ORIGINAL RESEARCH ARTICLE
Duplex ultrasound analysis of hemodynamic changes following microsurgical repair of unilateral digital artery injuries: a retrospective follow-up study
Justus Osterloha,b, Bastian Drollmanna, Luca Kümmerla, Andreas Arkudasa, Raymund E. Horcha and Aijia Caia
aDepartment of Plastic and Hand Surgery and Laboratory for Tissue Engineering and Regenerative Medicine, University Hospital Erlangen, Friedrich-Alexander University Erlangen-Nürnberg (FAU), Erlangen, Germany; bDepartment of Plastic and Hand Surgery, University of Freiburg Medical Centre, Medical Faculty of the University of Freiburg, Freiburg, Germany
ABSTRACT
Background: Whether unilateral digital artery injuries benefit from surgical repair remains controversial, as perfusion is typically preserved by the remaining, contralateral artery. Evidence on the long-term patency and hemodynamic effects of reconstructed unilateral arteries is limited. This study aimed to evaluate the patency and flow characteristics of digital arteries after microsurgical repair using duplex ultrasonography.
Methods: A retrospective single-center study was conducted including patients with unilateral digital artery injuries at the level of the digit who underwent primary microsurgical anastomosis between 2017 and 2022. Patients with fractures, proximal injuries, or vein grafts were excluded. Duplex ultrasonography was used to assess arterial patency and blood flow at follow-up.
Results: Twenty-seven patients were examined at a mean follow-up of 37 months (range 16–82). Duplex ultrasonography demonstrated anterograde flow in 26 of 27 reconstructed arteries (96.3%). The median flow volume in the repaired artery (1.1 ml/min, interquartile range [IQR]: 0.5–2.8) was significantly lower than in the contralateral artery of the same digit (3.6 ml/min, IQR: 1.4–7.7) and the corresponding artery of the contralateral hand (2.8 ml/min, IQR: 1.3–6.8). No significant compensatory increase was observed in the intact artery of the injured digit compared with its contralateral counterpart.
Conclusion: Duplex sonography demonstrates that repaired unilateral digital arteries remain patent in the long term, despite reduced flow compared with contralateral controls. While the functional benefit of arterial repair remains uncertain, long-term patency suggests a potential role for repair in selected cases to support vascular integrity.
KEYWORDS: Microsurgery; duplex ultrasonography; arterial anastomosis; digital vascularization.
Citation: Journal of Plastic Surgery and Hand Surgery 2026; 61: 51–55. DOI: https://doi.org/10.2340/jphs.v61.45557.
Copyright: © 2026 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 25 September 2025; Accepted: 27 January 2026; Published: 25 March 2026
CONTACT: Justus Osterloh Justus-Osterloh@web.de Department of Plastic and Hand Surgery, University of Freiburg Medical Centre, Medical Faculty of the University of Freiburg, Hugstetter Straße 55, 79106, Freiburg, Germany
Competing interests and funding: The authors declare no conflicts of interest related to this study.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Introduction
Hand injuries are very common and are reported to account for up to 30% of all patients presenting to emergency departments [1, 2]. In case of vascular injury, when both arteries of a digit are transected, inadequate perfusion leads to ischemia, necrosis, and ultimately amputation, making vascular repair mandatory. In contrast, in unilateral digital artery injuries, the digit typically remains viable due to the dual blood supply, and the indication for arterial repair is less clear. Accordingly, clinical studies and reviews describe that, in routine clinical practice, isolated unilateral digital artery injuries with adequate collaterals and preserved digital perfusion are often not routinely repaired [3–5]. While some centers prioritize nerve or tendon repair in unilaterally perfused digits, others advocate for arterial reconstruction to optimize vascularization and potentially support healing and regeneration [3, 6–9]. The functional relevance of unilateral digital artery repair has been debated. Several studies have compared outcomes in digits with one versus two patent arteries, with conflicting results regarding sensory recovery, neuroma formation, and cold intolerance [3, 8, 9]. However, little is known about the long-term patency of repaired unilateral digital arteries and the associated hemodynamic changes in the affected digits. Clinical assessment of vascular status typically relies on capillary refill, skin color, and temperature, but these parameters are not sufficiently reliable or standardized to confirm vessel patency. Definitive assessment would require imaging, with duplex ultrasonography offering a noninvasive, cost-effective, and widely available method for evaluating vascular flow [10–12]. Despite its established role in other vascular diagnostics, its application in the context of digital artery repair has been scarcely studied.
