REVIEW ARTICLE
Application of indocyanine green lymphography in the diagnosis and treatment of secondary upper extremity lymphedema: a systematic review
Youlei Qian, MDa*, Zixuan Yaoa*, Chao Wang, MDb, Chao Dong, MDc, Song Xia, MDa, Yuguang Sun, MDa, Wenbin Shen, MDa and Jianfeng Xin, MDa
aDepartment of Lymphatic Surgery, Beijing Shijitan Hospital, Capital Medical University, Beijing, PR China; bLaboratory of Surgical Oncology, Peking University People’s Hospital, Beijing, PR China; cDepartment of Ultrasound, Sanfine International Hospital, Beijing, PR China
ABSTRACT
Background: Lymphedema is a chronic progressive disease that impairs patients’ physical and psychological health. This study aimed to conduct a systematic review of the application of indocyanine green (ICG) lymphography for the diagnosis and treatment of secondary upper extremity lymphedema.
Methods: We searched PubMed for studies on ICG lymphography for secondary upper extremity lymphedema that were published until April 2024. The quality of included studies was assessed according to the Joanna Briggs Institute Review’s Manual. Qualitative synthesis using only descriptive statistics was performed.
Results: Of the 523 articles screened, 32 met the eligibility criteria. Most of the studies were observational (4 cohort studies and 28 case series). For this review, 1,869 patients with secondary lymphedema and 112 volunteers were identified. ICG lymphography for diagnostic imaging of secondary lymphedema was reported to have a sensitivity of 89.5% and a specificity of 85.7% and was particularly useful for the diagnosis of early lymphedema. A severity staging system based on ICG lymphography images for secondary lymphedema was also reported. In the lymphaticovenous anastomosis (LVA) surgery, ICG lymphography was helpful in detecting functional lymphatic vessels preoperatively and in localizing lymphatic vessels and assessing LVA patency intraoperatively, thereby facilitating smaller skin incision and shorter operating time.
Conclusions: ICG lymphography has a great value in the diagnosis and treatment of secondary upper extremity lymphedema.
KEYWORDS: ICG lymphography; near-infrared fluorescence imaging; secondary lymphedema; upper extremity lymphedema; lymphaticovenous anastomosis
Citation: Journal of Plastic Surgery and Hand Surgery 2025; 60: 171–179. DOI: https://doi.org/10.2340/jphs.v60.44582.
Copyright: © 2025 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 23 February 2025; Accepted: 26 July 2025; Published: 25 August 2025
CONTACT: Jianfeng Xin, MD xinjianfeng@bjsjth.cn Department of Lymphatic Surgery, Beijing Shijitan Hospital, Capital Medical University, Beijing 100038, PR China; Wenbin Shen, MD Department of Lymphatic Surgery, Beijing Shijitan Hospital, Capital Medical University, Beijing 100038, PR China
*These authors contributed equally to this work and should be considered co-first authors.
Competing interests and funding: The authors declare that they have no conflicts of interest. This work was supported by Beijing Municipal Administration of Hospitals Incubating Program, Code: PX2022028.
Introduction
Lymphedema is a chronic progressive disease resulting primarily from congenital lymphatic anomaly and secondarily from injury to the lymphatic system [1]. Lymphedema causes disfigurement and decreased mobility, leading to physical and psychological morbidity [2]. More than 20% of the patients develop arm lymphedema 2 years after breast cancer surgery [3]. Lymphedema has become one of the most significant survivorship issues after cancer treatment, yet no curative treatment for lymphedema has been established. Early detection of and intervention for lymphedema is crucial because it could significantly improve treatment outcomes [4]. However, lymphoscintigraphy, which is the current golden standard for the diagnosis of lymphatic transport dysfunction, is inappropriate for lymphedema screening because of the radiological hazard of its contrast agent. Thus, diagnostic modality with higher sensitivity is needed for the early diagnosis of lymphedema.
Indocyanine green (ICG) is a low toxicity fluorescent dye that has been used to evaluate cardiac output, hepatic function, and flap perfusion. In 2007, near-infrared (NIR) fluorescence imaging with ICG was adapted for lymphatic mapping [5], which was subsequently known as ICG lymphography; it facilitates real-time, low-invasive examination of the lymphatic system without radiation exposure. Furthermore, Yamamoto et al. classified ICG lymphography findings as a linear pattern or three dermal backflow (DB) patterns, splash, stardust, and diffuse patterns, correlating with the progression of lymphedema severity [6]. ICG lymphography showed better sensitivity and specificity than lymphoscintigraphy in the diagnostic imaging of lymphedema, especially for early-stage patients [7]. Meanwhile, preoperative lymphatic mapping by ICG lymphography in lymphaticovenous anastomosis (LVA) surgery was first introduced by Ogata et al., showing its potential application in the treatment of lymphedema [8]. This review aimed to examine the literature on the role of ICG lymphography for the diagnosis and management of lymphedema. The goal is to provide a comprehensive assessment of the published literature (1) to offer clinicians information on how to better apply ICG lymphography in the diagnosis and treatment of lymphedema and (2) to provide directions for future research.
Methods
This study was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [9].
Search strategy
We searched PubMed for relevant studies published until March 2024, using the search terms (‘Indocyanine green’ OR ‘Near-infrared fluorescence imaging’) AND ‘lymphedema’. Only English articles were reviewed.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) patients with secondary lymphedema of upper extremity; (2) studies with in vivo data acquisition on human tissues; (3) original studies regarding the use of ICG lymphography for the diagnosis and treatment of lymphedema; and (4) studies whose results included at least one outcome of interest.
The following studies were excluded: (1) those with fewer than five patients and (2) studies from the same institution with overlapping patients (in such cases, we selected the study that was published later).
