SYSTEMATIC REVIEW
Clinical outcome comparison of suture button suspensionplasty versus trapeziectomy with ligament reconstruction and tendon interposition in patients with carpometacarpal joint arthritis: a systematic review of direct comparison studies
Wildan Latiefa, Riky Setyawanb and Winona Andrari Mardhitiyanib
aHand and Microsurgery Division, Department of Orthopaedics and Traumatology, Cipto Mangunkusumo Hospital, Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia; bDepartment of Orthopaedics and Traumatology, Cipto Mangunkusumo Hospital, Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia
ABSTRACT
Introduction: Trapeziectomy nowadays is predominantly done with Ligament Reconstruction and Tendon Interposition (LRTI) or Suture Button Suspensionplasty (SBS). This article is intended to highlight comparison between SBS and trapeziectomy with LRTI through direct comparison evidence.
Material and Method: The LRTI technique involves the removal of the diseased trapezium bone and creating suspension through the use of flexor carpi radialis tendon, while SBS stabilize the metacarpal base by suspending the first metacarpal bone. The record screening process of this systematic and meta-analysis was in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis guidelines. QuickDASH, post-operative strength, visual analog scale were set as the primary outcomes, while the adverse event reported and miscellaneous findings worth mentioning per study were set as the secondary outcomes.
Results: Of the 102 records screened, 1 Randomized Control Trial (RCTs) and 1 Cohorts, consisting of 188 cases were included in the analysis. Both modalities showed comparable, non-significant difference in efficacy (alleviating pain associated with basal joint arthritis, improving strength and function of the affected thumb, in the long term) at the endpoint of the follow-up. Both procedures also showcased excellent safety and long-term functional profile. However, SBS displayed an advantage in post-operative recovery aspect as well as the biomechanical aspect compared to LRTI.
Conclusions: Both LRTI & SBS demonstrated non-inferiority to each other, hence clinical judgment might be more based on the preference and tolerability of the patient, as well as the experience of the center. Further prospective, comparative study might be needed to truly erect the superiority of one of the procedures to another.
KEYWORDS: Carpometacarpal joint arthritis; ligament reconstruction and tendon interposition; suture button suspensionplasty; trapeziectomy
Citation: Journal of Plastic Surgery and Hand Surgery 2026; 61: 12–16. DOI: https://doi.org/10.2340/jphs.v61.44912.
Copyright: © 2026 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 13 April 2025; Accepted: 10 September 2025; Published: 11 February 2026
CONTACT: Wildan Latief wildan2510@gmail.com Hand and Microsurgery Division, Department of Orthopaedics and Traumatology, Cipto Mangunkusumo Hospital, Faculty of Medicine, Universitas Indonesia, Jl. Salemba Raya No. 6, Central Jakarta 10430, Indonesia
Competing interests and funding: The authors report that there are no competing interests to declare.
Private funding.
Introduction
Basal joint arthritis, also known as carpometacarpal arthritis of the thumb, is a degenerative condition affecting the basal joint of the thumb. This joint is located at the base of the thumb and is responsible for the thumb’s dexterity and manipulative function. The unique anatomy of the basal joint, which includes the saddle morphology of the trapezium and a stout complement of ligamentous constraints, makes it susceptible to arthrosis and degenerative changes [1]. Basal joint arthritis can cause considerable pain and disability, particularly in postmenopausal females. The prevalence of carpometacarpal arthritis is relatively high, with 7% reported in men and 15% in women [1, 2]. Symptoms of the condition include pain, weakness, and instability that can severely limit hand function. Treatment options focus on removing the diseased trapezium and stabilizing the metacarpal base, with newer options such as carpometacarpal arthroplasty potentially improving function in some patients. [2]
Conservative treatment, such as medications, orthoses, and steroid injections, can be effective in early disease, but surgery is often required in advanced cases [2]. Surgical treatment options for basal joint arthritis include excisional arthroplasty, tendon interposition, ligament reconstruction, implant arthroplasty, and arthroscopy. The choice of treatment depends on the severity of the arthritis and the individual patient’s needs. To the best of the authors’ knowledge, not one of these techniques has been proven to be superior to the others [1, 3].
