SYSTEMATIC REVIEW
Current materials and techniques in cosmetic hand injections
Yutong Liang, MDa*, Jun Zhuang, MDb*, Xueshang Su, MDa, Ziming Zhang, MDa, Qingqian Wei, MDa and Jintian Hu, MDa*
aDepartment of Cosmetic Injection Center, Plastic Surgery Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, P.R. China; bDepartment of Ear Reconstruction, Plastic Surgery Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China
ABSTRACT
Background: With the widespread popularity and development of aesthetic treatments, the focus has extended from facial aging to include the aging of hands. The primary aim of this study is to review the current materials, methods of injection, and testing procedures employed in cosmetic hand injections.
Methods: PubMed database (from 1971 to April 2024) was searched to identify relevant studies on materials, injection techniques, and evaluation methods associated with aesthetic hand injections, excluding systematic reviews and medical record reports.
Results: A total of 1815 articles were identified, of which 41 articles were included. This study summarizes the current materials, injection techniques, and outcome evaluation methods used for cosmetic hand injections, while discussing observations and making recommendations.
Conclusion: Hand skin conditions tend to receive less attention than cosmetic facial injections. In existing studies of injected substances, hydroxyapatite remains the main material used for cosmetic hand injections. Poly-L-lactic acid (PLLA), platelet-rich plasma (PRP), and polycaprolactone injections were significantly more effective than other substances in the hand. In commonly used injection techniques, catheter-based injection methods are more accurate than needle positioning and dose. The most commonly used assessment methods remain ultrasound and the Merz hand partial scale. At present, there is still a relative lack of research on aesthetic hand injections, and extensive and in-depth research, such as randomized studies comparing hyaluronic acid and calcium hydroxylapatite and longitudinal data on the results of PLLA or PRP, is recommended to further develop hand injection techniques with lasting aesthetic results. Increased public awareness of hand injections derives from more reliable and valid studies. And we need standardized outcome measures and long-term follow-up data in future studies.
KEYWORDS: hand; injections; rejuvenation
Citation: Journal of Plastic Surgery and Hand Surgery 2026; 61: 78–85. DOI: https://doi.org/10.2340/jphs.v61.45435.
Copyright: © 2026 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 6 October 2024; Accepted: 5 January 2026; Published: 23 April 2026.
CONTACT: Jintian Hu, MD hujintian@vip.163.com Department of Cosmetic Injection Center, Plastic Surgery Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Thirty-three Badachu Road, Shijingshan District, Beijing, P.R. China
*Yutong Liang and Jun Zhuang contributed equally to this work.
Competing interests and funding: None declared.
None.
Introduction
As age changes, the problem of hand aging becomes more and more prominent, and patients’ needs for improving the condition of their hands gradually increase [1]. The popularity of facial rejuvenation surgery and the increasing availability of treatments have prompted an increased demand for hand rejuvenation of up to 60% [2, 3]. In fact, an article published in Plastic and Reconstructive Surgery as early as 2006 proposed that hand condition can independently reflect a person’s age [4]. A study points to an increased need to close the gap between youthful faces and aging hands; at the same time, as the use of masks becomes routine during and after the COVID-19 pandemic, hands have become the first visible sign of the body’s aging index [5, 6]. Soft-tissue volume is the most important factor in perceived hand esthetics [7]. Aging of the hands can manifest as soft-tissue atrophy, wrinkling, increased discoloration, excessive protrusion of bones, tendons, veins, etc [8, 9]. Similar to the face, improvements to the hands can be divided into two main categories: surgical and non-surgical. Autologous fat grafting is the preferred surgical option, combined with laser or chemical treatment of the epidermis [10]. Non-surgical techniques include dermal filler injections. Fillers have the advantages of convenience, satisfaction, and minimal trauma [11, 12]. They are widely accepted by patients and are a common technique for hand rejuvenation. This systematic review summarizes the commonly used, safe, and effective injection materials as well as the existing injection and detection methods, which provides ideas for the follow-up research on hand injection materials and calls on more researchers to pay more attention to the problem of hand aging.
Methods
Search keywords and data extraction
The authors searched the PubMed database for studies related to hand injections until the end of April 2024, including the injection site (hand), injection materials (hyaluronic acid [HA], calcium hydroxylapatite [Ca-HA], collagen, poly-L-lactic acid [PLLA], polycaprolactone [PCL], platelet-rich plasma [PRP], and botulinum toxin), needle specifications (size and diameter), detection methods (ultrasound analysis), and observation indicators. The authors limited the search to English language reports and exclude reports not related to the subject, non-English reports, or reports related to other injection sites and methods. Specific inclusion and exclusion criteria are shown in Table 1.
Data management and excursion assessment
This review was conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. All articles were independently screened by three investigators, and those that met the inclusion criteria were screened. Systematic reviews and meta-analyses were excluded due to the lack of original experimental data, while case reports were excluded because of their strong individuality and limitations. In case of uncertainty, three investigators discussed the relevant articles and reached consensus, summarizing from three aspects: injection material, injection method, and evaluation method.
Results
Overall distribution
Of the 1815 studies identified, a total of 41 studies were finally included after screening against exclusion criteria (Figure 1). Of the remaining 41 articles, 30 were related to hand injection materials, of which 10 were related to HA (33.3%), 8 to Ca-HA (26.7%), 5 to PLLA application in the hand (16.7%), 1 to PCL (3.3%), and 3 to PRP application in the hand (10%). Because Botox is mainly used in the treatment of hand diseases, there is no literature on hand injection rejuvenation. Thirty studies were related to the injected material, two to the method of injection, and nine to the method of examination. The specific data are shown in Table 2.