Outcomes of interest
Studies in which ICG lymphography was used for the diagnosis and staging of secondary upper extremity lymphedema or ICG lymphography was used as part of secondary upper extremity lymphedema treatment were of interest in this review.
Data extraction
The eight authors independently gather and extracted the following data: first author, publication year, study design, number of patients, location of lymphedema, clinical stage of lymphedema, imaging protocol, and information on optical signal analysis. After the first author summarized them, other authors discussed together and reached a consensus. The final results were also approved by all authors.
Assessment of study quality
We used the Joanna Briggs Institute (JBI) Review’s Manual [10] to assess the quality of the included qualitative studies. The manual has 10 items, and each item was judged ‘Yes’, ‘No’, ‘Unclear’, or ‘Not applicable’.
Statistical analysis
Only descriptive statistics were performed for qualitative synthesis. No assessment of heterogeneity, publication bias, or any other statistical data was planned.
Results
Study selection and characteristics
For this systematic review, 523 articles were screened and 32 met the eligibility criteria. Thus, a total of 32 studies, with 1,869 secondary lymphedema and 112 volunteers, were included in this review (Figure 1). 13% of the included clinical studies were cohort studies (4/32), and the rest were case series (28/32). The quality of every included study was assessed (Figure 2).
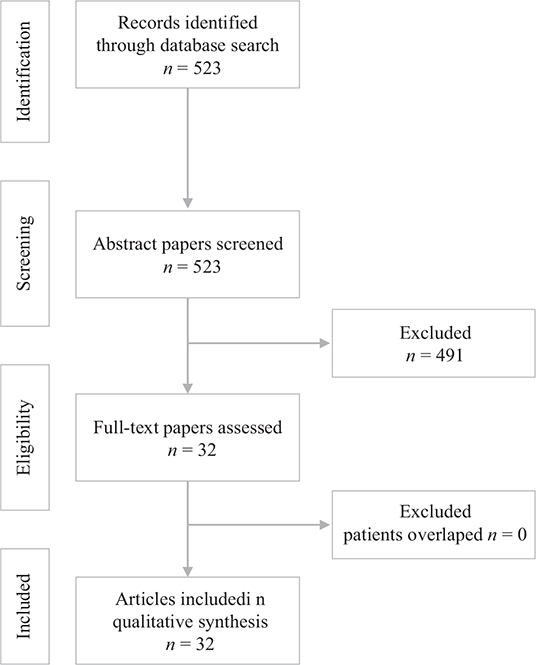
Figure 1. Flow chart of the study selection.
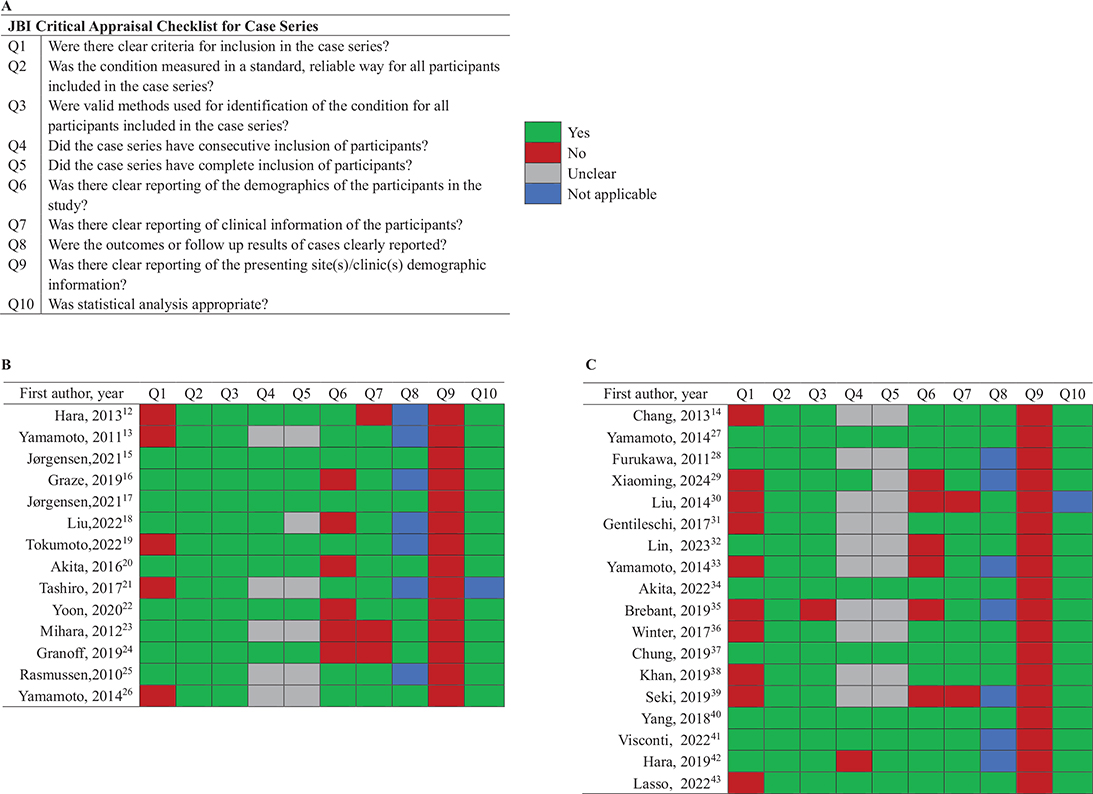
Figure 2. Assessment of study quality. (A) JBI Review Manual’s critical appraisal checklist for case series. (B) Quality assessment of studies regarding lymphedema diagnosis and staging. (C) Quality assessment of studies regarding ICG-L-guided lymphatic microsurgery.
JBI: Joanna Briggs Institute; ICG-LG: indocyanine green lymphography.