The surgical treatment of carpometacarpal arthritis, specifically using trapeziectomy and suspensionplasty, is a common procedure for patients suffering from this condition. Trapeziectomy nowadays is predominantly done with Ligament Reconstruction and Tendon Interposition (LRTI) technique, which involves the removal of the diseased trapezium bone and creating suspension through the use of flexor carpi radialis (FCR) tendon, while Suture Button Suspensionplasty (SBS) aims to stabilize the metacarpal base by suspending the first metacarpal bone. This procedure has been shown to improve range of motion, pain relief, and overall hand function in patients with thumb carpometacarpal arthritis [4, 5, 6, 7]. The success rate and the efficacy of trapeziectomy and suspensionplasty varies among patients, with some studies reporting a low risk of complications within 1 year of surgery [8]. However, there is no conclusive evidence of superiority between trapeziectomy and suspensionplasty, hence further investigation was required.
This article is intended to show a comparison between SBS and resection arthroplasty using trapeziectomy with LRTI technique to help physicians determine which technique to use for their patients, considering both the efficacy and safety profile of both modalities.
Methods
Study design
This systematic and meta-analysis was done according to Cochrane Handbook for Systematic Review [9]. The record screening process of this systematic and meta-analysis was in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines [10]. Records of any interventional human studies about trapziectomy with LRTI technique, SBS, or direct comparison between both, including RCTs and cohorts were included. Meanwhile records that are inaccessible, written in non-English language, and written in gray paper, guideline, review, case-report and case-series, and study protocol format were excluded.
Search strategy
Records searching process was done on major medical databases, namely Medline (PubMed), Cochrane, and Elsevier (Scopus). Individual searches were performed through google and google scholar search engines. Combinations of keywords containing ‘basal joint arthritis’ or ‘carpometacarpal joint arthritis’, ‘suspensionplasty’ and ‘suture button’, ‘trapeziectomy’ and ‘ligament reconstruction and tendon interposition’ were used. The screening process of this study is displayed in PRISMA flowchart as displayed in Figure 1.
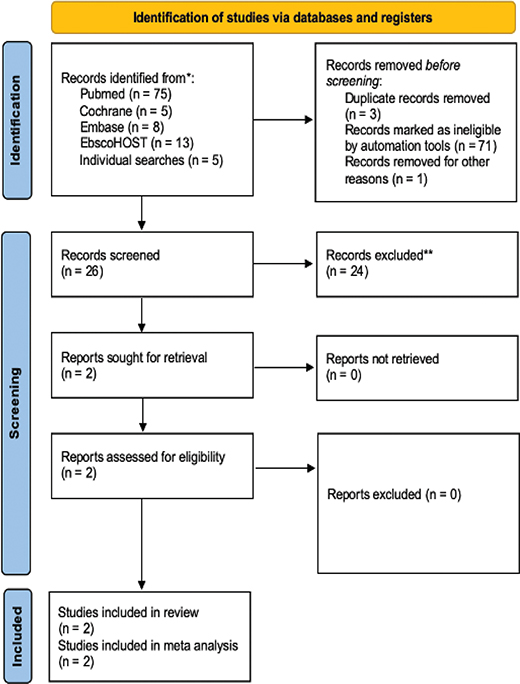
Figure 1. PRISMA flowchart of study screening process.
Data extraction process, analysis, and risk of bias assessment
During data extraction, the authors decided to set QuickDASH, post-operative strength, subsidence (through trapezial space ratio or the ratio of metacarpal length divided by trapezial space length) and visual analog scale (VAS) as the primary outcomes, while the adverse event reported and miscellaneous findings worth mentioning per study as the secondary outcomes. Meanwhile, qualitative analysis was carried out using narrative synthesis technique based on notable findings per study. Sensitivity and subgroup analysis were carried out to address heterogeneity. During data extraction, the authors were also simultaneously assessing the risk of bias. RoB 2 tool was used for RCT while ROBINS-I was used for cohort studies.