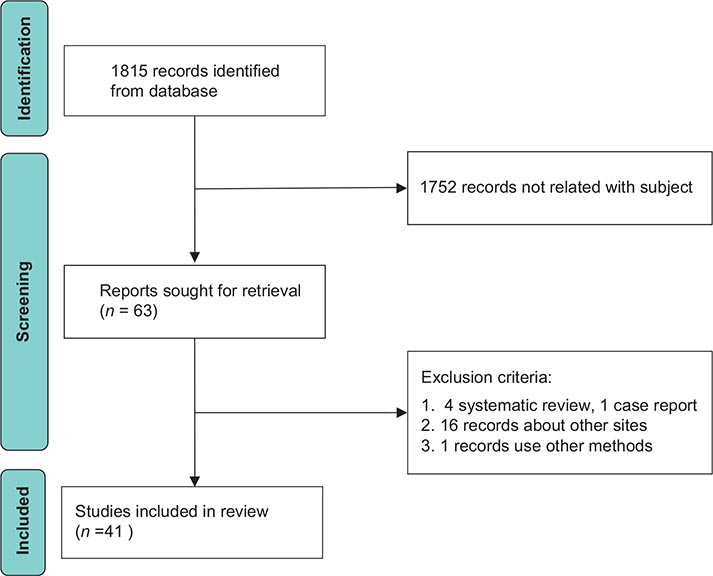
Figure 1. Flowchart of the literature screening process.
Injection materials
Among the 30 articles related to hand injection materials, 10 were HA related (33.3%), 8 were Ca-HA related (26.7%), 5 were about the application of PLLA in hand (16.7%), 1 was about PCL (3.3%), and 3 were about the hand application of PRP (10%) (Figure 2). Because Botox is mainly used for the treatment of hand diseases, there is no literature on hand injection beauty. The properties of different hand injection materials are shown in Table 2.
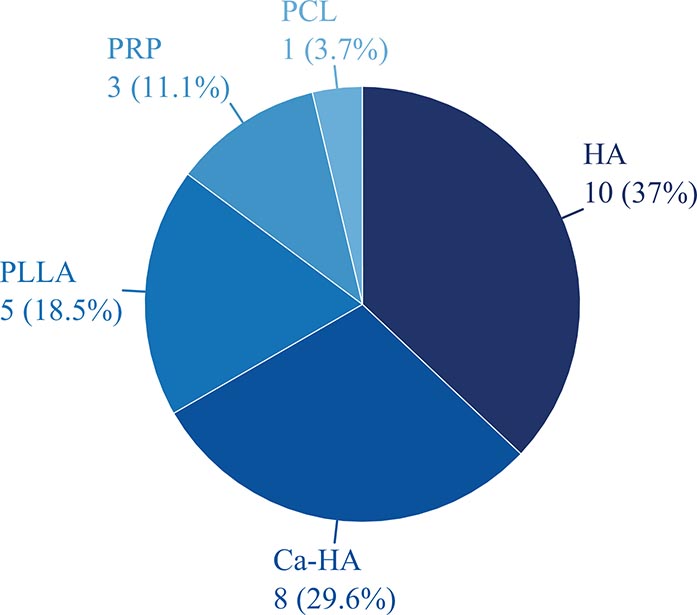
Figure 2. Distribution of different materials in the 30 studies related to injection materials that were included. PLLA: poly-L-lactic acid; PRP: platelet-rich plasma; PCL: polycaprolactone; HA: hyaluronic acid; Ca-HA: calcium hydroxylapatite.
Hyaluronic acid
HA is the most common dermal filler used for both facial and hand treatments [13]. It addresses wrinkles and volume loss not only through filling and volumizing but also by hydrating the injected area (nasolabial folds, popliteal fossa, malar fat pads, leading lines, labial enhancements, and inter-brow lines) due to its water affinity. HA has also been examined as a potential skin restorer in intermediate-effect therapies, which involve multiple microinjections into the dermis to rejuvenate the skin [14]. Following injection, patients achieved safe, effective, and lasting outcomes due to HA’s unique chemical-physical properties, biocompatibility, biodegradability, and versatility [1, 15–21]. There are two types of HA: stable (S-HA) and non-stable (NS-HA). Studies have shown that S-HA has superior effects compared to NS-HA [20, 22]. A study has indicated that HA demonstrated superior efficacy compared to collagen [23]. In addition, recent studies have shown that HA can act as a skin booster. A 2007 study observed fibroblast elongation and collagen regeneration after injecting cross-linked HA fillers into the forearms of 11 elderly patients [24, 25]. Although the improvement after HA injection is significant at all time points, it is still necessary to acknowledge the possible complications, need for remediation, and appropriate dosages [26]. A study tested the effect of large granule HA on initial impressions following hand injection. The results showed that after treatment, the initial impression scores of all experimental groups increased, further demonstrating the effectiveness of HA in hand injections [27].