Based on the literature, ICG lymphography was evaluated for two clinical applications. First, ICG lymphography was used to evaluate the function of the lymphatic system. 2 cohort studies and 12 case series were identified (Table 1) [11–24]. Second, 2 cohort studies and 16 case series reported on the use of ICG lymphography for guiding lymphatic microsurgery (Table 2) [25–42].
| First author, Year | Study design | No. of cases | Sites | Clinical stage | Protocol | Results | ||
| ICG administration | Imaging timing (after ICG injection) | Equipment | ||||||
| Hara, 2013 [11] | Case series | 29P* | 23LE 2UE |
ISL0-3 | II of 0.2 mL 0.5% ICG at the first interdigit of foot or at the second interdigit of the hand | 15–22 h | PDE | ICG-LG findings were related to the condition of collecting lymph vessels. |
| Yamamoto, 2011 [12] | Case series | 20P | UE | Campisi1-4 | SI of 0.1 mL of 0.25% ICG at the second interdigit of the hand and the ulnar border of the palmaris longus tendon at the level of the wrist | Immediately | PDE | Introduced DB staging of UE-SLE |
| Jørgensen, 2021 [13] | Case series | 237P | 237UE | ISL0-3 | SI and II of 0.1 mL of 0.25% ICG at the first and third webspace and on the ulnar border of the palmaris longus tendon at the level of the wrist | Immediately, 10 min and 1 h | HE | Reveal the poor correlation between the ISL stage and the MDA and ADB stages. |
| Graze, 2019 [14] | Case series | 212P | 130UE 82LE |
UD | II of 0.1–0.2 mL ICG at each webspace and at the volar radial and ulnar wrist of the hand or at each webspace and just inferior to the medial and lateral malleoli | Soon | PDE | The clinical ISL stage does not correlate well with the ICG stage in patients undergoing physiologic lymphedema surgery. |
| Jørgensen, 2021 [15] | Case series | 200P | 200UE | ISL0-3 | Injection of 0.1 mL of 0.25% ICG at the ulnar border of the palmaris longus tendon at the wrist’s level | Immediately | HE | The superiority of ICG-L at modeling the amount of excess volume, fat mass, and lean mass compared with ISL staging. |
| Liu, 2022 [16] | Cohort study | 91P 88V | 97UE | UD | SI of 0.2 mL ICG at the second web space of the dorsal aspect of the hand | Immediately and every 30 min | PDE | ICG-positive patients have a higher risk of lymphedema. |
| Tokumoto, 2022 [17] | Case series | 155P | 155UE | UD | SI of 0.3 mL ICG at the first web space over the dorsum of the affected hand. | 1 h | PDE | Propose the relationship between circumference and the severity of ICG finding. |
| Akita, 2016 [18] | Case series | 196P | UE | UD | SI of 0.3 mL of ICG at the first interdigit of the hand | 1 h | PDE | Lymphatic function disorder could be detected before volume changes by ICG-LG. |
| Tashiro, 2017 [19] | Case series | 29P | UE | ISL1–3 | II of 0.2 mL of 0.5% ICG at the second interdigit of the hand and the ulnar border of the palmaris longus tendon at the level of the wrist | 15–24 h | PDE | Variations in the UE lymphatic system were easily visualized using ICG-LG. |
| Yoon, 2020 [20] | Case series | 47P | 47UE | UD | SI of 0.2 mL of 0.25% ICG at the bilateral upper extremities at the first and third web space of the hand. | Every hour | UD | The confirm ADB stage is correlated with lymphoscintigraphy severity stage positively. |
| Mihara, 2012 [21] | Case series | 21P | UE | ISL1 | SI of 0.2 mL of 0.5% ICG at the second interdigit of the hand | Immediately | PDE | ICG-LG was superior to lymphoscintigraphy for the diagnostic imaging of early lymphedema of the UE. |
| Granoff, 2019 [22] | Case series | 17P | UE | UD | II of 0.1 mL of 0.625% ICG at the first and fourth web spaces of the hand, volar forearm, and lateral upper arm of the ipsilateral extremity | Immediately | PDE | Described an approach to quantify lymphatic contractility during ICG-LG |
| Rasmussen, 2010 [23] | Cohort study | 20P 24V |
10UE 10LE | UD | II of 0.1 mL of 0.25% ICG, varied injection sites | Immediately | UD | Described changes in lymphatic architecture and dynamic transport of LE limbs in ICG-LG |
| Yamamoto, 2014 [24] | Case series | 15P | UE | ISL0–3 | SI of 0.2 mL of 0.5% ICG at the second interdigit of the hand | Immediately and 2 h | PDE | Dynamic ICG-LG could evaluate both lymph pump function and circulation. |
| No: number; P: patients; V: volunteers; P*: including primary lymphedema patients; LE: lower extremities; UE: upper extremities; G: genitalia; SLE: secondary lymphedema; GL: genital lymphedema; ISL: International Society of Lymphology; SI: subcutaneous injection; II: intracutaneous injection; ICG-LG: ICG lymphography; UD: undefined; DB: dermal backflow; LEC: Latency-Edema-Compression; PDE: photodynamic eye infrared camera system; HE: HyperEye medical system. | ||||||||
| First author,Year | Study design | No. of cases | Sites | Clinical stage | Protocol | Result | ||
| ICG administration | Imaging timing(after ICG injection) | Equipment | Application | |||||
| Chang, 2013 [25] | Case series | 100P | 89UE 11LE | UD | II of 0.01–0.02 mL ICG at the second interdigit of the hand | Immediately | PDE | Pre: detecting functional lymphatic vessels |
| Yamamoto, 2014 [26] | Case series | 8P | 5LE 3UE | UD | SI of 0.2 mL of 0.25% ICG at the second web space of the foot or 0.1 mL of 0.25% ICG at the second web space of the hand | 1 day | PDE and OPMI Pentero Infrared 800 | Pre: detecting functional lymphatic vessels Intra: localization of lymphatic vessels |
| Furukawa, 2011 [27] | Case series | 9P | UE | UD | II of 0.2 mL ICG at the second interdigit of the hand | Immediately | PDE | Pre: detecting functional lymphatic vessels |
| Xiaoming, 2024 [28] | Case series | 29P | 29UE | UD | Injection of 0.3–0.5 mL ICG at the interdigital spaces of the affected limb | Immediately | Venous ultrasound and Pentero 800 | Pre: detecting low pressure veins |
| Liu, 2014 [29] | Case series | 20P | 11UE 9LE | ISL1–2 | SI of 0.2 mL of 0.5% ICG at the second and third web spaces of the hand and the medial and lateral sides of the volar surface of the wrist, or at the first and third web spaces of the foot and the medial and lateral sides of the Achilles tendon | 1 h | Leica FL800 | Pre: lymphatic mapping and staging Intra: localization of lymphatic vessels and confirmation of the patency of the LVA |
