ORIGINAL RESEARCH ARTICLE
Functional results after extensor indicis proprius to extensor pollicis longus tendon transfer for ruptures associated with distal radius fractures
Ingrid Andreassona,b  , Christos Ni. Sarigiannisb,c , Michael Ullmanb,d and Anders Björkmanb,c
, Christos Ni. Sarigiannisb,c , Michael Ullmanb,d and Anders Björkmanb,c
aDepartment of Occupational Therapy and Physiotherapy, Sahlgrenska University Hospital, Gothenburg, Sweden; bInstitute of Clinical Sciences, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden; cDepartment of Hand Surgery, Sahlgrenska University Hospital, Gothenburg, Sweden; dDepartment of Orthopedics, Sahlgrenska University Hospital, Gothenburg, Sweden
ABSTRACT
Rupture of the extensor pollicis longus (EPL) tendon is a recognised complication after distal radius fracture (DRF) that leads to loss of active thumb extension. Transfer of the extensor indicis proprius (EIP) tendon to the EPL is one of the most common reconstructive procedures, but prospective outcome data are limited. This study evaluated functional and patient-reported outcomes after EIP-to-EPL tendon transfer exclusively in patients with EPL rupture secondary to DRF. Thirty consecutive patients (26 women, 4 men; median age 65 years, range 17–80) underwent EIP-to-EPL tendon transfer between 2021 and 2025 for EPL rupture secondary to DRF. Thumb motion, grip and pinch strength and QuickDASH scores were recorded at 3 and 6 months postoperatively. All motion parameters improved between 3 and 6 months. At 6 months, lift-off height recovered to approximately two-thirds, total thumb flexion to > 80% and radial/palmar abduction to about 90% of the contralateral side. Grip and pinch strength reached 79–85% of the uninjured hand. Mean QuickDASH score improved from 29 to 21 points (p = 0.015). In conclusion, EIP-to-EPL tendon transfer restores satisfactory thumb motion, strength and patient-rated function following EPL rupture associated with DRF. Functional recovery at 6 months is comparable to that of patients with uncomplicated DRFs.
Clinical Trials registry no. NCT05264675
KEYWORDS: EPL rupture; EIP transfer; distal radius fracture; functional outcome; patient-reported outcome
Citation: Journal of Plastic Surgery and Hand Surgery 2026; 61: 140–145. DOI: https://doi.org/10.2340/jphs.v61.46150.
Copyright: © 2026 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 3 December 2026; Accepted: 11 May 2026; Published: 26 May 2026.
CONTACT: Ingrid Andreasson ingrid.f.andreasson@gu.se Department of Occupational Therapy, Sahlgrenska University Hospital, 431 80 Mölndal, Sweden
Competing interests and funding: The authors declare no competing interests.
This study was funded by Västra Götaland local research funding under Grant (VGFOUGSB- 964048).
Introduction
The extensor pollicis longus (EPL) tendon is the primary extensor of the thumb, producing extension at both the metacarpophalangeal and interphalangeal joints [1]. Rupture of the EPL results in the characteristic inability to actively extend the thumb, which can severely impair hand function and dexterity [2]. Distal radius fractures (DRFs) are a well-recognised cause of EPL rupture [3, 4]. The reported incidence of EPL rupture following a DRF varies with the management approach. After non-operative management, rupture rates as high as 5% have been described, whereas the rate following osteosynthesis is generally less than 1% [5–8]. Multiple mechanisms have been proposed, including compromised tendon vascularity due to bleeding and increased pressure within the tendon sheath at the level of Lister’s tubercle, attrition from sharp fracture fragments and mechanical irritation from screws or hardware after open reduction and internal fixation [8–10].
Several surgical strategies have been described to restore thumb extension after EPL rupture, such as primary repair, interposition grafting and tendon transfer. Transfer of the extensor indicis proprius (EIP) tendon to the EPL has become one of the most widely used techniques, offering reliable restoration of thumb extension with minimal functional deficit in the index finger [11, 12]. However, evidence from prospective series, particularly in patients with EPL rupture secondary to DRF, is scarce [11, 13].
