ORIGINAL RESEARCH ARTICLE
Clinical outcomes of isolated ulnar shortening osteotomy for ulnar impaction syndrome with concomitant distal radioulnar joint instability
Xing Gaoa†, Aozhengzheng Donga,c†, Jingxin Lia, Changliang Maa, Wencui Lib, Jianquan Liub, Zhiqin Dengb and Zhe Zhaob,d
aMedical School, Shenzhen University, Shenzhen, Guangdong 518028, China; bDepartment of Hand and Foot Surgery, Shenzhen Second People’s Hospital (The First Hospital Affiliated to Shenzhen University), Shenzhen, Guangdong 518028, China; cBeijing Jishuitan Hospital, Capital Medical University, Beijing 100000, China; dDepartment of Sports Medicine, The First Affiliated Hospital, Guangdong Provincial Key Laboratory of Speed Capability, The Guangzhou Key Laboratory of Precision Orthopedics and Regenerative Medicine, Jinan University, Guangzhou 510630, China
ABSTRACT
Background: This study aimed to evaluate the clinical outcomes and changes in distal radioulnar joint (DRUJ) stability in patients with ulnar impaction syndrome (UIS) combined with DRUJ instability, treated with ulnar shortening osteotomy (USO) without concomitant triangular fibrocartilage complex (TFCC) repair.
Materials and methods: Between November 2017 and December 2024, a total of 16 patients (7 males, 9 females; mean age, 40 ± 12 years) underwent USO combined with wrist arthroscopy, followed by structured rehabilitation and regular follow-up. Clinical outcomes were assessed using ulnar variance, the Ballottement test, visual analog scale (VAS) for pain, Disabilities of the Arm, Shoulder, and Hand (DASH) score, modified Mayo wrist score, Patient-Rated Wrist Evaluation (PRWE), grip strength, and wrist range of motion. Preoperatively, all patients had positive Ballottement tests, and TFCC injuries were confirmed by arthroscopy.
Results: At the final follow-up (mean, 31 months), ulnar variance was significantly reduced, and VAS, DASH, modified Mayo wrist score, PRWE, and grip strength all showed marked improvement. DRUJ stability was restored in all patients, with the Ballottement test converting to negative.
Conclusions: These findings suggest that isolated USO effectively treats UIS with concurrent DRUJ instability and achieves satisfactory clinical outcomes without the need for simultaneous TFCC repair.
Type of study/level of evidence: Therapeutic, Level IV.
KEYWORDS: Ulnar shortening osteotomy; ulnar impaction syndrome; distal radioulnar joint instability
Citation: Journal of Plastic Surgery and Hand Surgery 2025; 61: 44–50. DOI: https://doi.org/10.2340/jphs.v61.45517.
Copyright: © 2026 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 25 September 2025; Accepted: 13 January 2026; Published: 24 March 2026.
CONTACT: Zhe Zhao 2210244055@email.szu.edu.cn Department of Hand and Foot Surgery, Shenzhen Second People’s Hospital (The First Hospital Affiliated to Shenzhen University), Shenzhen, Guangdong 518028, China
†These authors contributed equally.
Competing interests and funding: The authors declare that they have no conflict of interest.
The study was supported by the Key Medical Discipline Construction Fund of Shenzhen (SZXK025), the ‘Sanming’ Project of Shenzhen Health System (SZSM202311008), and the Internal Clinical Research Fund of High-level Hospital Development Program (2023yjlcyj009).
Introduction
Ulnar impaction syndrome (UIS), first described by Milch in 1941, is one of the primary causes of ulnar-sided wrist pain [1–3]. Patients typically present with deep, aching pain on the ulnar side of the wrist, reduced grip strength, and symptom aggravation during forearm rotation or axial loading, often accompanied by localized tenderness and restricted motion. UIS is commonly seen in individuals with repetitive wrist use and positive ulnar variance, a condition that increases ulnocarpal loading. It has been reported that a 2.5 mm increase in ulnar length can raise the ulnocarpal load to as much as 42% [4, 5]. Excessive ulnar length may lead to chronic impaction of the triangular fibrocartilage complex (TFCC), lunate, and triquetrum, resulting in TFCC degeneration and perforation, cartilage softening, bone marrow edema, cyst formation, and even osteonecrosis [6]. Repetitive ulnocarpal impaction and prolonged overloading on the ulnar side of the wrist can cause TFCC tears and degeneration, subsequently leading to distal radioulnar joint (DRUJ) instability [7]. Thus, DRUJ instability is commonly observed in patients with UIS.
