, et al. Custom prosthetic reconstruction for proximal tibial osteosarcoma with proximal tibiofibular joint involved. Surg Oncol. 2008; 17(2): 87–95. https://doi.org/10.1016/j.suronc.2007.11.003
[18] Sapino G, Guiller D, Osinga R, et al. Muscle-only versus chimeric musculocutaneous gastrocnemius pedicled flap in complex orthoplastic reconstructions of the knee region: a retrospective study. J Plast Reconstr Aesthet Surg. 2023; 77: 298–308. https://doi.org/10.1016/j.bjps.2022.12.006