The aim of this study was therefore to evaluate the long-term patency and flow characteristics of digital arteries after microsurgical repair using duplex ultrasonography.
Material and methods
A retrospective analysis was conducted at a single center, focusing on patients with unilateral digital artery transection who underwent microsurgical anastomosis between 2017 and 2022. Eligible patients were identified using the Operationen- und Prozedurenschlüssel (OPS) code for microsurgical anastomosis of digital arteries. Inclusion criteria were sharp injuries to a digital artery at the level of the digit and primary microsurgical repair performed within 6 h of referral to the emergency department. Exclusion criteria were associated fractures, injuries proximal to the digit, or the use of vein grafts.
All adult patients received 100 mg acetylsalicylic acid daily for 4 weeks after surgery. Patients were contacted by telephone and invited for follow-up examination. Written informed consent was obtained from all participants. Information on regular medication use prior to trauma was collected from medical records and patient history.
All examinations were performed by a single experienced investigator under standardized conditions. To minimize physiologic fluctuations in digital blood flow, all participants underwent an acclimatization period of 20 min at constant room temperature prior to the examination. Examinations were conducted with the patient in a seated position, with both hands supported at heart level on an examination table. Prior to sonographic assessment, finger length was measured from the metacarpophalangeal joint to the fingertip. Patency and anterograde flow of the reconstructed digital artery were assessed using Allen test and duplex ultrasonography (Figure 1). Duplex ultrasonography was performed using GE HealthCare’s LOGIQ™ E10 series with a high-frequency linear L6–24 MHz transducer using a manufacturer-provided preset for finger examination. Standard B-mode imaging was combined with color Doppler and pulsed-wave Doppler ultrasound to assess vessel morphology, patency, flow direction, and flow velocity. Anterograde arterial blood flow distal to the anastomosis was confirmed using color Doppler imaging and spectral Doppler waveforms. Volume flow was calculated based on time-averaged mean velocity and vessel diameter measurements obtained in longitudinal section. Anterograde blood flow in the reconstructed artery was compared with the contralateral artery of the injured digit and with the corresponding finger of the uninjured hand.
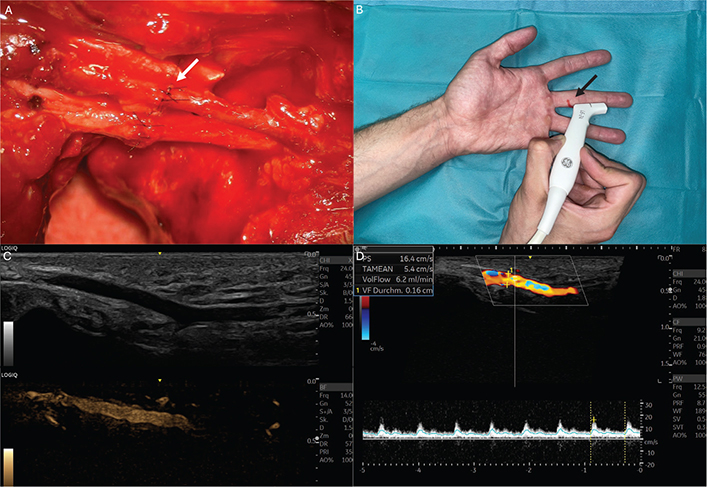
Figure 1. Images of a representative patient with unilateral digital artery repair included in this study. (A) Image showing microsurgical anastomosis of a unilateral digital artery (white arrow) (B) Clinical scenario of duplex ultrasound examination measuring signals distal to the vascular anastomosis. The height of injury and anastomosis is marked in red (black arrow). (C) Ultrasound images showing digital artery in B and M Mode. (D) Duplex sonography of digital artery measuring diameter, peak systole (PS) and volume flow (VolFlow).
For descriptive purposes, the digital arteries were labeled A1–A10, corresponding to the thumb radial digital artery (A1), thumb ulnar digital artery (A2), index radial (A3), index ulnar (A4), middle radial (A5), middle ulnar (A6), ring radial (A7), ring ulnar (A8), little finger radial (A9), and little finger ulnar digital artery (A10).
Statistical analyses were performed using R software (version 2024.09.0+375; R Foundation for Statistical Computing, Vienna, Austria). Volume flow measurements were assessed for normal distribution and were found to be non-normally distributed. Accordingly, these data are presented as median and interquartile range (IQR), and group comparisons were performed using the Wilcoxon rank-sum test. Other continuous variables are reported descriptively as mean and range. Results were considered significant at p < 0.05.