Ulnar shortening osteotomy (USO) is the most widely used surgical treatment for UIS, aiming to correct ulnar positive variance and relieve ulnocarpal impingement [8]. In patients with concurrent DRUJ instability, many authors recommend that if instability persists intraoperatively after USO, TFCC repair should be performed simultaneously. Otherwise, symptoms such as ulnar-sided pain and weakness may persist postoperatively [7, 9, 10]. However, some scholars argue that USO alone may yield satisfactory outcomes for UIS [11]. Seo retrospectively reviewed 31 patients with chronic DRUJ instability who underwent USO and found that both USO combined with arthroscopic debridement and USO combined with TFCC repair produced satisfactory outcomes in cases of unstable TFCC tears with ulnar positive variance [12].
Currently, there is no consensus on whether TFCC repair should routinely be combined with USO in patients with UIS and DRUJ instability. Although TFCC repair may theoretically enhance DRUJ stability, it increases operative time and complexity, and typically requires 6 weeks of postoperative immobilization. This may lead to complications such as sensory disturbances and joint stiffness. Previous studies have shown that USO alters the congruency pattern of the DRUJ, leading to increased joint pressure and contact area, and potentially contributing to the development of osteoarthritic changes over time. These biomechanical adaptations may enhance the bony stability of the DRUJ, thereby promoting the restoration of stability in previously unstable joints [4, 13–15]. However, such changes may also predispose to joint degeneration. Given the limited number of relevant studies, the optimal surgical strategy for UIS combined with DRUJ instability remains uncertain. This study aims to evaluate the clinical efficacy of USO alone in this patient population, with the goal of providing reference data for future surgical decision-making.
Methods
Inclusion and exclusion criteria
Inclusion criteria
The inclusion criteria were as follows: (1) patients diagnosed with UIS; (2) concomitant diagnosis of DRUJ instability; (3) persistent symptoms after at least 3 months of conservative treatment, followed by USO combined with wrist arthroscopy performed at our institution; and (4) positive arthroscopic hook test and positive Ballottement test indicating DRUJ instability after USO.
Exclusion criteria
The exclusion criteria were as follows: (1) history of wrist fractures; (2) presence of severe systemic diseases rendering the patient unfit for surgery or anesthesia; (3) incomplete follow-up data; and (4) negative arthroscopic hook test or negative Ballottement test indicating DRUJ stability after USO.
Study design and patients
This retrospective study was approved by the institutional ethics committee. A total of 28 patients diagnosed with UIS combined with distal DRUJ instability, who underwent wrist arthroscopy and oblique ulnar shortening osteotomy (OUSO) between November 2017 and December 2024, were initially identified from the institutional clinical database. The diagnostic criteria for UIS were as follows: (1) ulnar-sided wrist pain with limited motion, aggravated by rotation, ulnar deviation, or axial loading; (2) positive ulnar stress test; (3) positive ulnar variance >2 mm on standard wrist radiographs; and (4) MRI evidence of signal alterations in the lunate, triquetrum, or TFCC [10]. A diagnosis of DRUJ instability was confirmed when the following were present: a positive ulnar fovea sign, a positive Ballottement test, MRI showing deep TFCC ligament injury, and a positive hook test on wrist arthroscopy [16].
Based on inclusion and exclusion criteria, 16 patients were included in the final analysis; 12 were excluded due to incomplete follow-up or negative intraoperative hook/Ballottement tests after osteotomy. The cohort comprised seven men and nine women, with a mean age of 40 years (range: 22–55). The right wrist was involved in 13 cases and the left in 3; all cases were unilateral. Three patients reported prior trauma, while 13 had no identifiable cause. All presented with ulnar-sided wrist pain and functional limitations affecting daily life and work. Preoperative imaging included posteroanterior/lateral radiographs and MRI. Ulnar variance was measured using the vertical line method; all cases showed positive variance (mean: 3.6 mm; range: 2.0–5.7 mm). Tolat classification showed 10 wrists as type 1, 2 as type 2, and 4 as type 3. MRI revealed TFCC injuries in all patients: cystic changes in the lunate in 2, triquetrum in 5, and both bones in 5; four patients also had bone marrow edema. On examination, all patients had positive ulnar stress and Ballottement tests, consistent with DRUJ instability (Table 1).