| Gentileschi, 2017 [30] | Case series | 16P | UE | ISL2 | II of 0.2 mL ICG at the second interdigit of the hand and the ulnar border of the palmaris longus tendon at the level of the wrist | Immediately | PDE | Pre: lymphatic mapping of DB UE by mirroring of the healthy limb with ICG-LG |
| Lin, 2023 [31] | Cohort study | 6P | 2UE 4LE | UD | SI or II of 0.1 mL ICG at the first two finger digital spaces or toe web spaces | 30 min | Moller 3–1000 | Intra: distinguish ICG-enhanced vessels under the microscope |
| Yamamoto, 2014 [32] | Case series | 11P | 3UE 8LE | UD | SI of 0.1 mL of 0.25% ICG at the second web space of the hand and the ulnar border of the palmaris longus tendon at the level of the wrist, or 0.2 mL ICG at the first web space of the foot and the lateral border of the Achilles tendon | UD | PDE and OME-900 | Pre: detecting functional lymphatic vessels Intra: localization of lymphatic vessels and confirmation of the patency of the LVA |
| Akita, 2022 [33] | Case series | 57P | 13UE 44LE | ISL0–2b | SI of 0.2 mL of 0.25% ICG at five sites on the hand or foot and each anastomotic site after the anastomosis was completed | Within 3 h | PDE | Intra: confirm the patency of anastomosis |
| Brebant, 2019 [34] | Case series | 32P | 26UE 5LE | ISL2 | SI of 0.1 mL of 0.25% ICG at the second and third interdigital spaces of the hand | 1 day | Leica M530 OHX with glow 89 technology ULT530 | Intra: localization of lymphatic vessels and confirmation of the patency of the LVA |
| Winters, 2017 [35] | Case series | 29P | UE | Campisi1b–2a | SI of 0.25% ICG at the second web space of the hand | UD | PDE | Pre: detecting functional lymphatic vessels Intra: confirmation of the patency of the LVA |
| Chung, 2019 [36] | Case series | 18P | 8UE 10LE |
Campisi2–4 | II of 0.3–0.5 mL of 0.8% ICG at the first and second web spaces of the fingers/toes, and an additional II of 0.3–0.5 mL ICG at a location 5–6 cm distal from the possible incision sites | UD | Pantero 900 | Intra: localization of lymphatic vessels and confirmation of the patency of the LVA |
| Khan, 2019 [37] | Case series | 27P | UE | UD | II or SI of 0.1–0.2 mL of 0.5% ICG at the second web space of the hand and the ulnar border of the hand | Immediately | PDE | Pre: detecting functional lymphatic vessels Intra: confirmation of the patency of the LVA |
| Seki, 2019 [38] | Case series | 10P | UE | ISL2 | II of 0.1 mL of 0.25% ICG at the second web space of the hand, at the anterior border of the styloid process of the radius, and at the anterior border of the styloid process of the ulna | 2 h | LIGHTVION | Intra: confirmation of lymphatic vessels |
| Yang, 2018 [39] | Case series | 58P* | 8UE 48LE | ISL2–3 | UD | UD | Pantero 900 | Intra: confirmation of lymphatic collecting vessels |
| Visconti, 2022 [40] | Case series | 76P | 47UE 29LE | ISL2b–3 | UD | UD | PDE and UHFUS | Pre: detecting functioning lymphatic vessels undetectable by lymphoscintigraphy and ICG-L |
| Hara, 2019 [41] | Cohort study | 60P* 49C |
10UE 186LE | ISL1–3 | SI of 0.1 mL of 0.5% ICG at the second web space of the hand or at the first web space of the foot. In the multi-injection group, additional ICG was injected in the medial or lateral ankle or knee for LE or in the wrist or elbow for UE. | Immediately | PDE | Pre: detecting functional lymphatic vessels |
| Lasso, 2022 [42] | Case series | 20P | 13UE LE | ISL2 | II of 0.1 mL ICG at the first and fourth web spaces | 15 min | PDE | Intra: localization of lymphatic vessels with ICG-guidance on liposuction |
| No: number; P: patients; C: controls; P*: including primary lymphedema patients; LE: lower extremities; UE: upper extremities; SLE: secondary lymphedema; ISL: International Society of Lymphology; SI: subcutaneous injection; II: intracutaneous injection; ICG-LG: ICG lymphography; UD: undefined; DB: dermal backflow; PDE: photodynamic eye infrared camera system; UHFUS: ultra-high-frequency ultrasound; LVA: lymphovenous anastomosis; Pre: Preoperatively; Intra: Intraoperatively. | ||||||||
ICG lymphography for lymphedema diagnosis and staging
Hara et al. reported that the severity of DB patterns has a strong correlation with the condition of regional collecting lymph vessels in the upper extremity, in the linear region, normal lymph vessels account for about 35%, while in the more serious regions, it is only about 10%. On the contrary, the most serious sclerosis-type lymph vessels, which are not found in the linear region, account for 30 and 50% in stardust and diffuse regions [11]. By combining DB patterns with the anatomical region, Yamamoto et al. established the DB staging system of secondary lymphedema of the arm. In this staging system, DB patterns were more proximal in earlier stages and were worse and progressively spread distally in more severe stages, and the DB stage is linearly correlated with clinical stage [12]. Chang et al. established a simplified staging system, i.e. M. D. Anderson lymphedema classification, which was mainly based on the size of DB area [25]. Jørgensen et al. found that the M. D. Anderson (MDA) scale and the Arm Dermal Backflow (ADB) scale were in near perfect inter- and intrarater agreement. Meanwhile, the correlation between the International Society of Lymphology (ISL) stage and the MDA and ADB scales was weak, which indicated clinical stage, and the ICG lymphography stage was in a quite low agreement [13]. An analysis of 212 cases by Garza et al. also revealed a weak correlation between the ISL stage and the M. D. Anderson stage [14]. Moreover, Jørgensen et al. reported that each ICG lymphography staging’s increase leads to percentage points increase in volume, fat mass, and lean mass, when the ascending ISL stages lead no significant difference in the fat and lean mass, indicating that ICG lymphography was more adequate for assessing lymphatic function than clinical staging [15].