Ethics
The study was performed in accordance with the ethical standards of the Declaration of Helsinki and was approved by the local ethical review committee (No. 23-236-B).
Results
We identified 333 patients with digital artery transection who underwent microsurgical anastomosis at the Department of Plastic and Hand Surgery of the University Hospital Erlangen. Of these, 133 were excluded based on the predefined exclusion criteria. Among the remaining 200 eligible patients, 27 consented to participate and presented for follow-up examination. The main reason for non-inclusion was that patients declined or did not attend the scheduled appointment despite telephone contact.
The mean age of the patients was 38 years (range 8–63). Six patients were female (22.2%), and 21 patients were male (77.8%). Six patients (22.2%) reported regular medication use prior to trauma including antihypertensive drugs (n = 4), acetylsalicylic acid (n = 2), and thyroid hormone replacement therapy (n = 4). The mean duration between the surgery and the examination (follow-up) was 37 months (range 16–82). In 10 patients (37.0%), the right hand was affected and in 17 patients (63.0%), the injury occurred on the left hand. The mean length of the injured finger (measured from MCP-joint to fingertip)was 8.8 cm (range 6.0–12.0 cm). Twelve patients (44.4%) additionally had injuries to the flexor tendon and 25 patients had injuries of the digital nerve (92.6%). The mean surgery time was 116 min (range 92–148 min). In the study cohort every digital artery (A1–A10) was affected while injuries of the digital artery A3 (6 patients, 22.2%) and A10 (5 patients, 18.5%) were most common (Table 1).
Duplex ultrasound imaging demonstrated anterograde arterial blood flow in the sutured digital artery distal to the anastomosis in 26 of 27 patients (96.3%). The volume blood flow distal to the anastomosis of the sutured artery was 1.1 ml/min (IQR: 0.5–2.8 ml/min). This was significantly lower than the median volume blood flow of the contralateral side of the injured finger at the same height (3.6 ml/min [IQR: 1.4–7.7 ml/min]; p = 0.01, Wilcoxon test). The median blood flow of the anastomosed vessel was also significantly lower than the median blood flow of the corresponding artery of the contralateral hand (1.1 ml/min [IQR: 0.5–2.8 ml/min] vs. 2.8 ml/min [IQR: 1.3–6.8 ml/min]; p = 0.01, Wilcoxon test). When comparing the median blood flow of the intact artery of the injured finger with the corresponding artery of the contralateral hand, we could detect no significant difference (3.6 ml/min [IQR: 1.4–7.6] vs. 5.2 ml/min [IQR: 1.3–8.3]; p = 0.76, Wilcoxon test) (Figure 2).
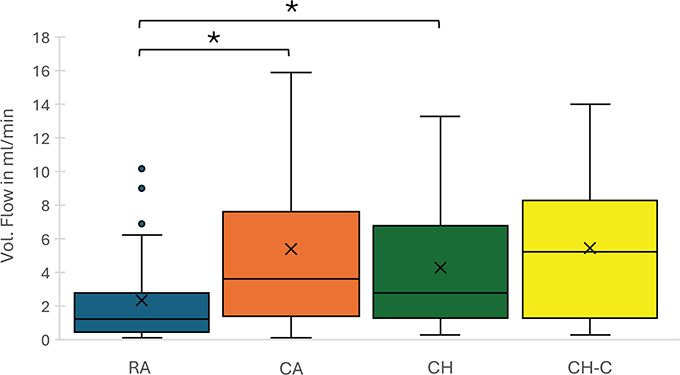
Figure 2. Box plots illustrate the volume flow measurements obtained via duplex ultrasonography. The groups include the microsurgically reconstructed arteries (RA), contralateral arteries of the affected finger (CA), corresponding arteries of the affected artery in the contralateral hand (CH), and contralateral arteries in the contralateral hand (CH-C). The boxes represent the interquartile range (IQR), with the horizontal line indicating the median. Whiskers extend to the minimum and maximum values within 1.5× IQR, while outliers are displayed as individual points. Statistical differences between groups were assessed using Wilcoxon rank-sum test.