Surgical technique
Wrist arthroscopy
Wrist arthroscopy was performed using a traction tower, with finger traps applied to two or three fingers of the affected hand. After marking Lister’s tubercle, standard portals (3–4, 6R, 4–5, 6U) were established. Saline (5–10 mL) was injected via the 3–4 portal for joint distension. The arthroscope was introduced through this portal to assess the radioscapholunate (RSL) and radiolunate (RL) ligaments. Articular cartilage of the lunate and triquetrum was examined for wear, degeneration, and cysts. The hook test evaluated TFCC deep fiber integrity; radial translation under ulnar traction indicated a positive result [16]. Synovial proliferation was debrided using a shaver or radiofrequency device via 4–5 and 6R portals. In cases of lunotriquetral ligament injury or cartilage softening, unstable tissue was removed and thermal shrinkage applied. Bone cysts were treated with microfracture or bone grafting. Central TFCC tears were debrided and thermally stabilized; deep insertions were not repaired.
Oblique ulnar shortening osteotomy
With the patient supine and a tourniquet applied to the upper arm, a longitudinal incision was made along the ulnar aspect of the distal forearm, starting at the ulnar neck. The dorsal ulna was exposed subperiosteally. A seven-hole dynamic compression plate (DCP) was temporarily positioned, with its distal end spanning from the ulnar neck to the sigmoid notch. The distal-most screw was inserted to establish plate position. An osteotomy site was marked between the third and fourth holes based on the preoperative ulnar variance. After removing the plate, osteotomy ends were marked with cautery to guide reduction. An oblique osteotomy was performed using a sagittal saw, and the resected segment was removed. The ulna was reduced along the marked axis, avoiding rotational malalignment. The DCP plate was reattached, and remaining screws were placed under dynamic compression to achieve stable fixation. Fluoroscopic imaging confirmed correction of ulnar variance and alignment (Figure 1). The incision was closed in layers (Figure 2).
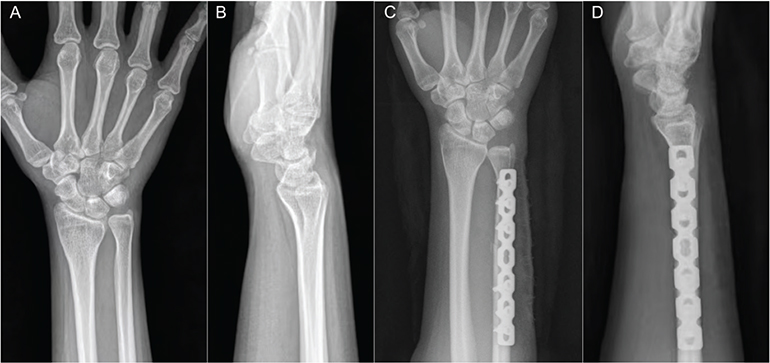
Figure 1. A patient with ulnar impaction syndrome treated with oblique ulnar shortening osteotomy. (A) Preoperative posteroanterior and lateral radiographs of the right wrist. (B) Postoperative posteroanterior and lateral radiographs of the right wrist.
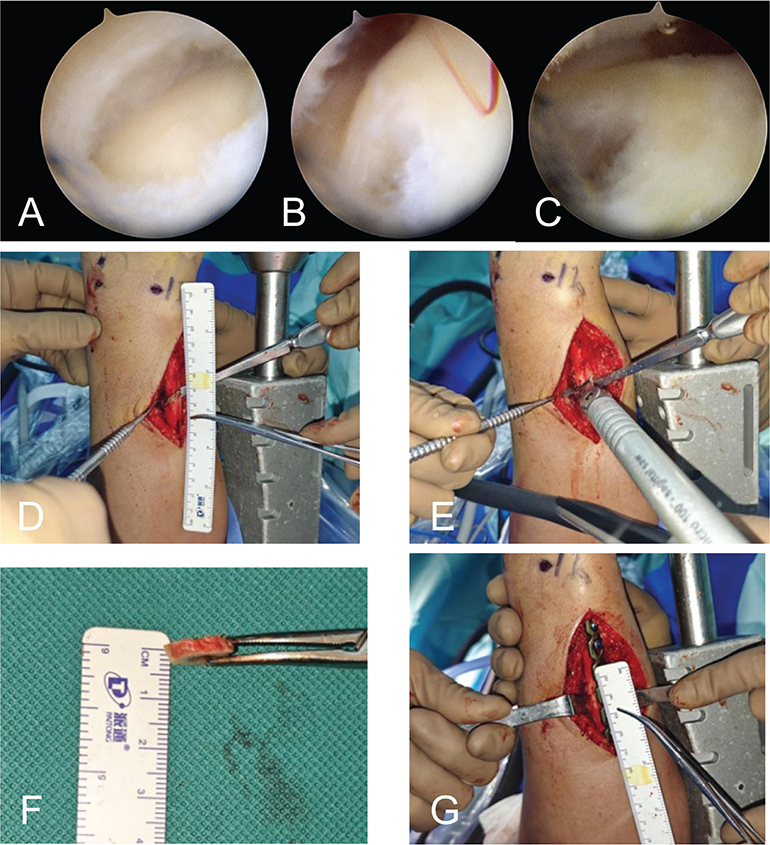
Figure 2. A patient with ulnar impaction syndrome treated with oblique ulnar shortening osteotomy. (A) Preoperative posteroanterior radiograph of the right wrist. (B) Preoperative lateral radiograph of the right wrist. (C) Postoperative posteroanterior radiograph of the right wrist. (D) Postoperative lateral radiograph of the right wrist.