ICG lymphography could detect lymphatic function disorder even before edema becomes clinically evident. According to the result of ICG lymphography, a cohort study divided 88 postoperative breast cancer patients without lymphedema into ICG-positive (n = 47) and ICG-negative (n = 41) groups, and Liu et al. detected that the ICG-positive group has a higher incidence of lymphedema [16]. By observing 155 patients with unilateral breast cancer-related lymphedema, Tokumoto et al. also indicated that circumference change has significant correlation with ICG lymphography staging at four parts on upper limb (around the wrist, forearm, elbow, and brachium) [17]. Akita et al. detected that 21 of 35 patients with lymphatic disorder do not have significant limb volume change, which means the DB pattern could be detected before volume changes. Akita et al. also reported that early intervention with conservative treatments resulted in lymphatic function improvement in just under one-third of the cases [18]. Moreover, variations in the lymphatic system such as superficial lymphatic collateral ways were easily visualized using ICG lymphography [19].
Ja et al. had confirmed that the ADB stage is correlated with the lymphoscintigraphy severity stage positively, when the agreement between them is low [20]. Go a step further, Mihara et al. reported that ICG lymphography is superior to lymphoscintigraphy for the diagnostic imaging of secondary lymphedema, the sensitivity and specificity of ICG lymphography were both 1, whereas those of lymphoscintigraphy were 0.62 and 1, respectively [21].
Lymphatic function could be quantitatively measured by real-time dynamic ICG lymphography. Granoff et al. described an approach to quantify lymphatic contractility using ICG lymphography [22]. Moreover, Rusmussen et al. proposed two parameters to assess lymphatic function: apparent lymph propagation velocity and contractile frequency [23]. However, this protocol required visual identification of subsets of images showing movement of ‘packets’ of higher fluorescent intensity along the lymphatic vessels, which may not be possible in patients with advanced lymphedema. Studies showed that ICG velocity decreases as lymphedema severity progresses in upper extremity secondary lymphedema [24, 26].
The ICG lymphography protocols in the studies included in this review varied specifically in the ICG dose, injection sights, observation timing, and imaging system. Nevertheless, typically, ICG was administered intradermally or subcutaneously into the interdigital space, which is usually the second web space of the hand. Subsequently, an infrared camera system was used to collect ICG fluorescence and turn it into visible images in real-time. Thus, more than half of the studies recorded images in the plateau phase when no further change in images would be expected, which might take 12–24 h after ICG injection. Given the heterogeneity of ICG lymphography protocols, a comparison of the qualitative and quantitative results from different studies appears challenging.
ICG lymphography-guided lymphedema treatment
Skin incisions for LVA were generally designed on regions with linear pattern to shorten the incision length and the time required for detecting functional lymphatics. Nevertheless, to maximally preserve the distal linear lymphatic vessel, incisions could also be made on the area with vein and DB overlap [27]. Additionally, combined with ultrasonography, ICG lymphography can identify low pressure veins to shorten operative duration and lessen ineffective incisions [28].
Some studies suggested that LVA be avoided in patients with severe lymphedema, especially when a linear pattern could not be detected by ICG lymphography as the risk of failure to detect functional lymphatic vessel would be high [29]. However, Gentileschi et al. reported methods for lymphatic mapping in patients with unilateral advanced lymphedema, in which the lymphatic anatomy of the healthy limb was investigated using ICG lymphography and reported on the affected limb [30]. This study reported 100% success in detecting lymphatic vessels that are suitable for anastomosis, which shorten the operative time and the incisional length, indicating that LVA in advanced lymphedema is possible with the help of ICG lymphography.
Detecting translucent lymphatic vessels in subcutaneous tissue could be difficult. By equipping an NIR illumination system to a camera-integrated operating microscope, the ICG-enhanced lymphatic vessels were easily distinguished under the microscope [26, 31]. Yamamoto et al. managed to perform multi-site LVA within 2 h via small skin incisions (<1 cm) under the guidance of ICG lymphography [32]. Immediately after the LVA, intraoperative ICG lymphography could be used to determine shunt patency, and Akita et al. judged 267 LVAs and confirm the patency in 95.1% as ‘useful’ [33]. Meanwhile, Brebant et al. localized lymphatic vessels and confirmed the patency of the LVA under the ICG lymphography-guidance [34]. When ICG fluorescence from the lymphatic duct to the subdermal vein could not be observed, instant adjustment or re-anastomosis could be performed to elicit effective outcomes of LVA surgery with patent anastomosis [35–37]. An upgraded ICG lymphography system managed to separate the NIR fluorescence light of ICG from visible light of the operating microscope, which in turn enables the surgeon to identify lymphatic vessels easily by checking dual images from original and ICG fluorescent views [38].