Given that DRFs are among the most common upper extremity fractures, with an incidence that is continuing to rise due to the ageing population and increased activity levels [14–16], the absolute number of EPL ruptures is also expected to increase. A clearer understanding of functional outcomes after EIP-to-EPL tendon transfer in this context is therefore of growing clinical relevance. This study prospectively evaluated thumb motion, strength and patient-reported outcomes after EIP-to-EPL tendon transfer in patients with EPL rupture following DRF.
Patients and methods
Between October 2021 and March 2025, consecutive patients aged ≥16 years presenting with EPL rupture following a prior DRF were prospectively included. All patients underwent EIP-to-EPL tendon transfer. Exclusion criteria included rheumatoid arthritis, symptomatic CMC-1 arthritis, previous thumb fracture, de Quervain tenosynovitis, or inability to comply with postoperative rehabilitation. Patients with surgically treated DRF underwent a CT scan to exclude protruding osteosynthesis material as a cause of EPL rupture.
Surgical technique
A longitudinal incision was made over the rupture site at the base of the first metacarpal. The EIP tendon was harvested through a small transverse incision over the dorsum of the index metacarpophalangeal joint, rerouted distal to the extensor retinaculum and sutured to the EPL distal stump using either the side-to-side technique described by Fridén or a Pulvertaft weave [17], depending on surgeon preference. Figures 1–3 demonstrate the surgical technique for EIP to EPL tendon transfer. Figures 4–5 illustrate the suture techniques.
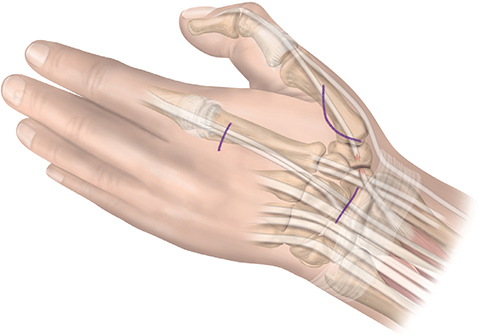
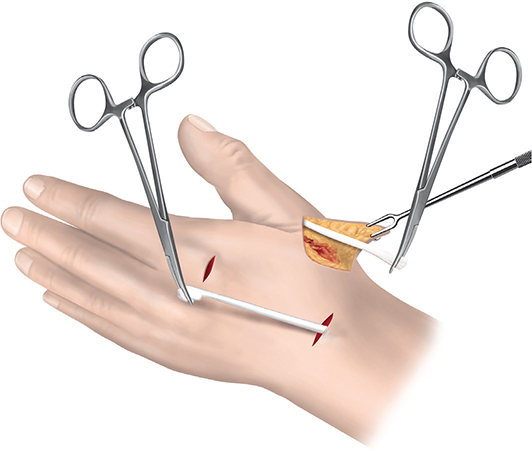
Figure 2. Harvesting of the EIP tendon.
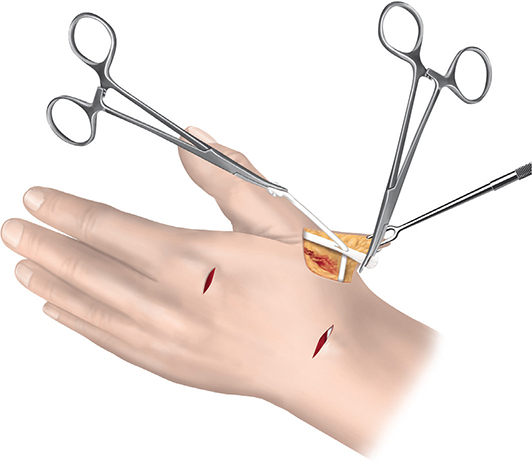
Figure 3. Rerouting of the EIP tendon to the EPL tendon.

Figure 4. Tendon coaptation using the Fridén technique.
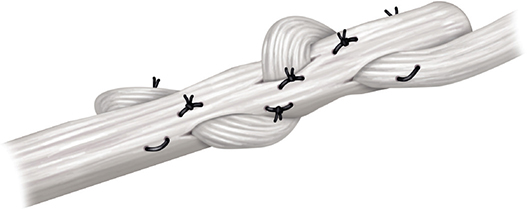
Figure 5. Tendon coaptation using the Pulvertaft technique.