Discussion
In this study, we found that 96.3% of digital arteries repaired with microsurgical anastomosis remained patent at a mean follow-up of 37 months, as demonstrated by duplex ultrasonography. Anterograde blood flow in the reconstructed arteries was significantly lower than in contralateral controls, while the intact arteries of injured digits showed no compensatory increase compared to the opposite hand. However, the role of duplex ultrasonography in the assessment of digital artery injuries is not well established, and its relevance for clinical management has not been clearly defined. In a digit with unilateral arterial injury that is clinically viable and shows normal capillary refill, poor or absent flow on ultrasound alone would not justify reoperation. Instead, ultrasound should be considered an adjunct to clinical assessment, particularly in cases where perfusion is doubtful or where closed arterial injuries are suspected.
The role of unilateral digital artery repair remains debated [3, 8, 9]. Arterial repair is unquestionably indicated in cases of total amputation or avascularity following bilateral vascular damage to restore blood supply and prevent necrosis or amputation. However, in cases of unilateral arterial damage, there is less clarity regarding the optimal therapy and the indication for arterial repair [8–10]. If the affected digit remains well perfused, some centers perform digital nerve repair but may choose not to reconstruct the injured artery. Microsurgical anastomosis of digital arteries is technically demanding due to the small vessel caliber and complex anatomy, requiring a surgical microscope. This procedure also prolongs the duration of surgery, making careful evaluation of its benefits essential. In our cohort, the mean operative time was nearly 2 h, primarily due to the microsurgical anastomosis. This highlights the practical trade-off between potential vascular benefit and longer operative time.
Previous studies have reported conflicting outcomes regarding the functional impact of digital artery repair. Dastagir et al. investigated the differences between one- and two-arterial blood supplies in the finger using questionnaires, clinical examinations, and circulatory imaging. They found no significant differences between the reconstruction and non-reconstruction groups [8]. Similarly, Yildiran et al. studied the impact of intact digital arteries on peripheral nerve regeneration after digital nerve injury [10]. No statistical significance was observed between the intact and the non-repaired artery groups regarding neuroma formation, two-point discrimination (2PD), or cold intolerance. However, in contrast to Dastagir et al. and Yildiran et al., Piquet et al. demonstrated statistically significant benefits in sensory recovery and reduced cold intolerance in patients with a patent artery following microsurgical anastomosis [9].
A major limitation of this study is its retrospective design without a control group and the low inclusion rate: only 27 of 200 eligible patients ultimately attended follow-up. This introduces a risk of selection bias, as patients who agreed to participate may not be representative of the broader cohort. Additionally, duplex ultrasound remains an examiner-dependent imaging tool and objective imaging results are needed to validate these findings. This is further highlighted by the variability observed in the volume flow of the digits (Figure 3). For instance, the median digital artery flow in finger artery A1 was found to be higher in the reconstructed artery group compared to both the contralateral artery and the healthy hand groups – an unexpected finding from a physiological perspective. However, variations in factors such as hand size, occupation, hobbies, comorbidities and gender may influence digital artery flow. These factors were not accounted for in the study design. As a result, the reliability of volume flow quantification using duplex sonography remains uncertain. Prospective studies, ideally including healthy volunteers and inter-observer assessments, are needed to clarify the reproducibility of duplex-based volume flow measurements. Advanced imaging modalities such as magnetic resonance angiography (MRA) provide more detailed visualization of digital arteries but are more resource-intensive and cannot quantify flow [13]. Another limitation is the wide age range of the included patients (8–63 years). Children and adults may differ considerably in terms of vascular healing capacity, remodeling potential, and long-term outcomes after digital artery repair [14]. Due to the limited sample size, subgroup analyses by age were not feasible in this study. Furthermore, regular medication use with potential effects on peripheral circulation, such as antihypertensive drugs or acetylsalicylic acid, was present in a minority of patients and may represent a confounding factor. Future prospective studies with larger cohorts should stratify outcomes by age group to provide more specific insights.
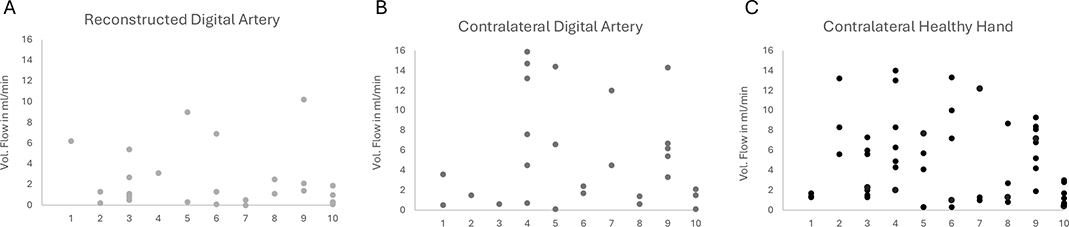
Figure 3. Dot plots (A–C) showing the volume flow measurements of digital arteries (A1–A10). Each dot represents an individual measurement. (A) Volume flow in microsurgically anastomosed arteries. (B) Volume flow in the contralateral artery of the affected finger. (C) Volume flow in the corresponding arteries of the contralateral healthy hand. The comparison highlights differences in perfusion between reconstructed and native arteries.