Results
Study results and risk of bias
Of the 102 records screened, only two records were deemed to be suitable for the topic. The records were consisting of 1 RCT and 1 cohort. The entire article selection process is displayed in Figure 1. A total of 188 cases, consisted of 96 SBS cases and 92 LRTI cases, were included in the analysis. Risk of bias assessment yielded low risk of bias for the RCT by Morais et al., while the author deemed study by Shonuga et al. and Winiger et al. to be high in risk of bias, as demonstrated in Figure 2. Overall, the study characteristics were summarized in Table 1, while outcome specific information is tabulated in Table 2. Due to graphical error displayed and unavailable SD data in the article by Shonuga et al., the author was unable to proceed to meta-analysis.
| Author, year | Study design | Subject characteristics | Intervention characteristics | |||||
| Mean age | Eaton & littler severity (median) | LRTI/SBS | Male (%) | Loss-to-follow up (%) | Follow up duration (post-op) | Surgical technique details | ||
| Shonuga et al., 2021 [11] | RCT | 63.1 | Eaton III–IV (NA) | 53/59 | 28.5% | 9/121 (7.5%) | 2 weeks, 3 months, and 1 year | Operators: 8 fellowship-trained orthopedic surgeons LRTI: Abductor policis longus & flexor carpi ulnaris as the suspension SBS: Placing button (Mini TightRope©) on the index metacarpal base |
| Morais et al., 2021 [12] | Cohort | 61.4 | Eaton II–IV (III) | 39/37 | 7.8% | 5/81 (6.1%) | 40 months | Operators: 1 person fellowship-trained orthopedic surgeon LRTI: Flexor carpi ulnaris tendon as suspension SBS: Placing button (Mini TightRope©) on the index metacarpal base and second button in index metacarpal cortex |
| Wininger et al., 2023 [13] | Cohort | 60 | 25/6 | 17% | 12, 18, and 60 months | Operators: 1 person fellowship-trained orthopedic surgeon LRTI: Flexor carpi ulnaris tendon as suspension SBS: Placing button (Mini TightRope©) on the index metacarpal base and second button in index metacarpal cortex |
||
| LRTI: Ligament Reconstruction and Tendon Interposition; SBS: Suture Button Suspensionplasty; RCT; Randomized Control Trial. | ||||||||
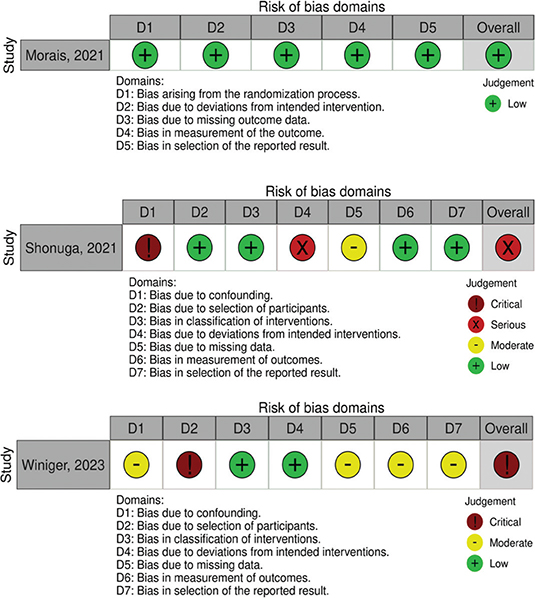
Figure 2. Traffic light plot for risk of bias assessment of included records.