Rehabilitation
The hand was immobilised in a plaster splint for 2–3 weeks. Patients were advised to perform gentle range of motion exercises for the thumb and wrist 4–5 times per day after splint removal. An orthosis, positioning the wrist in neutral position and the thumb in abduction-extension, was worn between training sessions until 4 weeks post-surgery. After that, patients wore wrist orthosis for another 2 weeks with support for the thumb only in case of extension defect. Gentle loading in daily activities was allowed from 6 weeks.
Functional assessment
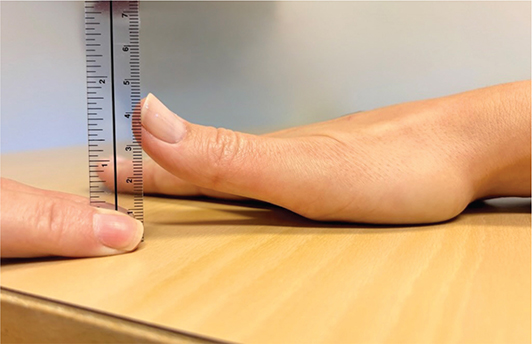
Patients were assessed 3 and 6 months after surgery. Thumb range of motion was evaluated by measuring lift-off height as well as radial and palmar abduction in millimetres using a ruler. Lift-off was assessed by measuring the distance from the tabletop to the radial nail fold [18], as seen in Figure 6, and for radial and palmar abduction, the distance between the ulnar nail fold of the thumb to the radial nail fold of the index finger was measured. The patients rested the hand under evaluation on the tabletop and were encouraged to use its full range of motion. Opposition was assessed by measuring the distance in millimetres from the thumb tip to the base of the little finger, with smaller values indicating better opposition.
Grip, tripod and lateral pinch strength were evaluated as the mean of three measurements using a Jamar dynamometer (Patterson Medical, Warrenville, IL, USA) and a standardised Pinch Gauge (B&L Engineering, Santa Fe Springs, USA). For each parameter, three consecutive measurements were obtained, and the mean value was recorded to reduce variability.
Patient-reported outcomes were collected using the Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH) questionnaire [19], which captures symptoms and functional limitations in daily activities. The questionnaire was administered at both follow-up visits to evaluate patient-perceived recovery over time.
Statistics
Analyses were performed using IBM SPSS Statistics, version 28.0 (IBM Corp., Armonk, NY, USA). Data distribution was assessed for normality using the Shapiro–Wilk test. Descriptive statistics were calculated for all variables. Continuous data are presented as mean values with standard deviations (SD) when normally distributed, or as medians with ranges when not normally distributed. Categorical variables are reported as counts and percentages.
Comparisons between the operated and contralateral uninjured sides were performed using independent-samples t-tests. Changes in quantitative measurements between the 3- and 6-month follow-up visits were analysed using paired samples t-tests when normality assumptions were met. For ordinal data and continuous variables not meeting normality assumptions, the Wilcoxon signed-rank test was applied. To express the degree of functional recovery, restoration ratios were calculated for each motion and strength parameter as:
(value of operated side ÷ value of contralateral side) × 100%.
All statistical tests were two-tailed, and a p-value of < 0.05 was considered significant. No adjustment for multiple comparisons was applied, as the study was exploratory in nature and intended to generate hypotheses for future confirmatory research.
Ethics
The study followed the principles of the Declaration of Helsinki and was approved by the Swedish Ethical Review Authority (2021-03523). All participants got oral and written information about the study and provided written consent to participate.
Clinical trials registry
The study was registered before the study start, NCT Number NCT05264675 (Unique protocol ID VGFOUGSB-964048). Last updated 241113.
Results
Thirty patients (26 women, 4 men; median age 65 years, range 17–80) were included.
The fractures were classified according to the AO classification system by CS [20]: seven (23%) were nondisplaced fractures (AO/OTA type A2.1), 11 (37%) were simple dorsally displaced extra-articular fractures (AO/OTA type A2.2), two (7%) were volarly displaced extra-articular fractures (AO/OTA type A2.3), four (13%) were extra-articular fractures with metaphyseal comminution (AO/OTA type A3), two (7%) were simple intra-articular fractures (AO/OTA type B), and four (13%) were severely comminuted intra-articular fractures (AO/OTA type C). Figure 7 shows radiographs from two representative patients from the cohort.

Figure 7. Radiographs from two representative patients from the cohort. (A, B) Minimally displaced distal radius fracture treated non-operatively. (C, D) Displaced distal radius fracture in a patient presenting with early EPL tendon rupture within days of injury. (E, F) Postoperative radiograph of the same patient after volar plate fixation of the distal radius fracture combined with tendon transfer.