Calcium hydroxylapatite
Ca-HA is chemically identical to the calcium component of bones and teeth, which provides the product with a high degree of biocompatibility. In recent years, it has been utilized as a radiopaque dermal filler to provide volume correction in the dorsal hands [28]. A 2-year, prospective, single-center, open-label study demonstrated that Ca-HA injections in the hands do not obscure the bones as observed on X-rays up to 24 months post-injection, thus attesting to its safety [29]. Meanwhile, relevant controlled experimental studies have demonstrated that the dorsal intermediate lamina is a loosely structured and easily stretchable layer [30]. Regardless of whether the injection is administered at the sub-dermal level using a cannula or by a needle in the deep fat lamina, there is no significant difference in the injection effect. However, considering patient satisfaction and the risk of adverse reactions, the use of cannulas is recommended [31]. Ca-HA is classified as an adjustable filler, in contrast to HA, which is fully reversible through hyaluronidase digestion. Adverse effects, such as swelling and edema post-injection, are common and can sometimes be debilitating. The combination of certain reagents (e.g. triamcinolone and foam sclerotherapy) without the cosmetic effect not only avoids negatively impacting treatment efficacy but also dramatically reduces adverse effects, thereby improving patient experience and treatment tolerance [32, 33].
Compared to HA, Ca-HA exhibits stronger tissue lifting and skin-tightening effects. Premixing HA with Ca-HA can enhance the collagen-stimulating properties of HA fillers, while high G prime HA can provide additional volume while maintaining tissue softness, thereby enhancing the effectiveness of Ca-HA fillers [34]. Additionally, due to the rapid absorption of the carboxymethyl cellulose gel carrier before the new collagen formation induced by Ca-HA granules takes effect, the area injected with Ca-HA sometimes experiences unexpected early volume loss. Moreover, significantly more bruising and swelling were observed in the hands injected with Ca-HA compared to those injected with HA. When HA is premixed with Ca-HA, HA can compensate for this early volume loss, and Ca-HA is known to have a longer-lasting effect than most types of HA [11]. Therefore, in the long term, the premixing of HA and Ca-HA can extend the duration of the filler treatment’s effect.
Collagen
Collagen, a widely used dermal filler in cosmetic surgery, can be divided into bovine collagen and porcine collagen [35]. Due to its consistency, flow characteristics, lack of longevity, and the resulting uneven skin surface, bovine collagen is rarely used for correcting hand appearance [36]. In the context of hands, unlike faces, collagen is often used in the treatment of post-burn hand malfunctions and certain hand contracture diseases, such as Dupuytren’s Contracture [37, 38].
PRP
The presence of various growth factors in platelets renders PRP a potent tool for stimulating collagen regeneration in aging skin [39]. A recent study conducted a prospective, randomized clinical trial in which 18 women with aged hands received PRP injections into one hand every 4 weeks for a total of 12 weeks, while the other hand received saline injections in a randomized, controlled, single-blind manner. At 12 and 24 weeks of follow-up and evaluation, researchers found only slight skin changes, understanding that PRP may not be an effective option for hand rejuvenation [40]. Furthermore, the application of PRP can reduce the visibility of skin blood vessels, promote collagen synthesis, and increase the number of fibroblasts and blood vessels in the superficial dermis [41]. One study that conducted a controlled clinical trial to investigate the relationship between PRP and fat transplantation concluded that fat grafting with PRP was safe and associated with minimal side effects after 1 year [42].
Poly-L-lactic acid
Hands remain a particularly challenging area to treat with any technique. However, polylactic acid presents a promising solution to this problem [9]. Polylactic acid filler, the first sustained collagen stimulator initially used on the face, can now also be applied to other areas with increased volume, contouring, and loose skin, such as the neck, chest, arms, and thighs. In the hand, PLLA mainly addresses the problem of volume loss and must be injected into the thin subcutaneous layer on the back of the hand, avoiding muscles, tendons, and veins [43]. The US Food and Drug Administration has approved injectable PLLA for the correction of shallow to deep nasolabial fold contour deficiencies, other facial wrinkles, and the restoration and/or correction of signs of facial lipoatrophy related to the human immunodeficiency virus [44]. Some studies have demonstrated that aesthetic restoration of the hands with injectable PLLA may yield satisfactory results, consistent with those reported for facial applications [45, 46].
Polycaprolactone
The non-HA bioresorbable PCL-based filler, known for its collagen-stimulating properties, has a proven safety profile. It is typically used on the face to improve signs of aging and has a low complication rate, with rare cases of nodules and/or granulomas. Although there are not enough reports demonstrating the use of PCL in the hand, PCL filler has been determined to be effective for improving dorsal hand volume loss with minimal side effects [47].
Botulinum toxin
Botulinum toxin is a common facial injection used to mitigate wrinkles and combat aging [48]. However, no research has shown its effectiveness in addressing aging issues in the hand. Instead, it is more commonly used to treat muscle spasms and muscle tone-related diseases, such as systemic sclerosis, Parkinson’s disease, and Raynaud’s syndrome in the hand [49].