| Author, year | Group | Pain domain (VAS) | Strength domain (lateral/key test) | Functional domain (QuickDASH) | Subsidence domain (Trapeziometacarpal index) | Safety profile and commentaries | ||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | |||
| Morais et al., 2021 [12] | LRTI Pre (40 months) | 4.8 | 2.3 | 3.8 | 1.4 | 59.8 | 21.3 | 0.364 | 0.012 | 7/76 experienced post-op complication, 3 in LRTI & 4 in SBS. LRTI was reported to have longer operation and peri-operative recovery time, with p <0.05 for operative time (MD 28 min), immobilization time (MD 4 weeks), physical therapy (MD 6.2), and time to do normal activity (MD 2 weeks) |
| LRTI Post (40 months) | 1.4 | 1.2 | 4.4 | 0.8 | 30.1 | 17.8 | 0.262 | 0.08 | ||
| SBS Pre (40 months) | 4.3 | 3.1 | 3.1 | 1.7 | 62.1 | 26.4 | 0.368 | 0.011 | ||
| SBS Post (40 months) | 1.5 | 1.4 | 4.3 | 0.6 | 31.6 | 20.3 | 0.304 | 0.06 | ||
| Shonuga et al., 2021 [11] | LRTI Pre (1 year) | 6.6 | NA | 5.39 | NA | 55.9 | NA | 0.26 | NA | No peri and post-operative complication reported in 2 groups. |
| LRTI Post (1 year) | 0.6 | 5.2 | 7.5 | 0.13 | ||||||
| SBS Pre (1 year) | 7.2 | 3.96 | 62 | 0.27 | ||||||
| SBS Post (1 year) | 0.3 | 5.7 | 21.5 | 0.13 | ||||||
| Wininger et al., 2023 [13] | LRTI Pre (1 year) | NA | NA | 3.2 | NA | 50 | NA | NA | NA | Complications occurred in 12.2% patients who underwent LRTI and in 13.3% who underwent SBS. The most common complications in both groups were paresthesias, dysesthesias, or neuromas of the superficial radial nerve. There were 6 re-operations reported in the LRTI group and 2 re-operations in the SBS group. The reasons for re-operation in LRTI patients included metacarpophalangeal hyperextension, tendinitis, neuroma, or persistent pain. For the SBS patients, both re-operations were related to hardware issues – one due to prominent hardware and the other due to hardware loosening. |
| LRTI Post (1 year) | NA | NA | 5.5 | NA | 15 | NA | NA | NA | ||
| SBS Pre (1 year) | NA | NA | 3.9 | NA | 40 | NA | NA | NA | ||
| SBS Post (1 year) | NA | NA | 5 | NA | 20 | NA | NA | NA | ||
| VAS: visual analog scale; LRTI: Ligament Reconstruction and Tendon Interposition; SBS: Suture Button Suspensionplasty; SD: standard deviation; MD; Mean Difference. | ||||||||||
Discussion
Comparing the efficacy of trapeziectomy LRTI and SBS and clinical practice implication
Based on the two primary studies alone, both modalities showed comparable, non-significant difference in efficacy (alleviating pain associated with basal joint arthritis, improving strength and function of the affected thumb, as well as the subsidence in the long term) at the endpoint of the follow-up. These results are backed by the result presented in Liu et al. meta- analysis [14]. This finding demonstrates that both LRTI and suspensionplasty should be done without considering the long-term outcome as both are equally efficacious at the follow-up endpoint. A similar systematic review about indirect comparison between SBS & LRTI by Winiger et al. also resulted in relative equality between the two procedures, in term of functional aspect (QuickDASH), strength (key pinch and grip strength), and the adverse event, further backing up the non-inferiority of both procedures compared to each other [13].
The authors argue that choosing the options should be more oriented on the tolerability, the preference of the patients, and the one the surgeon most familiarized with. A study by Deutch et al., stated that most of the surgeon preferred trapeziectomy with LRTI compared to SBS, while the younger, newer surgeons preferred SBS as their technique of choice. These preferences were built based on clinical experience rather than other, more objective reasonings such as ‘current evidence’ and ‘training’ [15].