Two patients, one female and one male, did not attend the 6-month follow-up; for these patients, only 3-month measurements are reported. The median time from fracture to EPL rupture was 29 [min 1, max 1,331] days. Seventeen ruptures occurred after nonoperative fracture management, and 13 after internal fixation, including two following corrective osteotomies. No protruding or misplaced osteosynthesis material was identified at the operated fractures. The median interval between rupture diagnosis and EIP-to-EPL tendon transfer was 12 days [range 0–321]. Strength data were normally distributed; other variables were not.
All motion parameters improved between 3 and 6 months (Table 1). The lift-off height increased significantly (p = 0.001) and reached approximately two-thirds of the uninjured contralateral side. Figure 8 shows an example of a patient in the ‘lift-off position’.

Figure 8. Patient with non-surgically treated DRF in the left (dominant) side, thumbs in maximum extension. The EIP-to-EPL transfer was conducted 8 months after the fracture. Picture 16 months after the operation.
Total thumb flexion exceeded 80% and interphalangeal flexion averaged >90% of the contralateral side. Most patients (93%) achieved full opposition, while radial and palmar abduction both recovered to about 93% of the contralateral side.
Grip and pinch strength increased significantly throughout the follow-up period. At 6 months, grip strength averaged about 80% and pinch strength 80–85% of the uninjured hand, both showing significant improvement from 3 months (p < 0.05). The mean QuickDASH score improved significantly from 29 points to 21 points (p = 0.015). Detailed results are presented in Table 1.
Discussion
This prospective study demonstrates that EIP-to-EPL tendon transfer for rupture of the EPL associated with DRF leads to good recovery of thumb motion, grip strength and patient-reported function within 6 months. Most patients regained near-normal range of motion, achieved full opposition, and recovered approximately 80–85% of grip and pinch strength compared with the contralateral hand. Importantly, these outcomes are comparable to those reported after uncomplicated DRF, indicating that reconstruction of the EPL can restore function to a level similar to that of patients without tendon rupture.
Recovery of thumb motion was generally good. Lift-off height and total flexion recovered to approximately 65% and 80% of the uninjured side, respectively, consistent with previous findings by Figl et al. [21] and Ha et al. [12]. Preservation of interphalangeal (IP) joint flexion is particularly important for functional pinch and grasp, and the present study confirmed that IP motion was well maintained, averaging 91% of the contralateral side. These results correspond closely to those of Adams et al. [13] and Lemmen et al. [22], who also demonstrated that near-normal IP flexion is achievable following tendon transfer. Moreover, radial and palmar abduction both recovered to more than 90% of the uninjured side, reflecting restoration of multidirectional thumb mobility and suggesting that the transfer does not compromise overall dexterity.
Hand strength followed a similar pattern of recovery. Both grip and pinch strength improved significantly between 3 and 6 months, reaching approximately 80–85% of the contralateral hand. These recovery outcomes align closely with those typically reported 6–12 months after DRF [23–25]. This comparison is clinically meaningful because it indicates that, once reconstructed, an EPL rupture does not appear to hinder the overall recovery process of the wrist and hand even in the early stages of rehabilitation after DRF. As the present results for strength and thumb motion are consistent with those of case series evaluating EIP-to-EPL tendon transfer with longer follow-up, across mixed aetiologies [12, 21], these findings suggest that the extent of functional improvements is greatest within the first 6 months and that later gains are more modest and gradual.
Patient-reported outcomes paralleled the objective measures. From 3 to 6 months, the mean QuickDASH score improved significantly from 29 to 21 points, approaching the lower limit of the 8–15 point threshold considered clinically important for upper-limb conditions [26]. This pattern is consistent with the recovery trajectory seen after DRF, where functional improvements are most pronounced during the first postoperative year [27]. The slightly higher QuickDASH scores herein compared with those in long-term EIP-to-EPL tendon transfer studies [12, 13] probably reflect the shorter follow-up in this cohort and the inclusion of patients still in the active rehabilitation phase.