Injection methods
The literature on hand injection methods is limited, with only three research reports in this field. Botulinum toxin is primarily used in the hand for treating limb spasms and focal dystonia. A controlled trial compared two types of electrophysiological guidance: electrical stimulation and ultrasound. The study concluded that both methods were equally effective, but ultrasound was recommended for patient comfort [50]. A 2015 study investigated the efficacy and safety of injecting Radiesse® with a needle versus a cannula for hand aging. A 6-month clinical trial involving 10 women with consistent hand aging issues found no significant differences in efficacy or safety between the two injection methods [51]. In addition, a recent study demonstrated that the use of a trocar for injecting soft-tissue fillers can precisely deliver the product to a predetermined tissue plane [52]. Injecting fewer products into deeper tissues improves accuracy. In a 2019 study, a five-step method for hand rejuvenation was proposed for HA injections. The process involves wrapping the skin and injecting the filler perpendicular to the skin while carefully avoiding veins and extensor tendons on the back of the hand. The injection area was then massaged with ultrasonic gel, and a post-injection assessment was conducted [53]. The method of conducting a safety check through ultrasound after a sharp needle injection is rather cumbersome. Therefore, the injection method using a cannula needle to spread the skin and dermis layer on the back of the hand remains the most effective and safe injection method at present.
Examined methods
Ultrasound analysis
Ultrasound is a noninvasive technology that has been widely used in various fields of medicine and plays an important role in hand injections [54]. Atrophy of hand adipose tissue is a key indicator of hand aging. Ultrasound technology has revealed that there are three layers of hand adipose tissue: the dorsal superficial layer (DSL), the dorsal intermediate layer (DIL), and the dorsal deep layer (DDL). The study also found that as age increases, the volume of these three fat layers decreases, with the reduction of the DIL being particularly noticeable after the age of 30 [6].
With advancements in ultrasound technology, skin-targeted ultrasound and high-frequency ultrasound have emerged, both of which are noninvasive technologies. Skin-targeted ultrasound technology revealed that the subepidermal low echo band (SLEB) is associated with chronic ultraviolet radiation [55]. The lower the SLEB echo, the higher the photoaging. Consequently, this technology can be used to evaluate the effectiveness of skin photoaging treatments. High-frequency ultrasound operates at a frequency of 20–100 MHz, which can clearly distinguish each layer of skin. The ultrasound data can be quantified, making it useful for evaluating age-related changes in the dermis [56].
Hand grading scale
The Merz Hand Score (MHGS) is a commonly used scale for physicians to evaluate the condition of their patients’ hands. It is a 5-point scale that can be used for both photographic assessment of the back of the hand and on-site assessment [57]. With its highly weighted K-value and consistent surface, the MHGS is a suitable and tested tool for clinicians to consult with patients and evaluate changes after hand rejuvenation treatment [58].
In 2019, a new hand grading scale, the Hand Volume Rating Scale (HVRS), was proposed. This 5-point numerical rating scale, with 0 (absent), 1 (mild), 2 (moderate), 3 (moderate to severe), and 4 (severe), is used for objectively evaluating the volume change of the hand in Asians. Developed by five experienced plastic surgeons, the scale considers the degree of fat loss and the visibility of veins and tendons as key scoring factors. However, as the participants in the study were all Asians, the applicability of the scale may be limited [59].
Table 3 shows a comparative analysis of ultrasound and the two evaluation scales from the perspectives of sensitivity, reproducibility, and clinical feasibility.
Other method
With the advancement of 3D technology in recent years, it has been integrated into various fields. In the field of injectable esthetics, many handheld 3D systems have emerged, offering a noninvasive, accurate, and repeatable method for evaluating the volume of injections in the face, vulva, and hands. The selection of these systems is based on clinical needs and available resources [60].
Discussion
This systematic review indicates that HA and Ca-HA, according to the number of published studies, are the most commonly used materials for hand rejuvenation injections. The incidence of mild complications is low, and no related serious complications have been reported. Among all the materials, patient satisfaction is high, and the aesthetic effect tends to be more lasting. With the rapid development of facial injection esthetics, the importance placed on the appearance of the hands is gradually increasing, extending beyond the use of hand creams, masks, and other single external methods for hand skin maintenance. Fat transplantation is another method of hand rejuvenation that can fill the defective tissue of the hand to achieve rejuvenation. However, it is more invasive, and the survival rate and maintenance time of the injected fat tissue are limited, with a higher risk of complications [61]. Therefore, compared to fat transplantation to improve the aging state of the hand, people tend to prefer a less invasive, effective, and more lasting aesthetic solution – hand injection.
In plastic surgery, botulinum toxin is frequently used as an anti-aging component for facial treatments [62]. Although there are risks of complications such as headaches, local skin reactions, and facial neuromuscular symptoms, it remains a popular product for facial wrinkle removal when applied with the correct injection method and appropriate dosage [63, 64]. However, our review has found that in the context of hand treatments, unlike its use in facial applications, botulinum toxin is commonly used as a treatment for muscle spasms and dystonia-related disorders, and it is seldom used for cosmetic purposes in the hands [65–68].
Despite the popularity of facial injections, surprisingly, there are very few studies focused on hand injections, and most of the injection materials are already well known [69]. Our review indicates that there have been no new injection materials for hand cosmetic surgery introduced since the research on hand rejuvenation materials conducted 3 years ago, while there are increasingly diverse injection materials available for the face, neck, and eyelids, such as concentrated growth factors (CGFs) [70], stem cells, platelet-rich fibrin (PRF), etc., which are considered safer, more effective, and more durable [71–73]. Concurrently, there are few reports on the cosmetic use of popular injection materials like PLLA, PCL, and PRP, which have been widely used in facial treatments with notable effectiveness and high patient satisfaction, particularly over the past 5 years [71, 74, 75]. Furthermore, no serious complications were reported following the injections, and patient satisfaction was high.