During intraoperative ICG lymphography, ICG-negative but flow-positive lymphatic vessels within the incision site have always been observed. Should these lymphatic vessels be considered functional as well? In a retrospective study of Yang et al. including 56 patients, 258 flow-positive lymphatic vessels were detected, of which >20% was not ICG enhanced. LVAs were performed on 27 ICG-negative lymphatic vessels in seven patients, and all of them were satisfied with their improvements [39]. Similar observation was reported by Visconti et al. that functioning lymphatic vessels can be detected by ultra-high-frequency ultrasound when preoperative ICG lymphography showed no sign of lymphatic vessels [40]. Hara et al. conducted a prospective cohort study including a total of 109 patients and showed that ICG injection into multiple sites in the affected limbs resulted in the detection of a greater number of functional lymphatic vessels during LVA, thereby leading to a better surgical result [41]. Therefore, inappropriate ICG injection sites could be the reason for missing functional lymphatic vessels. Considering that unsatisfactory result after LVA exists, Lasso et al. suggested that liposuction with ICG guidance could be applicable on poor responders after LVAs to avoid inadvertent damage to lymphatic system [42].
Discussion
Early diagnosis of lymphedema is essential to achieve a favorable treatment outcome. Severity scaling systems aimed for early diagnosis based on lymphoscintigraphy have been reported. However, lymphoscintigraphy carries the risk of radiation exposure and is inappropriate for repeated test and lymphedema screening. Based on available evidence, ICG lymphography has better sensitivity and specificity for the early diagnosis of lymphedema compared with lymphoscintigraphy. Moreover, ICG lymphography is safe, simple, non-invasive, and relatively cheap, it also makes lymphatic function visualized by real-time dynamic equipment. Thus, several studies recommended that ICG lymphography be performed on a routine schedule after lymphadenectomy for malignancies to determine the earliest lymphatic disorder, especially in patients with a high risk of developing lymphedema. In a preliminary study, ICG lymphography detected lymphatic function disorder in 35 of 196 patients in the early postoperative period (<1 year) after breast cancer surgery, and with early conservative treatment, lymphatic function improved in nearly one-third of the cases. Randomized controlled cohort studies are needed to guide its application as a screening test for lymphedema. Besides, although side effects following ICG lymphography have not been reported, further studies on the effect of repeated administration of ICG to the lymphatic system are warranted to ensure safety.
A staging system that is adequately correlated with clinical severity is crucial for surgeons to make an optimal therapeutic decision. In the commonly used ISL staging system, stage 0 represents the condition when there is lymphatic injury but no swelling has shown.
In the DB staging system proposed by Yamamoto et al., ISL stage 0 was subdivided into DB stage I and DB stage II, which allows further stratification of the risk of lymphedema development in asymptomatic limbs of patients with secondary lymphedema. It was recommended that surgical interventions should be made only after DB stage II, when stardust or the diffused pattern was seen in ICG lymphography because the splash pattern in DB stage I represents a reversible lymphatic disorder.
Based on the size of DB area, the MDA and ADB scales have close correlation with clinical severity, when patients in a same ISL stage suffer different clinical severities. Otherwise, early diagnosis of lymphedema is essential to achieve a favorable treatment outcome. ICG lymphography can detect early lymphedema before clinical symptoms appear, which means we can predict if patients have high risk of lymphedema when they have no volume or circumference change. For BCRL patients, ICG lymphography could be used to access their DB patterns after accepting cancer-related treatment, which is correlated with the incidence of lymphedema. Further studies would be needed to clarify whether an early intervention based on DB staging is key for the prevention and management of lymphedema.
LVA has become a popular choice for refractory lymphedema because of its effectiveness and low invasiveness. Without a lymphatic mapping method, successful results of LVA would depend mainly on surgeon’s experience and technique. The use of ICG lymphography enables easy detection of functional lymphatic vessels, direct navigation for lymphatic vessel dissection, and immediate intraoperative verification of anastomotic patency; consequently, the incision is smaller, and the operating time is shorter. Even when considering the treatment of severe lymphedema, suitable lymphatic vessels could be detected with the guidance of ICG lymphography, so LVA becomes an appropriate choice.
Nevertheless, inappropriate ICG injection sites could lead to false-negative results during lymphography, thereby missing functional lymphatic vessels that are suitable for LVA. Based on Hara’s research, a greater number of functional lymphatic vessels were detected by adding ICG injection sites, which in turn resulted in better surgical outcomes. Thus, adjustments to ICG lymphography protocol should be made to meet the demand of intraoperative applications. Moreover, ICG-negative lymphatic vessels could be detected by ultrasound. Currently, it is still too early to detect functional lymphatic vessels fully depending on ICG lymphography, and careful evaluation of ICG-negative lymphatics is necessary for a better outcome.
Our systematic review is limited by the low-to-moderate quality of the studies. As most of the included studies were descriptive, data were insufficient for a meta-analysis. In the absence of a meta-analysis, the potential bias due to prolific authorship could not be evaluated. Finally, based on existing evidence, different injection sites might affect the images obtained during ICG lymphography. The ICG lymphography protocols from the included studies were hardly consistent, which in turn affected the comparison between studies and thus possibly influenced the conclusion.
In conclusion, based on limited evidence, we believe that ICG lymphography has a great value in the diagnostic imaging of lymphedema and is suitable particularly as a screening test for early lymphedema. ICG lymphography could be used in LVA surgery, specifically in preoperative lymphatic mapping, intraoperative navigation, and patency assessment. Nevertheless, high-quality clinical studies are needed to provide evidence for the clinical application of ICG lymphography.
Acknowledgments
None.