In the present study, the time between EPL rupture to EIP-to-EPL tendon transfer ranged from 0–321 days, and outcomes were satisfactory across the study cohort. Similar functional results have been reported by Jung et al. [28] for EIP transfers performed 2–16 weeks following EPL rupture. This suggests that the timing from rupture to tendon transfer is not critical for the functional outcome.
The strengths of this study include its prospective design, a homogeneous cohort limited to EPL ruptures following DRFs, and a standardised rehabilitation protocol supervised by certified hand therapists. These factors enhance internal validity and minimise variation arising from surgical or rehabilitative techniques. Limitations include the relatively small sample size, which reduces generalisability, and the short length of follow-up, which does not capture how recovery plateaus beyond 6 months or the long-term durability of the transfer. Moreover, subtle donor-site effects on the index finger were not specifically assessed. Future investigations should therefore incorporate extended follow-ups, matched comparisons between DRF patients with and without EPL rupture, assessment of index finger function and qualitative assessments of patient-perceived dexterity and satisfaction.
Conclusion
EIP-to-EPL tendon transfer provides reliable restoration of thumb extension and flexion as well as grip and pinch strength after EPL rupture associated with DRF. Functional recovery at 6 months is comparable to that of patients with uncomplicated DRFs.
Acknowledgements
We would like to thank Pontus Andersson from Pontus Art Production for his valuable contribution in providing the illustrations showing the surgical technique.
AI was used only for writing assistance.
References
[1] D’Antoni AV. Gray’s anatomy, the anatomical basis of clinical practice, forty‐first edition, by Susan Standring, Editor‐in‐Chief, Elsevier Limited, 2016. ISBN: 978‐0‐7020‐5230‐9. Rochester: Wiley Subscription Services, Inc; 2016. p. 264–265.
[2] Gelb RI. Tendon transfer for rupture of the extensor pollicis longus. Hand Clin. 1995;11(3):411–422. https://doi.org/10.1016/S0749-0712(21)00062-7
[3] Bjorkman A, Jorgsholm P. Rupture of the extensor pollicis longus tendon: a study of aetiological factors. Scand J Plast Reconstr Surg Hand Surg. 2004;38(1):32–35. https://doi.org/10.1080/02844310310013046
[4] Sarigiannis CN, Ullman M, Andreasson I, et al. Inflammatory and degenerative changes in the extensor pollicis longus muscle and tendon following ruptures caused by distal radius fractures. BMC Musculoskelet Disord. 2025;26(1):10. https://doi.org/10.1186/s12891-024-08212-4
[5] Hove LM. Delayed rupture of the thumb extensor tendon. A 5-year study of 18 consecutive cases. Acta Orthop Scand. 1994;65(2): 199–203. https://doi.org/10.3109/17453679408995434
[6] Sato K, Murakami K, Mimata Y, et al. Incidence of tendon rupture following volar plate fixation of distal radius fractures: a survey of 2787 cases. J Orthop. 2018;15(1):236–238. https://doi.org/10.1016/j.jor.2018.01.030
[7] White BD, Nydick JA, Karsky D, et al. Incidence and clinical outcomes of tendon rupture following distal radius fracture. J Hand Surg Am. 2012;37(10):2035–2040. https://doi.org/10.1016/j.jhsa.2012.06.041
[8] Roth KM, Blazar PE, Earp BE, et al. Incidence of extensor pollicis longus tendon rupture after nondisplaced distal radius fractures. J Hand Surg Am. 2012;37(5):942–947. https://doi.org/10.1016/j.jhsa.2012.02.006
[9] Engkvist O, Lundborg G. Rupture of the extensor pollicis longus tendon after fracture of the lower end of the radius – a clinical and microangiographic study. Hand. 1979;11(1):76–86. https://doi.org/10.1016/S0072-968X(79)80015-7
[10] Kunes JA, Hong DY, Hellwinkel JE, et al.. Extensor tendon injury after volar locking plating for distal radius fractures: a systematic review. Hand (N Y). 2022;17(
[11] Ganon S, Bellity J, Zbili D, et al. Reconstruction strategies after rupture of the extensor pollicis longus tendon: a systematic review. Hand Surg Rehabil. 2020;39(6):502–507. https://doi.org/10.1016/j.hansur.2020.07.005