Conclusion
Unilateral digital artery repair with microsurgical anastomosis is technically and timely demanding and may not always be prioritized in hand trauma. Although functional benefits remain unproven, our findings show that repaired digital arteries maintain long-term patency, which may justify arterial repair in selected cases to optimize vascularization and reduce the risk of future ischemic complications.
Acknowledgments
The present work was performed in (partial) fulfillment of the requirements for obtaining the degree ‘Dr. med.’ (M.D.) of the Friedrich-Alexander-Universität Erlangen-Nürnberg, Medizinische Fakultät for Bastian Drollmann.
References
[1] Angermann P, Lohmann M. Injuries to the hand and wrist. A study of 50,272 injuries. J Hand Surg. 1993;18(5):642–644. https://doi.org/10.1016/0266-7681(93)90024-A
[2] Ootes D, Lambers KT, Ring DC. The epidemiology of upper extremity injuries presenting to the emergency department in the United States. Hand (N Y). 2012;7(1):18–22. https://doi.org/10.1007/s11552-011-9383-z
[3] Dastagir N, Obed D, Bucher F, et al. Blood vessel injuries of the fingers: a clinical comparison of one- and two-arterial blood supply. J Clin Med. 2023;12(18). https://doi.org/10.3390/jcm12185889
[4] Linnaus ME, Langlais CS, Kirkilas M, et al. Outcomes of digital artery revascularization in pediatric trauma. J Pediatr Surg. 2016;51(9):1543–1547. https://doi.org/10.1016/j.jpedsurg.2016.04.011
[5] Gelberman RH, Blasingame JP, Fronek A, et al. Forearm arterial injuries. J Hand Surg Am. 1979;4(5):401–408. https://doi.org/10.1016/S0363-5023(79)80031-3
[6] Eming SA, Martin P, Tomic-Canic M. Wound repair and regeneration: mechanisms, signaling, and translation. Sci Transl Med. 2014;6(265):265sr6. https://doi.org/10.1126/scitranslmed.3009337
[7] Johnson KE, Wilgus TA. Vascular endothelial growth factor and angiogenesis in the regulation of cutaneous wound repair. Adv Wound Care (New Rochelle). 2014;3(10):647–661. https://doi.org/10.1089/wound.2013.0517
[8] Yildiran G, Sutcu M, Akdag O, et al. Long-term outcomes of digital nerve repair accompanied by digital artery injury in flexor zone 2. Surg J (N Y). 2020;6(1):e7–e9. https://doi.org/10.1055/s-0039-3400229
[9] Piquet M, Obert L, Laveaux C, et al. Influence of palmar digital artery patency on neurological recovery of palmar digital nerve lesions. Chir Main. 2010;29(2):94–99. https://doi.org/10.1016/j.main.2009.12.004
[10] Hussain ST. Blood flow measurements in lower limb arteries using duplex ultrasound. Ann R Coll Surg Engl. 1997;79(5):323–330.
[11] Perko MJ. Duplex ultrasound for assessment of superior mesenteric artery blood flow. Eur J Vasc Endovasc Surg. 2001;21(2):106–117. https://doi.org/10.1053/ejvs.2001.1313
[12] Schöning M, Walter J, Scheel P. Estimation of cerebral blood flow through color duplex sonography of the carotid and vertebral arteries in healthy adults. Stroke. 1994;25(1):17–22. https://doi.org/10.1161/01.STR.25.1.17
[13] Salehi Ravesh M, Lebenatus A, Bonietzki A, et al. High-resolution, non-contrast-enhanced magnetic resonance angiography of the wrist, hand and digital arteries using optimized implementation of Cartesian quiescent interval slice selective (QISS) at 1.5 T. Magn Reson Imaging. 2021;78:58–68. https://doi.org/10.1016/j.mri.2021.02.008
[14] Haldeman PB, Harfouche C, Rosales R, et al. Immediate and delayed flap reconstruction have equivalent outcomes and associated costs following soft tissue sarcoma surgery. J Surg Oncol. 2024;130(3):562–568. https://doi.org/10.1002/jso.27770