To analyze the reasons, first, this study has certain limitations. Our research only included articles published in English and was restricted to one database, PubMed, without considering other databases, which might lead to a lack of comprehensive data. Second, people tend to prioritize the functional use of their hands over their appearance, resulting in a general neglect of hand esthetics. Consequently, few people opt for hand rejuvenation procedures. The lack of widespread acceptance of hand cosmetics, coupled with insufficient research support, means that during patient consultations, we cannot provide adequate references, thereby reducing the number of potential patients and leading to a lack of clinical data support, forming a vicious cycle. Third, from an evidentiary standpoint, compared to populations in other regions, the issue of hand aging among Asians is not severe. Unless combined with other diseases, normal individuals rarely exhibit serious hand tissue defects as they age, which also contributes to the low number of hand injections.
Based on our systematic review, we have several suggestions regarding hand injections. We recommend that more plastic surgeons focus on research into hand aging, further develop hand injection techniques with long-lasting aesthetic effects, and work toward improving public awareness of hand injections.
Conclusion
At present, beauty hand injection materials that can be used mainly include HA, collagen II, PLLA, Ca-HA, and PRP, in which HA and Ca-HA are reported as widely used materials. Needle and cannula are mainly used for injection. Although there is no significant difference in the injection effect between the two groups, the cannula has higher patient satisfaction and accuracy. Ultrasound and MHGS are still the main methods to evaluate the state of hand aging and the efficacy of treatment. Although there is a lag in hand injections compared to facial injections, with the increased attention and research on hand injections, we believe that plastic surgeons will have to pay more attention to clinical research and clinical practice work on hand injections in the future to find more effective and long-lasting minimally invasive rejuvenation materials.
Financial disclosure statement
The authors have no financial interest to declare in relation to the content of this article.
Disclosures
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Data acquisition
The datasets generated and/or analyzed during the current study are not publicly available but are available from the corresponding author upon reasonable request.
Ethical approval
Not required.
References
[1] Moradi A, Allen S, Bank D, et al. A prospective, multicenter, randomized, evaluator-blinded, split-hand study to evaluate the effectiveness and safety of large-gel-particle hyaluronic acid with lidocaine for the correction of volume deficits in the dorsal hand. Plast Reconstr Surg. 2019;144(4):586e–596e. https://doi.org/10.1097/PRS.0000000000006070
[2] Fabi SG, Goldman MP. Hand rejuvenation: a review and our experience. Dermatol Surg. 2012;38(7 Pt 2):1112–1127. https://doi.org/10.1111/j.1524-4725.2011.02291.x
[3] Bidic SM, Hatef DA, Rohrich RJ. Dorsal hand anatomy relevant to volumetric rejuvenation. Plast Reconstr Surg. 2010;126(1):163–168. https://doi.org/10.1097/PRS.0b013e3181da86ee
[4] Bains RD, Thorpe H, Southern S. Hand aging: patients’ opinions. Plast Reconstr Surg. 2006;117(7):2212–2218. https://doi.org/10.1097/01.prs.0000218712.66333.97
[5] Fathi R, Cohen JL. Challenges, considerations, and strategies in hand rejuvenation. J Drugs Dermatol. 2016;15(7):809–815.
[6] Hung YT, Cheng CY, Chen CB, Huang YL. Ultrasound analyses of the dorsal hands for volumetric rejuvenation. Aesthet Surg J. 2022;42(10):1119–1126. https://doi.org/10.1093/asj/sjac035
[7] Eberlin KR, Chang J, Curtin CM, Sammer DM, Saint-Cyr M, Taghinia AH. Soft-tissue coverage of the hand: a case-based approach. Plast Reconstr Surg. 2014;133(1):91–101. https://doi.org/10.1097/01.prs.0000436831.73323.88
[8] Butterwick KJ. Lipoaugmentation for aging hands: a comparison of the longevity and aesthetic results of centrifuged versus noncentrifuged fat. Dermatol Surg. 2002;28(11):987–991. https://doi.org/10.1097/00042728-200211000-00003
[9] Redaelli A. Cosmetic use of polylactic acid for hand rejuvenation: report on 27 patients. J Cosmet Dermatol. 2006;5(3):233–238. https://doi.org/10.1111/j.1473-2165.2006.00259.x
[10] Abergel RP, David LM. Aging hands: a technique of hand rejuvenation by laser resurfacing and autologous fat transfer. J Dermatol Surg Oncol. 1989;15(7):725–728. https://doi.org/10.1111/j.1524-4725.1989.tb03619.x
[11] Kim JS. Detailed sonographic anatomy of dorsal hand augmentation with hyaluronic acid and calcium hydroxyapatite fillers. Aesthet Surg J. 2019;39(10):1096–1106. https://doi.org/10.1093/asj/sjy227
[12] Guida S, Galadari H. A systematic review of Radiesse/calcium hydroxylapatite and carboxymethylcellulose: evidence and recommendations for treatment of the face. Int J Dermatol. 2024;63(2):150–160. https://doi.org/10.1111/ijd.16888
[13] Fallacara A, Manfredini S, Durini E, Vertuani S. Hyaluronic acid fillers in soft tissue regeneration. Facial Plast Surg. 2017;33(1):87–96. https://doi.org/10.1055/s-0036-1597685
[14] Greene JJ, Sidle DM. The hyaluronic acid fillers: current understanding of the tissue device interface. Facial Plast Surg Clin North Am. 2015;23(4):423–432. https://doi.org/10.1016/j.fsc.2015.07.002
[15] Wilkerson EC, Goldberg DJ. Small-particle hyaluronic acid gel treatment of photoaged hands. Dermatol Surg. 2018;44(1):68–74. https://doi.org/10.1097/DSS.0000000000001251
[16] Wu Y, Tian Y, Xu J, Zhong S, Wang R, Wu W. A randomized study showing improved skin quality and aesthetic appearance of dorsal hands after hyaluronic acid gel treatment in a Chinese population. J Cosmet Dermatol. 2020;19(7):1627–1635. https://doi.org/10.1111/jocd.13221
[17] Brandt FS, Cazzaniga A, Strangman N, Coleman J, Axford-Gatley R. Long-term effectiveness and safety of small gel particle hyaluronic acid for hand rejuvenation. Dermatol Surg. 2012;38(7 Pt 2):1128–1135. https://doi.org/10.1111/j.1524-4725.2011.02282.x
[18] Williams S, Tamburic S, Stensvik H, Weber M. Changes in skin physiology and clinical appearance after microdroplet placement of hyaluronic acid in aging hands. J Cosmet Dermatol. 2009;8(3):216–225. https://doi.org/10.1111/j.1473-2165.2009.00447.x
[19] Gubanova EI, Starovatova PA, Rodina MY. 12-month effects of stabilized hyaluronic acid gel compared with saline for rejuvenation of aging hands. J Drugs Dermatol. 2015;14(3):288–298.