One must also observe that statistically significant different must always be clinically correlated, as small enough difference might as well be clinically insignificant. In these comparative studies, there were several significant, albeit small difference, between SBS and LRTI, as reported by Shonuga et al. The SBS was shown to be more resilient to subsidence in 3 months, and better overall QuickDASH profile. These results, however, did not conform to those demonstrated by another superior study by Morais et al., which showed relatively indifferent result. Moreover, several studies, as reported by Morais et al. and Guerrero et al., mentioned that SBS offers significantly earlier mobilization post-operation, return to normal activity, and shorter operation time [16]. This difference, however, remains inconclusive due to many confounding variables still unaddressed, though offering somewhat weak evidence about the shorter relieve and operation duration SBS can offer. Either way, the authors argued that the difference might just be minute to non-existent.
The biomechanical aspect of both modalities has been researched and yielded the superiority of SBS. A study by Desai et al. on cadaveric model showcased SBS to be better at resisting metacarpal subsidence compared to LRTI, though resting subsidence of both groups did not differ. This means that SBS might offer a more stable joint placement if strained to higher degree. Even still, the clinical implication of the higher stress-resistance and stability of SBS is still vague [17].
Safety profile
Both procedures displayed excellent safety profile, with low-to-none rate of having reoperation. In terms of total complication rate, however, SBS displayed smaller rate of complication compared to LRTI. However, post-operative complications caused by either procedures were reported to be tolerable, hence less need for corrective operation. A larger, non-direct comparative systematic review by Winiger et al. also supported the stance of minimal adverse event and reoperation rate of both procedures. This reinforces our finding about the excellent and consistent safety profile of both LRTI & SBS [13].
Surgical technique aspect and biomechanical comparison of LRTI and SBS
LRTI is the gold standard for terminal CMC 1 arthritis. This technique is the evolution of simple trapeziectomy technique and has been put into clinical practice for over 50 years now. Posterolateral triradiate incision is made to expose trapeziometacarpal joint, of which the tendon of FCR or Abductor Policis Longus (APL), along with a guide wire called Kishner wire, are used to secure the base of first metacarpal bone to the base of second metacarpal, with the thumb projection, ideally, being coaxis to the scaphoid, the base of thumb metacarpal is at the same level as the index metacarpal, and the position of thumb tip in a fist should be at the middle row of index finger [18]. The LRTI aspect of the trapeziectomy is supposedly done to increase thumb stability and range of motion, however a biomechanical study by Luria et al., comparing trapeziectomies with and without implant showed no significant difference between LRTI, simple trapeziectomy, and trapeziectomy with either ligament reconstruction or tendon interposition [19]. This result, however, does not translate well clinically, as several studies mentioned better grip and tip strength [20, 21, 22].
Meanwhile, SBS is a form of basal joint arthritis, of which an implant called suture button is placed on the dorsolateral aspect of metacarpal bone of the thumb and the metacarpal bone of the index. This technique is relatively new compared to conventional trapeziectomies. This implant acts as anchors for suspension created from tendon graft, usually harvested from APL [23, 24]. Suspensionplasty is found to be more resistant to subsidence compared to conventional trapeziectomy and LRTI [17, 24]. The SBS, despite being a newer procedure, has been proven to be efficacious in alleviating pain, improving strength, and increasing the range of motion of the affected thumb by several studies [25, 26, 27, 28].
Strength and weakness of this review
This review offered the first qualitative evidence of a direct comparison between SBS and LRTI. This study might play a pivotal role for better clinical judgment, on how to choose between the two, and provide foundation for further prospective, comparative study between SBS and LRTI. The evidence presented by Morais et al. is also deemed to be of high quality due to the singular operator and successful randomization, hence the authors could exert a higher degree of certainty on the evidence produced.
Even so, the lack of study size and number of centers included served as the biggest downside of this study. The evidence offered by Shonuga et al. was found to be high in risk of bias and several critical faults in this publication were identified, such as the absence of SD value, erroneous graphical representation of the data, and a lack of clarity in sociodemographic characteristics, even though the sample size is larger compared to Morais et al. This caused the authors to be unable to proceed with a quantitative analysis. Despite so, the relative consistency of the lack of difference between SBS and LRTI could still be inferred from both studies, hence the consistency of the findings itself.