Post-osteotomy arthroscopic and stability reassessment
Following osteotomy, the 3–4 portal was re-entered to perform a second arthroscopic hook test for deep TFCC assessment. Finally, under anesthesia, a bilateral Ballottement test was performed to evaluate postoperative DRUJ stability.
Postoperative management
All 16 patients underwent OUSO; among them, 11 also had arthroscopic debridement, and 2 underwent microfracture for lunate cysts. Wrist motion (rotation and flexion–extension) began on postoperative day 2, with strenuous activity restricted for 3 months. One patient with a large triquetral cyst received bone grafting and was immobilized in a short-arm cast for 4 weeks, followed by range-of-motion exercises. Two patients with steep Tolat type 3 sigmoid notches underwent concurrent notchplasty, followed by 3 weeks of long-arm casting, then 3 weeks of short-arm casting. Wrist mobilization began at 6 weeks.
All patients were followed up at 3 weeks, 6 weeks, 3 months, 6 months, and 1 year after surgery, and annually thereafter. Functional outcomes were evaluated at the final follow-up using the visual analog scale (VAS) for pain, Patient-Rated Wrist Evaluation (PRWE), Disabilities of the Arm, Shoulder, and Hand (DASH) score, wrist range of motion, and grip strength.
Clinical and radiographic evaluation
All clinical examinations – grip strength, wrist range of motion, and Ballottement test – were conducted by the same independent physician. DRUJ instability was defined as ≥1 cm of ulnar displacement relative to the contralateral side, with absent end-range resistance on Ballottement test [17].
Patient-reported outcomes included the DASH, PRWE, modified Mayo wrist score, and VAS pain score [18], measured preoperatively and at the final follow-up.
Standard posteroanterior wrist radiographs were obtained at baseline and each follow-up. Ulnar variance was measured using the vertical line method. Radiographs were also assessed for osteotomy healing and degenerative changes in the carpus or DRUJ.
Statistical analysis
Statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) statistical software (version 24.0; IBM Corp., Armonk, NY, USA). Continuous variables were first tested for normality using the Shapiro–Wilk test (p > 0.10 indicating normal distribution). Normally distributed data were presented as mean ± SD (standard deviation) and analyzed with paired t-tests; non-normally distributed data were expressed as median (Q1, Q3) and analyzed using the Wilcoxon signed-rank test. A two-tailed significance level of α = 0.05 was applied, with p < 0.05 indicating statistical significance.
Results
Arthroscopy confirmed TFCC ulnar tears in all 16 patients, all with positive hook tests. TFCC central perforation was found in 12 cases and central wear in 4. Cartilage wear of the lunate and/or triquetrum was observed in 14 cases, including one lunotriquetral ligament tear, three lunate cysts, and one large triquetral cyst; two cases showed no cartilage damage. Debridement and thermal shrinkage were applied to perforated and worn regions. Three lunate cysts underwent microfracture, and one triquetral cyst was grafted. According to the Palmer classification: 1B+2A (n = 2), 1B+2B (n = 2), 1B+2C (n = 12). All 16 patients underwent OUSO, and two additionally received sigmoidal notchplasty for Tolat type-3 sigmoid notches. Post-osteotomy arthroscopy showed persistent positive hook tests, and intraoperative Ballottement tests remained positive.
Follow-up and functional recovery
All patients completed follow-up (mean 31 months, range 6 months to 7 years). By about 5 months post-op, all returned to their original jobs. Plate removal was undertaken in five patients at 12 months due to implant irritation. All osteotomy sites achieved bony union (mean healing time 2.9 months). Seven patients resumed daily activities without discomfort; seven reported stiffness only at extremes of wrist motion. One patient experienced rotational pain, which was managed effectively with nonsteroidal anti-inflammatory drugs (NSAIDs).