[20] Agerup B, Berg P, Akermark C. Non-animal stabilized hyaluronic acid: a new formulation for the treatment of osteoarthritis. BioDrugs. 2005;19(1):23–30. https://doi.org/10.2165/00063030-200519010-00003
[21] Kumar V, Jain A, Atre S, et al. Non-surgical rhinoplasty using hyaluronic acid dermal fillers: a systematic review. J Cosmet Dermatol. 2021;20(8):2414–2424. https://doi.org/10.1111/jocd.14173
[22] Streker M, Reuther T, Krueger N, Kerscher M. Stabilized hyaluronic acid-based gel of non-animal origin for skin rejuvenation: face, hand, and décolletage. J Drugs Dermatol. 2013;12(9):990–994.
[23] Man J, Rao J, Goldman M. A double-blind, comparative study of nonanimal-stabilized hyaluronic acid versus human collagen for tissue augmentation of the dorsal hands. Dermatol Surg. 2008;34(8):1026–1031. https://doi.org/10.1111/j.1524-4725.2008.34201.x
[24] Yi KH, Winayanuwattikun W, Kim SY, et al. Skin boosters: definitions and varied classifications. Skin Res Technol. 2024;30(3):e13627. https://doi.org/10.1111/srt.13627
[25] Wang F, Garza LA, Kang S, et al. In vivo stimulation of de novo collagen production caused by cross-linked hyaluronic acid dermal filler injections in photodamaged human skin. Arch Dermatol. 2007;143(2):155–163. https://doi.org/10.1001/archderm.143.2.155
[26] Leclère FM, Vögelin E, Mordon S, et al. Nonanimal stabilized hyaluronic acid for tissue augmentation of the dorsal hands: a prospective study on 38 patients. Aesthetic Plast Surg. 2012;36(6):1367–1375. https://doi.org/10.1007/s00266-012-9974-2
[27] Cristel RT, Demesh D, Lombard R, et al. Blinded evaluation of hyaluronic acid hand filler injections and effects on first impressions. Dermatol Surg. 2021;47(5):637–640. https://doi.org/10.1097/DSS.0000000000002691
[28] Goldman MP, Moradi A, Gold MH, et al. Calcium hydroxylapatite dermal filler for treatment of dorsal hand volume loss: results from a 12-month, multicenter, randomized, blinded trial. Dermatol Surg. 2018;44(1):75–83. https://doi.org/10.1097/DSS.0000000000001203
[29] Kim JS, Lee W, Oh W, Park JA, Yang EJ. Identification of a suitable layer for injecting calcium hydroxylapatite fillers in the hands. J Plast Reconstr Aesthet Surg. 2021;74(4):866–873. https://doi.org/10.1016/j.bjps.2020.10.027
[30] Figueredo VO, Miot HA, Soares Dias J, Nunes G, Barros de Souza M, Bagatin E. Efficacy and safety of 2 injection techniques for hand biostimulatory treatment with diluted calcium hydroxylapatite. Dermatol Surg. 2020;46(Suppl 1):S54–S61. https://doi.org/10.1097/DSS.0000000000002334
[31] Moradi A, Ðaković R, Odena G. Aesthetic implantation of calcium hydroxylapatite does not interfere with radiological assessment of bones in the dorsum of the hands. Aesthet Surg J. 2023;43(6):696–703. https://doi.org/10.1093/asj/sjac344
[32] Lim A, Mulcahy A. Hand rejuvenation: combining dorsal veins foam sclerotherapy and calcium hydroxylapatite filler injections. Phlebology. 2017;32(6):397–402. https://doi.org/10.1177/0268355516655684
[33] Wu DC, Goldman MP. Randomized, double-blinded, sham-controlled, split-hand trial evaluating the safety and efficacy of triamcinolone acetate injection after calcium hydroxylapatite volume restoration of the dorsal hand. Dermatol Surg. 2018;44(4):534–541. https://doi.org/10.1097/DSS.0000000000001325
[34] Fakih-Gomez N, Kadouch J. Combining calcium hydroxylapatite and hyaluronic acid fillers for aesthetic indications: efficacy of an innovative hybrid filler. Aesthetic Plast Surg. 2022;46(1):373–381. https://doi.org/10.1007/s00266-021-02479-x
[35] Lemperle G, Knapp TR, Sadick NS, Lemperle SM. ArteFill permanent injectable for soft tissue augmentation: I. Mechanism of action and injection techniques. Aesthetic Plast Surg. 2010;34(3):264–272. https://doi.org/10.1007/s00266-009-9413-1
[36] Kühne U, Imhof M. Treatment of the ageing hand with dermal fillers. J Cutan Aesthet Surg. 2012;5(3):163–169. https://doi.org/10.4103/0974-2077.101369