Conclusion and recommendation
Both LRTI and SBS yielded excellent clinical efficacy and safety profile. Both demonstrated non-inferiority to each other, hence clinical judgment might be more based on the preference and tolerability of the patient, as well as the experience of the center. The SBS offers a shorter recovery and operating time, but this is still a somewhat weak evidence. Further prospective, comparative study might be needed to truly erect the superiority of one of the procedures to another.
Authors’ contributions
WL conceived the ideas of the study, performed data analysis and interpretation, provided grammatical revisions to scientific content of manuscript.
RS and WAM wrote the manuscript, carried out data analysis and interpretation, and provided grammatical revisions to manuscript.
References
[1] Ishikawa H. The latest treatment strategy for the rheumatoid hand deformity. J Orthop Sci. 2017;22(4):583–592. https://doi.org/10.1016/j.jos.2017.02.007
[2] Bakri K, Moran SL. Thumb carpometacarpal arthritis. Plast Reconstr Surg. 2015;135(2):508–520. https://doi.org/10.1097/PRS.0000000000000916
[3] Klim SM, Glehr R, Graef A, et al. Total joint arthroplasty versus resection-interposition arthroplasty for thumb carpometacarpal arthritis: a randomized controlled trial. Acta Orthop. 2023;94:224–229. https://doi.org/10.2340/17453674.2023.11919
[4] Shinya Y, Ikeguchi R, Noguchi T, et al. Radiographic evaluation after arthroscopic partial trapeziectomy with suture- button suspensionplasty for thumb carpometacarpal arthritis. Plast Reconstr Surg Glob Open. 2023;11(5):E4983. https://doi.org/10.1097/GOX.0000000000004983
[5] Wejnold Jørgensen R, Odgaard A, et al. Patient-reported outcomes following interposition arthroplasty of the basal joint of the thumb. J Plast Surg Hand Surg. 2021;55(2):105–110. https://doi.org/10.1080/2000656X.2020.1830101
[6] Molin U, Evans K, Wilcke M. Does proximal migration of the first metacarpal correlate with remaining pain after trapeziectomy? J Plast Surg Hand Surg. 2022;56(1):11–15. https://doi.org/10.1080/2000656X.2021.1898975
[7] Yoon AP, Hutton DW, Chung KC. Cost-effectiveness of surgical treatment of thumb carpometacarpal joint arthritis: a value of information study. Cost Eff Resour Alloc. 2023;21(1):28. https://doi.org/10.1186/s12962-023-00438-8
[8] Landes G, Gaspar MP, Goljan P, et al. Arthroscopic trapeziectomy with suture button suspensionplasty: a retrospective review of 153 cases. Hand. 2016;11(2):232–237. https://doi.org/10.1177/1558944715616955
[9] Higgins JPT, Thomas J, Chandler J, et al. Cochrane handbook for systematic reviews of interventions version 6.4 [Internet]. 2023 [cited 2024 May 8]. Available from www.training.cochrane.org/handbook
[10] Page MJ, McKenzie JE, Bossuyt PM, et al. The The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. https://doi.org/10.1136/bmj.n71
[11] Shonuga O, Nicholson K, Abboudi J, et al. Thumb-basal joint arthroplasty outcomes and metacarpal subsidence: a prospective cohort analysis of trapeziectomy with suture button suspensionplasty versus ligament reconstruction with tendon interposition. Hand (N Y). 2023;18(1):98–104. https://doi.org/10.1177/1558944721994227
[12] Morais B, Botelho T, Marques N, et al. Trapeziectomy with suture-button suspensionplasty versus ligament reconstruction and tendon interposition: a randomized controlled trial. Hand Surg Rehabil. 2022;41(1):59–64. https://doi.org/10.1016/j.hansur.2021.10.315
[13] Winiger AE, Orozco EI, Han A, et al. Systematic comparison of ligament reconstruction with tendon interposition and suture-button suspensionplasty for trapeziometacarpal osteoarthritis. Hand (N Y). 2023;18(7):1069–1079. https://doi.org/10.1177/15589447211043217
[14] Liu Q, Xu B, Lyu H, et al. Differences between simple trapeziectomy and trapeziectomy with ligament reconstruction and tendon interposition for the treatment of trapeziometacarpal osteoarthritis: a systematic review and meta-analysis. Arch Orthop Trauma Surg. 2022;142(6):987–996. https://doi.org/10.1007/s00402-020-03707-w
[15] Deutch Z, Niedermeier SR, Awan HM. Surgeon preference, influence, and treatment of thumb carpometacarpal arthritis. Hand (N Y). 2018;13(4):403–411.