Wrist mobility and grip strength
At final follow-up, there were no statistically significant differences in forearm pronation and supination compared to preoperative values. Pronation was 70.9° ± 4.9° preoperatively and 70.5° ± 5.0° postoperatively (p = 0.46); supination improved from 80.9° ± 4.9° to 88.6° ± 5.2° (p = 0.27). Similarly, no significant changes were observed in wrist extension or flexion. Extension measured 60.2° ± 5.6° preoperatively versus 59.8° ± 5.6° postoperatively (p = 0.27), while wrist flexion increased from a median of 71.5° (63.6°, 82.5°) to 76.9° (65.8°, 85.1°) (p = 0.36).
Grip strength improved significantly from 83 ± 9% to 90 ± 8% of the contralateral side (p = 0.02), indicating good recovery of wrist power and function (Table 3).
Patient-reported outcomes and clinical examination
Pain and function scores improved significantly: VAS from 5 (3, 5.75) to 0.5 (0, 1) (p < 0.001); DASH from 23.3 ± 10.5 to 3.0 ± 3.8 (p < 0.001); modified Mayo from 75.9 ± 6.8 to 93.4 ± 5.0 (p < 0.001); PRWE from 34.3 ± 15.2 to 4.7 ± 6.1 (p < 0.001) (Table 2). Ballottement tests at final follow-up confirmed DRUJ stability in all patients.
| Variable | Preoperative | Final postoperative follow-up | P-value | |
| VAS pain [M (Q1, Q3)] | 5 (3.25, 5.75) | 0.5 (0, 1) | <0.001* | |
| DASH score (SD) | 23.3 ± 10.5 | 3.0 ± 3.8 | <0.001* | |
| Mayo Wrist Score (SD) | 75.9 ± 6.8 | 93.4 ± 5.0 | <0.001* | |
| PRWE score (SD) | 34.3 ± 15.2 | 4.7 ± 6.1 | <0.001* | |
| If the paired differences did not follow a normal distribution, the Wilcoxon signed-rank test for paired data was used, and the results were expressed as median (Q1, Q3). If the paired differences followed a normal distribution, the paired t-test was used, and the results were expressed as mean ± standard deviation. VAS: visual analog scale; DASH: Disabilities of the Arm, Shoulder and Hand; PRWE: Patient-Rated Wrist Evaluation; SD: standard deviation. *Indicates a statistically significant difference. |
||||
Radiographic findings
Ulnar variance decreased significantly from 3.6 ± 1.1 mm to 0.6 ± 1.0 mm postoperatively (p < 0.001) (Table 3). All osteotomies healed without complications (mean 2.9 months). Radiographic signs of arthritis developed in 5 patients (mean 27 months post-op).
| Variable | Preoperative | Final postoperative follow-up | P-value | |
| Pronation (SD) | 70.9 ± 4.9 | 70.5 ± 5.0 | 0.46 | |
| Supination (SD) | 89.5 ± 4.9 | 88.6 ± 5.2 | 0.27 | |
| Extension (SD) | 60.2 ± 5.6 | 59.8 ± 5.6 | 0.27 | |
| Flexion [M (Q1, Q3)] | 71.5 (63.6, 82.5) | 76.9 (65.8, 85.1) | 0.36 | |
| Ulnar variance (SD) | 3.6 ± 1.1 | 0.6 ± 1.0 | <0.001* | |
| Ballottement (n) | 16(+)/0(–) | 0(+)/16(–) | ||
| Grip Strength (SD) | 83 ± 9 | 90 ± 8 | 0.02* | |
| If the paired differences did not follow a normal distribution, the Wilcoxon signed-rank test for paired data was used, and the results were expressed as median (Q1, Q3). If the paired differences followed a normal distribution, the paired t-test was used, and the results were expressed as mean ± standard deviation. SD: standard deviation. *Indicates a statistically significant difference. |
||||
Complications
All incisions healed primarily without infection; no delayed or non-union occurred. Five patients (31%) experienced implant irritation at 12 months, which resolved after plate removal. Degenerative changes in DRUJ were observed radiographically in five patients (mean onset at 27 months); only one patient had rotational pain attributed to radiographically evident DRUJ arthritis at 9 months postoperatively, which was managed conservatively. Tolat classification in these five cases: type 1 (vertical) n = 1 (20%), type 2 (inclined) n = 1 (20%), type 3 (reverse) n = 3 (60%).
Discussion
In this study, 16 patients with UIS and DRUJ instability – who continued to show intraoperative DRUJ instability after USO – underwent oblique USO without TFCC repair. At a mean follow-up of 31 months, all patients showed significant improvements across clinical outcomes. Grip strength increased from 83 ± 9% to 90 ± 8% of the contralateral side, and DRUJ stability was restored in all cases. Functionally, eight patients reported no discomfort, seven experienced mild stiffness at end range, and one had rotational pain.