References
[1] Maclellan RA, Greene AK. Lymphedema. Semin Pediatr Surg. 2014;23(4):191–197. https://doi.org/10.1053/j.sempedsurg.2014.07.004
[2] Yüksel A, Gürbüz O, Velioğlu Y, et al. Management of lymphoedema. VASA. 2016;45(4):283–291. https://doi.org/10.1024/0301-1526/a000539
[3] DiSipio T, Rye S, Newman B, et al. Incidence of unilateral arm lymphoedema after breast cancer: a systematic review and meta-analysis. Lancet Oncol. 2013;14(6):500–515. https://doi.org/10.1016/S1470-2045(13)70076-7
[4] Shah C, Arthur DW, Wazer D, et al. The impact of early detection and intervention of breast cancer-related lymphedema: a systematic review. Cancer Med. 2016;5(6):1154–1162. https://doi.org/10.1002/cam4.691
[5] Unno N, Inuzuka K, Suzuki M, et al. Preliminary experience with a novel fluorescence lymphography using indocyanine green in patients with secondary lymphedema. J Vasc Surg. 2007;45(5):1016–1021. https://doi.org/10.1016/j.jvs.2007.01.023
[6] Yamamoto T, Matsuda N, Doi K, et al. The earliest finding of indocyanine green lymphography in asymptomatic limbs of lower extremity lymphedema patients secondary to cancer treatment: the modified dermal backflow stage and concept of subclinical lymphedema. Plastic Reconstr Surg. 2011;128(4):314e–321e. https://doi.org/10.1097/PRS.0b013e3182268da8
[7] Mihara M, Hara H, Narushima M, et al. Indocyanine green lymphography is superior to lymphoscintigraphy in imaging diagnosis of secondary lymphedema of the lower limbs. J Vasc Surg. 2013;1(2):194–201. https://doi.org/10.1016/j.jvsv.2012.07.011
[8] Ogata F, Narushima M, Mihara M, et al. Intraoperative lymphography using indocyanine green dye for near-infrared fluorescence labeling in lymphedema. Ann Plastic Surg. 2007;59(2):180–184. https://doi.org/10.1097/01.sap.0000253341.70866.54
[9] Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700. https://doi.org/10.1136/bmj.b2700
[10] Moola S, Munn Z, Tufanaru C, et al. Joanna Briggs Institute review’s mannul. The Joanna Briggs Institute, Adelaide, Australia; 2017.
[11] Hara H, Mihara M, Seki Y, et al. Comparison of indocyanine green lymphographic findings with the conditions of collecting lymphatic vessels of limbs in patients with lymphedema. Plastic Reconstr Surg. 2013;132(6):1612–1618. https://doi.org/10.1097/PRS.0b013e3182a97edc
[12] Yamamoto T, Yamamoto N, Doi K, et al. Indocyanine green–enhanced lymphography for upper extremity lymphedema: a novel severity staging system using dermal backflow patterns. Plastic Reconstr Surg. 2011;128(4):941–947. https://doi.org/10.1097/PRS.0b013e3182268cd9
[13] Jørgensen MG, Toyserkani NM, Hansen FCG, et al. Prospective validation of indocyanine green lymphangiography staging of breast cancer-related lymphedema. Cancers. 2021;13(7):1540. https://doi.org/10.3390/cancers13071540
[14] Garza RM, Ooi ASH, Falk J, et al. The relationship between clinical and indocyanine green staging in lymphedema. Lymphat Res Biol. 2019;17(3):329–333. https://doi.org/10.1089/lrb.2018.0014
[15] Jørgensen MG, Hermann AP, Madsen AR, et al. Indocyanine green lymphangiography is superior to clinical staging in breast cancer-related lymphedema. Sci Rep. 2021;11(1):21103. https://doi.org/10.1038/s41598-021-00396-2
[16] Liu M, Liu S, Zhao Q, et al. Using the indocyanine green (ICG) lymphography to screen breast cancer patients at high risk for lymphedema. Diagnostics. 2022;12(4):983. https://doi.org/10.3390/diagnostics12040983
[17] Tokumoto H, Akita S, Kubota Y, et al. Relationship between the circumference difference and findings of indocyanine green lymphography in breast cancer-related lymphedema. Ann Plastic Surg. 2022;88(1):114–117. https://doi.org/10.1097/SAP.0000000000002918
[18] Akita S, Nakamura R, Yamamoto N, et al. Early detection of lymphatic disorder and treatment for lymphedema following breast cancer. Plastic Reconstr Surg. 2016;138(2):192e–202e. https://doi.org/10.1097/PRS.0000000000002337
[19] Tashiro K, Yamashita S, Koshima I, et al. Visualization of accessory lymphatic pathways in secondary upper extremity lymphedema using indocyanine green lymphography. Ann Plastic Surg. 2017;79(4):393–396. https://doi.org/10.1097/SAP.0000000000001120
[20] Yoon JA, Shin MJ, Shin YB, et al. Correlation of ICG lymphography and lymphoscintigraphy severity stage in secondary upper limb lymphedema. J Plastic Reconstr Aesth Surg. 2020;73(11):1982–1988. https://doi.org/10.1016/j.bjps.2020.08.055
[21] Mihara M, Hara H, Araki J, et al. Indocyanine green (ICG) lymphography is superior to lymphoscintigraphy for diagnostic imaging of early lymphedema of the upper limbs. PLoS One. 2012;7(6):e38182. https://doi.org/10.1371/journal.pone.0038182
[22] Granoff MD, Johnson AR, Lee BT, et al. A novel approach to quantifying lymphatic contractility during indocyanine green lymphangiography. Plastic Reconstr Surg. 2019;144(5): 1197–1201. https://doi.org/10.1097/PRS.0000000000006176