[16] Guerrero EM, Ferlauto HR, Grier AJ, et al. Suspensionplasty for revision thumb carpometacarpal osteoarthritis surgery: comparing suture button suspensionplasty to ligament reconstruction and tendon interposition. Plast Reconstr Surg. 2022;150(3):601–605. https://doi.org/10.1097/PRS.0000000000009408
[17] Desai MJ, Brogan DM, Richard MJ, et al. Biomechanical comparison of suture-button suspensionplasty and LRTI for basilar thumb arthritis. Hand (N Y). 2016;11(4):438–443.
[18] Karbach LE, Elfar J. Elbow instability: anatomy, biomechanics, diagnostic maneuvers, and testing. J Hand Surg Am. 2017;42(2):118–126. https://doi.org/10.1016/j.jhsa.2016.11.025
[19] Luria S, Waitayawinyu T, Nemechek N, et al. Implant arthroplasty for thumb carpometacarpal arthritis : a cadaver. Hand Surg. 2007; 32A:697–706. https://doi.org/10.1016/j.jhsa.2007.02.025
[20] Field J, Buchanan D. To suspend or not to suspend: a randomised single blind trial of simple trapeziectomy versus trapeziectomy and flexor carpi radialis suspension. J Hand Surg Eur Vol. 2007;32(4):462–466. https://doi.org/10.1016/J.JHSB.2007.02.005
[21] Gangopadhyay S, McKenna H, Burke FD, et al. Five- to 18-year follow-up for treatment of trapeziometacarpal osteoarthritis: a prospective comparison of excision, tendon interposition, and ligament reconstruction and tendon interposition. J Hand Surg Am. 2012;37(3):411–417. https://doi.org/10.1016/j.jhsa.2011.11.027
[22] Belcher HJCR, Nicholl JE. A comparison of trapeziectomy with and without ligament reconstruction and tendon interposition. J Hand Surg Am. 2000;25 B(4):350–356. https://doi.org/10.1054/jhsb.2000.0431
[23] Yao J. Suture-button suspensionplasty for the treatment of thumb carpometacarpal joint arthritis. Hand Clin. 2012;28(4):579–585. https://doi.org/10.1016/j.hcl.2012.08.013
[24] Lui H, Galbraith JG, Meyers K, et al. Biomechanical analysis of three techniques of suspensionplasty after trapeziectomy: a cadaveric study. J Hand Surg. 2023;48(11):1201–1206. https://doi.org/10.1177/17531934231186495
[25] Assiotis A, Giannakakis N, Hacker A. Trapeziumectomy and mini tightrope stabilization of the first metacarpal for thumb carpometacarpal osteoarthritis : a prospective case series. Acta Orthop Belg. 2017;83(3):473–479.
[26] Avant KR, Nydick JA, White BD, et al. Basal joint osteoarthritis of the thumb: comparison of suture button versus abductor pollicis longus suspensionplasty. Hand. 2015;10(1):80–84. https://doi.org/10.1007/s11552-014-9653-7
[27] González C, Suarez D, Vanegas D, et al. Trapezium bone resection arthroplasty and suspension with suture button for the treatment of trapeziometacarpal osteoarthritis: long-term follow-up in a colombian cohort. J Hand Surg Glob Online. 2019;1(2):96–100. https://doi.org/10.1016/j.jhsg.2018.12.003
[28] Parry JA, Kakar S. Dual mini tightrope suspensionplasty for thumb basilar joint arthritis: a case series. J Hand Surg Am. 2015;40(2):297–302. https://doi.org/10.1016/j.jhsa.2014.10.057