Oblique ulnar shortening osteotomy effectively treats UIS
USO is the standard surgical approach for UIS, aiming to reduce axial load on the ulnocarpal joint. Biomechanical studies have shown that shortening the ulna by 2.5 mm can decrease the joint load from 42 to 18% [19]. Compared with traditional transverse osteotomy, the oblique technique offers a larger bony contact surface and greater mechanical stability, promoting faster union and enabling earlier rehabilitation. In 2024, Miyashima reported that oblique USO yielded superior radiographic and clinical outcomes, including faster healing and greater pain relief, compared with the transverse approach [20]. Based on these advantages, oblique USO was selected in our cohort.
Controversy over the need for TFCC repair in UIS with concomitant DRUJ instability
Chan reported a 1.6% incidence of persistent ulnar wrist pain postoperatively [19]. Koh in a wrist arthroscopic assessment of 50 UIS patients, found that about half had TFCC tears or arthritis, suggesting these lesions may underlie residual symptoms [21]. Based on such findings, some authors recommend TFCC repair in UIS patients with DRUJ instability to improve outcomes [7]. In 2016, Seo compared outcomes of USO combined with either arthroscopic debridement or TFCC repair. At a minimum 24-month follow-up, both approaches yielded similarly satisfactory clinical results [12]. In our study, all patients underwent isolated USO without TFCC repair and achieved restored DRUJ stability and good clinical outcomes, consistent with Seo’s findings. Therefore, we hypothesize that postoperative ulnar-sided pain reported in some studies may result more from synovitis, DRUJ arthritis, or other causes, rather than persistent instability.
USO alone can restore DRUJ stability
USO may restore DRUJ stability by increasing the tension of stabilizing structures such as the TFCC, joint capsule, and the distal oblique bundle (DOB) [12]. In a cadaveric study, Sayuri demonstrated that even 1 mm of ulnar shortening significantly improved DRUJ stability [22]. Surgical procedures or injuries that alter DRUJ congruency – such as USO or distal radius fractures – can result in increased joint stiffness and reduced flexibility, but also improved stability. One study reported a 35.3% incidence of wrist stiffness following distal radius fracture fixation [23]. In our clinical practice, we have similarly observed that patients often present with limited forearm rotation in the early postoperative period, which improves with structured rehabilitation. However, many continue to report a sensation of stiffness at the extremes of motion, and Ballottement testing in these cases frequently reveals enhanced DRUJ stability compared to the contralateral side. On the other hand, we postulate that ulnar shortening may increase the distance between the torn deep fibers of the TFCC and their insertion at the fovea, potentially impeding natural healing and limiting the benefit of concurrent TFCC repair. Therefore, adding TFCC repair may not enhance DRUJ stability beyond what USO alone achieves.
Increased contact pressure and area promote DRUJ stability post-USO
Moritomo reported that USO increases the tension of the DOB, thereby enhancing DRUJ stability [22]. However, in our cohort, intraoperative Ballottement testing still indicated DRUJ instability immediately following osteotomy. Previous studies have identified a thickened fibrous structure within the distal interosseous membrane in a subset of individuals, defined by Noda as the DOB. Hohenberger’s anatomical study of 185 cadaveric forearms revealed that the DOB is present in only 29% of specimens [23], suggesting that this specialized structure may contribute significantly to enhanced DRUJ stability following USO. Notably, our study specifically enrolled patients who demonstrated persistent intraoperative DRUJ instability. Nonetheless, by the final follow-up, all patients exhibited DRUJ stability on physical examination. Previous studies have demonstrated that USO can induce DRUJ remodelling, increasing joint contact area and pressure. Nishiwaki et al reported that peak DRUJ contact pressure is positively correlated with the amount of ulnar shortening [4, 13]. In a 2023 finite element analysis, Jiang Hong demonstrated that shortening the ulna by 2–5 mm increased maximum DRUJ stress from 2.15 MPa to 5.76 MPa, with the effect more pronounced under load-bearing conditions [15]. Additional findings by Hyun and Nishiwaki indicated that USO reduced dorsal subluxation of the ulnar head and increased DRUJ contact area [4, 14]. We hypothesize that this recongruency effect and the resultant increase in articular contact area and pressure may represent a key mechanism contributing to postoperative DRUJ stabilization [24, 25]. In some patients, joint stiffness during extreme motion was observed, potentially attributable to this increased pressure and reduced joint flexibility. Furthermore, the elevated joint pressure may predispose to degenerative changes. In our series, five patients (31%) showed radiographic signs of DRUJ osteoarthritis at a mean of 27 months postoperatively, consistent with findings from Baek [14]. In five patients, radiographs revealed osteophyte formation around the DRUJ, which may have further contributed to joint stability.