[12] Ha C, Hong IT, Oh CH, et al. Clinical outcomes of extensor indicis proprius tendon transfer for extensor pollicis longus tendon rupture. J Hand Surg Eur Vol. 2024;49(10):1243–1249. https://doi.org/10.1177/17531934241226949
[13] Adams AJ, Patel SJ, Arango SD, et al. Extensor tendon transfer for fracture-related extensor pollicis longus rupture: long-term outcome case series. J Hand Ther. 2024;37(4):529–533. https://doi.org/10.1016/j.jht.2024.02.004
[14] Stirling ERB, Johnson NA, Dias JJ. Epidemiology of distal radius fractures in a geographically defined adult population. J Hand Surg Eur Vol. 2018;43(9):974–982. https://doi.org/10.1177/1753193418786378
[15] Nellans KW, Kowalski E, Chung KC. The epidemiology of distal radius fractures. Hand Clin. 2012;28(2):113–125. https://doi.org/10.1016/j.hcl.2012.02.001
[16] Chung KC, Spilson SV. The frequency and epidemiology of hand and forearm fractures in the United States. J Hand Surg Am. 2001;26(5):908–915. https://doi.org/10.1053/jhsu.2001.26322
[17] Tsiampa V, Ignatiadis I, Papalois A, et al. Structural and mechanical integrity of tendon-to-tendon attachments used in upper limb tendon transfer surgery. J Plast Surg Hand Surg. 2012;46: 262–266. https://doi.org/10.3109/2000656X.2012.684097
[18] Sarigiannis CN, Andreasson I, Ekstrom L, et al. Normative data on extensor pollicis longus force, lift-off height, and tendon gliding amplitude. J Hand Ther. 2026
[19] Gummesson C, Ward MM, Atroshi I. The shortened disabilities of the arm, shoulder and hand questionnaire (QuickDASH): validity and reliability based on responses within the full-length DASH. BMC Musculoskelet Disord. 2006;7:44. https://doi.org/10.1186/1471-2474-7-44
[20] Meinberg EG, Agel J, Roberts CS, et al. Fracture and dislocation classification compendium-2018. J Orthop Trauma. 2018;32
[21] Figl M, Mayer M, Lederer S, et al. Extensor pollicis longus rupture after distal radius fracture: results of reconstruction by transposition of the extensor indicis tendon and postoperative dynamic splinting. Wien Klin Wochenschr. 2011;123(15–16): 485–487. https://doi.org/10.1007/s00508-011-0038-4
[22] Lemmen MH, Schreuders TA, Stam HJ, et al. Evaluation of restoration of extensor pollicis function by transfer of the extensor indicis. J Hand Surg Br. 1999;24(1):46–49. https://doi.org/10.1016/S0266-7681(99)90025-6
[23] Chung KC, Squitieri L, Kim HM. Comparative outcomes study using the volar locking plating system for distal radius fractures in both young adults and adults older than 60 years. J Hand Surg Am. 2008;33(6):809–819. https://doi.org/10.1016/j.jhsa.2008.02.016
[24] Bobos P, Nazari G, Lalone EA, et al. Recovery of grip strength and hand dexterity after distal radius fracture: a two-year prospective cohort study. Hand Ther. 2018;23(1):28–37. https://doi.org/10.1177/1758998317731436
[25] Brogren E, Hofer M, Petranek M, et al. Fractures of the distal radius in women aged 50 to 75 years: natural course of patient-reported outcome, wrist motion and grip strength between 1 year and 2–4 years after fracture. J Hand Surg (European Volume). 2011;36(7): 568–576. https://doi.org/10.1177/1753193411409317
[26] Gummesson C, Atroshi I, Ekdahl C. The disabilities of the arm, shoulder and hand (DASH) outcome questionnaire: longitudinal construct validity and measuring self-rated health change after surgery. BMC Musculoskelet Disord. 2003;4(1):11. https://doi.org/10.1186/1471-2474-4-11
[27] MacDermid JC, Roth JH, Richards RS. Pain and disability reported in the year following a distal radius fracture: a cohort study. BMC Musculoskelet Disord. 2003;4:24. https://doi.org/10.1186/1471-2474-4-24
[28] Jung SW, Kim CK, Ahn BW, et al. Standard versus over-tensioning in the transfer of extensor indicis proprius to extensor pollicis longus for chronic rupture of the thumb extensor. J Plast Reconstr Aesthet Surg. 2014;67(7):979–985. https://doi.org/10.1016/j.bjps.2014.03.006