[23] Rasmussen JC, Tan IC, Marshall MV, et al. Human lymphatic architecture and dynamic transport imaged using near-infrared fluorescence. Transl Oncol. 2010;3(6):362–372. https://doi.org/10.1593/tlo.10190
[24] Yamamoto T, Narushima M, Yoshimatsu H, et al. Dynamic indocyanine green (ICG) lymphography for breast cancer-related arm lymphedema. Ann Plastic Surg. 2014;73(6):706–709. https://doi.org/10.1097/SAP.0b013e318285875f
[25] Chang DW, Suami H, Skoracki R. A prospective analysis of 100 consecutive lymphovenous bypass cases for treatment of extremity lymphedema. Plastic Reconstr Surg. 2013;132(5):1305–1314. https://doi.org/10.1097/PRS.0b013e3182a4d626
[26] Yamamoto T, Yamamoto N, Numahata T, et al. Navigation lymphatic supermicrosurgery for the treatment of cancer-related peripheral lymphedema. Vasc Endovasc Surg. 2014;48(2):139–143. https://doi.org/10.1177/1538574413510979
[27] Furukawa H, Osawa M, Saito A, et al. Microsurgical lymphaticovenous implantation targeting dermal lymphatic backflow using indocyanine green fluorescence lymphography in the treatment of postmastectomy lymphedema. Plastic Reconstr Surg. 2011;127(5):1804–1811. https://doi.org/10.1097/PRS.0b013e31820cf2e2
[28] Xiaoming L, Wei T, Yi’nan J, et al. Application of combined preoperative indocyanine green lymphography and ultrasonography for low-pressure vein localization in secondary lymphedema surgery for breast cancer. Asian J Surg. 2024;47(1):289–295. https://doi.org/10.1016/j.asjsur.2023.08.121
[29] Liu HL, Pang SY, Chan YW. The use of a microscope with near-infrared imaging function in indocyanine green lymphography and lymphaticovenous anastomosis. J Plastic Reconstr Aesth Surg. 2014;67(2):231–236. https://doi.org/10.1016/j.bjps.2013.10.039
[30] Gentileschi S, Servillo M, Albanese R, et al. Lymphatic mapping of the upper limb with lymphedema before lymphatic supermicrosurgery by mirroring of the healthy limb. Microsurgery. 2017;37(8):881–889. https://doi.org/10.1002/micr.30247
[31] Lin CH, Yamamoto T. Identification of lymph vessels using an indocyanine green camera-integrated operative microscope for lymphovenous anastomosis in the treatment of secondary lymphedema. J Vasc Surg. 2023;11(1):161–166. https://doi.org/10.1016/j.jvsv.2022.06.012
[32] Yamamoto T, Narushima M, Yoshimatsu H, et al. Minimally invasive lymphatic supermicrosurgery (MILS): indocyanine green lymphography-guided simultaneous multisite lymphaticovenular anastomoses via millimeter skin incisions. Ann Plastic Surg. 2014;72(1):67–70. https://doi.org/10.1097/SAP.0b013e3182605580
[33] Akita S, Unno N, Maegawa J, et al. A phase III, multicenter, single-arm study to assess the utility of indocyanine green fluorescent lymphography in the treatment of secondary lymphedema. J Vasc Surg. 2022;10(3):728–737.e3. https://doi.org/10.1016/j.jvsv.2021.09.006
[34] Brebant V, Heine N, Lamby P, et al. Augmented reality of indocyanine green fluorescence in simplified lymphovenous anastomosis in lymphatic surgery. Clin Hemorheol Microcircul. 2019;73(1):125–133. https://doi.org/10.3233/CH-199220
[35] Winters H, Tielemans HJP, Hameeteman M, et al. The efficacy of lymphaticovenular anastomosis in breast cancer-related lymphedema. Breast Cancer Res Treat. 2017;165(2):321–327. https://doi.org/10.1007/s10549-017-4335-0
[36] Chung JH, Baek SO, Park HJ, et al. Efficacy and patient satisfaction regarding lymphovenous bypass with sleeve-in anastomosis for extremity lymphedema. Arch Plastic Surg. 2019;46(1):46–56. https://doi.org/10.5999/aps.2018.00773
[37] Khan AA, Hernan I, Adamthwaite JA, et al. Feasibility study of combined dynamic imaging and lymphaticovenous anastomosis surgery for breast cancer-related lymphoedema. Br J Surg. 2019;106(1):100–110. https://doi.org/10.1002/bjs.10983
[38] Seki Y, Kajikawa A, Yamamoto T, et al. Real-time indocyanine green videolymphography navigation for lymphaticovenular anastomosis. Plastic Reconstr Surg. 2019;7(5):e2253. https://doi.org/10.1097/GOX.0000000000002253
[39] Yang JC, Wu S, Chiang M, et al. Intraoperative identification and definition of ‘functional’ lymphatic collecting vessels for supermicrosurgical lymphatico‐venous anastomosis in treating lymphedema patients. J Surg Oncol. 2018;117(5):994–1000. https://doi.org/10.1002/jso.25014
[40] Visconti G, Hayashi A, Bianchi A, et al. Lymphaticovenular anastomosis for advanced-stage peripheral lymphedema: expanding indication and introducing the hand/foot sign. J Plastic Reconstr Aesth Surg. 2022;75(7):2153–2163. https://doi.org/10.1016/j.bjps.2022.02.012
[41] Hara H, Mihara M. Multi-area lymphaticovenous anastomosis with multi-lymphosome injection in indocyanine green lymphography: a prospective study. Microsurgery. 2019;39(2): 167–173. https://doi.org/10.1002/micr.30398
[42] Lasso JM, Alonso-Farto JC. Indocyanine green-guided liposuction for patients presenting with residual nonpitting edema after lymphovenous anastomosis. J Plastic Reconstr Aesth Surg. 2022;75(8):2482–2492. https://doi.org/10.1016/j.bjps.2022.02.081