TFCC repair may compromise postoperative mobility
Some authors support TFCC repair in UIS patients with DRUJ instability, but our findings suggest it may not be routinely necessary. In this cohort, all patients who underwent USO without TFCC repair achieved significant pain relief, functional improvement, and restored DRUJ stability at final follow-up. These results challenge the necessity of combined TFCC repair and support further investigation. TFCC repair may result in persistent wrist pain, sensory disturbances, and limited range of motion. It also prolongs surgery and necessitates extended immobilization, increasing the risk of stiffness and reducing patient satisfaction. USO can induce DRUJ remodeling, making early mobilization essential to preserve joint mobility.
This study has limitations. It is a retrospective case series with a small sample size, which may introduce selection bias. In addition, DRUJ stability was primarily assessed using the Ballottement test, a subjective clinical measure. The absence of a control group in this case series limited comparisons to preoperative and postoperative conditions only. Future studies with objective imaging or biomechanical evaluation are needed to validate these findings.
Conclusion
Our results indicate that USO alone, combined with early rehabilitation, can restore DRUJ stability and provide favorable long-term outcomes. We therefore propose USO as a primary surgical strategy for UIS patients with DRUJ instability.
Declarations
Ethical approval
The study was approved by the Ethics Committee of Shenzhen Second People’s Hospital (Approval No. 2026-044-01PJ).
Informed consent
Informed consent was obtained from all individual participants included in the study.
Author contribution
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Jingxin Li, Wencui Li, Jianquan Liu, Changliang Ma, and Zhiqin Deng. The first draft of the manuscript was written by Xing Gao and Aozhengzheng Dong, and all authors, including Zhe Zhao, commented on previous versions of the manuscript. All authors read and approved the final manuscript.
References
[1] Mwaturura T, Daneshvar P, Pike J, et al. Clinical and radiographic correlates for the treatment of ulnocarpal impaction. J Wrist Surg. 2019;8(3):192–197. https://doi.org/10.1055/s-0038-1677534
[2] Stockton DJ, Pelletier ME, Pike JM. Operative treatment of ulnar impaction syndrome: a systematic review. J Hand Surg Eur Vol. 2015;40(5):470–476. https://doi.org/10.1177/1753193414541749
[3] Hontani K, Matsui Y, Kawamura D, et al. Stress distribution pattern in the distal radioulnar joint before and after ulnar shortening osteotomy in patients with ulnar impaction syndrome. Sci Rep Uk. 2021;11(1):17891. https://doi.org/10.1038/s41598-021-97398-x
[4] Nishiwaki M, Nakamura T, Nagura T, et al. Ulnar-shortening effect on distal radioulnar joint pressure: a biomechanical study. J Hand Surg Am. 2008;33(2):198–205. https://doi.org/10.1016/j.jhsa.2007.11.024
[5] Sachar K. Ulnar-sided wrist pain: evaluation and treatment of triangular fibrocartilage complex tears, ulnocarpal impaction syndrome, and lunotriquetral ligament tears. J Hand Surg Am. 2012;37(7):1489–1500. https://doi.org/10.1016/j.jhsa.2012.04.036
[6] Pirolo JM, Yao J. Minimally invasive approaches to ulnar-sided wrist disorders. Hand Clin. 2014;30(1):77–89. https://doi.org/10.1016/j.hcl.2013.09.001
[7] Im JH, Lee JY, Kang HV. The combined procedure of ulnar metaphyseal shortening osteotomy with triangular fibrocartilage complex foveal knotless repair. J Hand Surg Am. 2021;46(9):821–822. https://doi.org/10.1016/j.jhsa.2021.01.021
[8] Shi H, Huang Y, Shen Y, et al. Arthroscopic wafer procedure versus ulnar shortening osteotomy for ulnar impaction syndrome: a systematic review and meta-analysis. J Orthop Surg Res. 2024;19(1):149. https://doi.org/10.1186/s13018-024-04611-4
[9] Shaer SA, van der Palen J, Teunissen J, et al. An alternative treatment for degenerative triangular fibrocartilage complex injuries with distal radioulnar joint instability: first experience with 48 patients. J Hand Surg Eur Vol. 2024;49(2):240–249. https://doi.org/10.1177/17531934231197942