[37] Hirche C, Senghaas A, Fischer S, Hollenbeck ST, Kremer T, Kneser U. Novel use of a flowable collagen-glycosaminoglycan matrix (Integra™ Flowable ound Matrix) combined with percutaneous cannula scar tissue release in treatment of post-burn malfunction of the hand – a preliminary 6 month follow-up. Burns. 2016;42(1):e1–e7. https://doi.org/10.1016/j.burns.2015.10.013
[38] Yeh LC, Goldberg DJ. Twelve-month prospective study of polymethylmethacrylate/collagen dermal filler for volume loss of the dorsal of hands. J Cosmet Dermatol. 2020;19(9):2259–2266. https://doi.org/10.1111/jocd.13445
[39] Peng GL. Platelet-rich plasma for skin rejuvenation: facts, fiction, and pearls for practice. Facial Plast Surg Clin North Am. 2019;27(3):405–411. https://doi.org/10.1016/j.fsc.2019.04.006
[40] Pincelli T, Zawawi S, Shapiro S, et al. A pilot, randomized, single-blind, controlled study evaluating the use of platelet rich plasma (PRP) for hand skin rejuvenation. Plast Reconstr Surg. 2024;154(4):727–734. https://doi.org/10.1097/PRS.0000000000011164
[41] Cabrera-Ramírez JO, Puebla-Mora AG, González-Ojeda A, et al. Platelet-rich plasma for the treatment of photodamage of the skin of the hands. Actas Dermosifiliogr. 2017;108(8):746–751. https://doi.org/10.1016/j.ad.2017.04.006
[42] Sasaki GH. A preliminary clinical trial comparing split treatments to the face and hand with autologous fat grafting and platelet-rich plasma (PRP): a 3D, IRB-approved study. Aesthet Surg J. 2019;39(6):675–686. https://doi.org/10.1093/asj/sjy254
[43] Christen MO. Collagen stimulators in body applications: a review focused on poly-L-lactic acid (PLLA). Clin Cosmet Investig Dermatol. 2022;15:997–1019. https://doi.org/10.2147/CCID.S359813
[44] Rendon MI, Cardona LM, Pinzon-Plazas M. Treatment of the aged hand with injectable poly-l-lactic acid. J Cosmet Laser Ther. 2010;12(6):284–287. https://doi.org/10.3109/14764172.2010.538410
[45] Jabbar A, Arruda S, Sadick N. Off face usage of poly-L-lactic acid for body rejuvenation. J Drugs Dermatol. 2017;16(5):489–494.
[46] Vleggaar D. Soft-tissue augmentation and the role of poly-L-lactic acid. Plast Reconstr Surg. 2006;118(3 Suppl):46S–54S. https://doi.org/10.1097/01.prs.0000234846.00139.74
[47] Lowe NJ, Ghanem AM. Volume restoration of hands with polycaprolactone by cannula delivery; a prospective single center consecutive case series evaluation. J Cosmet Laser Ther. 2020;22(2):55–59. https://doi.org/10.1080/14764172.2019.1711127
[48] Noland ME, Lalonde DH, Yee GJ, Rohrich RJ. Current uses of botulinum neurotoxins in plastic surgery. Plast Reconstr Surg. 2016;138(3):519e–530e. https://doi.org/10.1097/PRS.0000000000002480
[49] Kalliainen LK, O’Brien VH. Current uses of botulinum toxin A as an adjunct to hand therapy interventions of hand conditions. J Hand Ther. 2014;27(2):85–94; quiz 95. https://doi.org/10.1016/j.jht.2013.12.003
[50] Lungu C, Nmashie A, George MC, et al. Comparison of ultrasound and electrical stimulation guidance for onabotulinum toxin-A injections: a randomized crossover study. Mov Disord Clin Pract. 2022;9(8):1055–1061. https://doi.org/10.1002/mdc3.13546
[51] Gubanova EI, Starovatova PA. A prospective, comparative, evaluator-blind clinical study investigating efficacy and safety of two injection techniques with Radiesse(®) for the correction of skin changes in aging hands. J Cutan Aesthet Surg. 2015;8(3):147–152. https://doi.org/10.4103/0974-2077.167271
[52] Calomeni M, Bravo B, Schelke LW, et al. Precision of soft-tissue filler injections: an ultrasound-based verification study. Aesthet Surg J. 2023;43(3):353–361. https://doi.org/10.1093/asj/sjac272
[53] Khosravani N, Weber L, Patel R, Patel A. The 5-step filler hand rejuvenation: filling with hyaluronic acid. Plast Reconstr Surg Glob Open. 2019;7(1):e2073. https://doi.org/10.1097/GOX.0000000000002073
[54] Park JA, Lee SH, Hwang SJ, Koh KS, Song WC. Anatomic, histologic, and ultrasound analyses of the dorsum of the hand for volumetric rejuvenation. J Plast Reconstr Aesthet Surg. 2021;74(7):1615–1620. https://doi.org/10.1016/j.bjps.2020.11.017
[55] Lacarrubba F, Tedeschi A, Nardone B, Micali G. Mesotherapy for skin rejuvenation: assessment of the subepidermal low-echogenic band by ultrasound evaluation with cross-sectional B-mode scanning. Dermatol Ther. 2008;21(Suppl 3):S1–S5. https://doi.org/10.1111/j.1529-8019.2008.00234.x
[56] Tedeschi A, Lacarrubba F, Micali G. Mesotherapy with an intradermal hyaluronic acid formulation for skin rejuvenation: an intrapatient, placebo-controlled, long-term trial using high-frequency ultrasound. Aesthetic Plast Surg. 2015;39(1):129–133. https://doi.org/10.1007/s00266-014-0432-1
[57] Bertucci V, Solish N, Wong M, Howell M. Evaluation of the merz hand grading scale after calcium hydroxylapatite hand treatment. Dermatol Surg. 2015;41(Suppl 1):S389–S396. https://doi.org/10.1097/DSS.0000000000000546
[58] Cohen JL, Carruthers A, Jones DH, et al. A randomized, blinded study to validate the merz hand grading scale for use in live assessments. Dermatol Surg. 2015;41(Suppl 1):S384–S388. https://doi.org/10.1097/DSS.0000000000000553
[59] Lee JH, Choi YS, Park ES, et al. A novel photonumeric hand grading scale for hand rejuvenation. Arch Plast Surg. 2019;46(4):359–364. https://doi.org/10.5999/aps.2019.00521
[60] Almadori A, Speiser S, Ashby I, et al. Portable three-dimensional imaging to monitor small volume enhancement in face, vulva, and hand: a comparative study. J Plast Reconstr Aesthet Surg. 2022;75(9):3574–3585. https://doi.org/10.1016/j.bjps.2022.04.042
[61] Cuzalina A, Guerrero AV. Complications in fat grafting. Atlas Oral Maxillofac Surg Clin North Am. 2018;26(1):77–80. https://doi.org/10.1016/j.cxom.2017.11.003
[62] Swift A, Green JB, Hernandez CA, et al. Tips and tricks for facial toxin injections with illustrated anatomy. Plast Reconstr Surg. 2022;149(2):303e–312e. https://doi.org/10.1097/PRS.0000000000008708
[63] Hong SO. Cosmetic treatment using botulinum toxin in the oral and maxillofacial area: a narrative review of esthetic techniques. Toxins (Basel). 2023;15(2):82. https://doi.org/10.3390/toxins15020082
[64] Zargaran D, Zoller F, Zargaran A, et al. Complications of cosmetic botulinum toxin A injections to the upper face: a systematic review and meta-analysis. Aesthet Surg J. 2022;42(5):NP327–NP336. https://doi.org/10.1093/asj/sjac036
[65] Senet P, Maillard H, Diot E, et al. Efficacy and safety of botulinum toxin in adults with Raynaud’s phenomenon secondary to systemic sclerosis: a multicenter, randomized, double-blind, placebo-controlled study. Arthritis Rheumatol. 2023;75(3):459–467. https://doi.org/10.1002/art.42342
[66] Glaser DA, Galperin TA. Botulinum toxin for hyperhidrosis of areas other than the axillae and palms/soles. Dermatol Clin. 2014;32(4):517–525. https://doi.org/10.1016/j.det.2014.06.001
[67] Sussman J. Musician’s dystonia. Pract Neurol. 2015;15(4):317–322. https://doi.org/10.1136/practneurol-2015-001148
[68] Goldman JG. Writer’s cramp. Toxicon. 2015;107(Pt A):98–104. https://doi.org/10.1016/j.toxicon.2015.09.024
[69] Newsome HA, Chi JJ. Mastering midface injections. Clin Plast Surg. 2023;50(3):437–446. https://doi.org/10.1016/j.cps.2022.12.008
[70] Buzalaf M, Levy FM. Autologous platelet concentrates for facial rejuvenation. J Appl Oral Sci. 2022;30:e20220020. https://doi.org/10.1590/1678-7757-2022-0020
[71] Li G, Wang H. Novel applications of concentrated growth factors in facial rejuvenation and plastic surgery. Facial Plast Surg. 2024;40(1):112–119. https://doi.org/10.1055/a-1987-3459
[72] Crowley JS, Liu A, Dobke M. Regenerative and stem cell-based techniques for facial rejuvenation. Exp Biol Med (Maywood). 2021;246(16):1829–1837. https://doi.org/10.1177/15353702211020701
[73] Breithaupt A, Fitzgerald R. Collagen stimulators: poly-L-lactic acid and calcium hydroxyl apatite. Facial Plast Surg Clin North Am. 2015;23(4):459–469. https://doi.org/10.1016/j.fsc.2015.07.007
[74] de Melo F, Nicolau P, Piovano L, et al. Recommendations for volume augmentation and rejuvenation of the face and hands with the new generation polycaprolactone-based collagen stimulator (Ellansé(®)). Clin Cosmet Investig Dermatol. 2017;10:431–440. https://doi.org/10.2147/CCID.S145195