[10] Lu C, Wang P, Zhang L, et al. Clinical study of wrist arthroscopy combined with oblique ulnar shortening osteotomy in the treatment of ulnar impaction syndrome. Orthop Surg. 2022;14(11):2947–2954. https://doi.org/10.1111/os.13428
[11] Kim BS, Song HS. A comparison of ulnar shortening osteotomy alone versus combined arthroscopic triangular fibrocartilage complex debridement and ulnar shortening osteotomy for ulnar impaction syndrome. Clin Orthop Surg. 2011;3(3): 184–190. https://doi.org/10.4055/cios.2011.3.3.184
[12] Seo JB, Kim JP, Yi HS, et al. The outcomes of arthroscopic repair versus debridement for chronic unstable triangular fibrocartilage complex tears in patients undergoing ulnar-shortening osteotomy. J Hand Surg Am. 2016;41(5):615–623. https://doi.org/10.1016/j.jhsa.2016.02.009
[13] de Runz A, Pauchard N, Sorin T, et al. Ulna-shortening osteotomy: outcome and repercussion of the distal radioulnar joint osteoarthritis. Plast Reconstr Surg. 2016;137(1):175–184. https://doi.org/10.1097/PRS.0000000000001870
[14] Baek GH, Lee HJ, Gong HS, et al. Long-term outcomes of ulnar shortening osteotomy for idiopathic ulnar impaction syndrome: at least 5-years follow-up. Clin Orthop Surg. 2011;3(4):295–301. https://doi.org/10.4055/cios.2011.3.4.295
[15] Hong J, Jiyang T, Xiaodong F, et al. Finite element analysis of altered contact stress in the distal radioulnar joint following shortening osteotomy of the ulnar diaphyseal metaphysis. Chinese J Hand Surg. 2023;39(5):431–436.
[16] Atzei A, Luchetti R, Carletti D, et al. The hook test is more accurate than the trampoline test to detect foveal tears of the triangular fibrocartilage complex of the wrist. Arthroscopy. 2021;37(6):1800–1807. https://doi.org/10.1016/j.arthro.2021.03.005
[17] Jens S, Luijkx T, Smithuis FF, et al. Diagnostic modalities for distal radioulnar joint. J Hand Surg Eur Vol. 2017;42(4):395–404. https://doi.org/10.1177/1753193416683876
[18] Cho JY, Lee SW, Kim DH, et al. Prognostic factors for clinical outcomes after arthroscopic treatment of traumatic central tears of the triangular fibrocartilage complex. Bone Joint J. 2024;106-B(4): 380–386. https://doi.org/10.1302/0301-620X.106B4.BJJ-2023-0642.R3
[19] Chan SK, Singh T, Pinder R, et al. Ulnar shortening osteotomy: are complications under reported? J Hand Microsurg. 2015;7(2):276–282. https://doi.org/10.1007/s12593-015-0201-7
[20] Miyashima Y, Uemura T, Okada M, et al. Comparison of dynamic compression plate systems with oblique osteotomy and locking plate fixation versus transverse osteotomy and non-locking plate fixation for ulnar shortening osteotomy. J Orthop Sci. 2025;30(5):798–804. https://doi.org/10.1016/j.jos.2024.11.007
[21] Koh KH, Lee HL, Chang YS, et al. Arthroscopy during ulnar shortening for idiopathic ulnar impaction syndrome. Orthopedics. 2013;36(12):e1495–e1500. https://doi.org/10.3928/01477447-20131120-12
[22] Arimitsu S, Moritomo H, Kitamura T, et al. The stabilizing effect of the distal interosseous membrane on the distal radioulnar joint in an ulnar shortening procedure: a biomechanical study. J Bone Joint Surg Am. 2011;93(21):2022–2030. https://doi.org/10.2106/JBJS.J.00411
[23] Kong L, Zhai Y, Zhang Z, et al. Radiocarpal joint stiffness following surgical treatment for distal radius fractures: the incidence and associated factors. J Orthop Surg Res. 2020;15(1):313. https://doi.org/10.1186/s13018-020-01857-6
[24] Tatebe M, Horii E, Nakao E, et al. Repair of the triangular fibrocartilage complex after ulnar-shortening osteotomy: second-look arthroscopy. J Hand Surg Am. 2007;32(4):445–449. https://doi.org/10.1016/j.jhsa.2007.01.013
[25] Cha SM, Shin HD, Ahn BK. Refracture after plate removal following ulnar shortening osteotomy for ulnar impaction syndrome – a retrospective case-control study. J Plast Surg Hand Su. 2021;55(1):48–55. https://doi.org/10.1080/2000656X.2020.1828900