ORIGINAL RESEARCH ARTICLE
Long-term longitudinal follow-up of individuals with UCLP after Gothenburg two-stage palate closure: surgical and speech outcomes
Hans Marka, Jan Liljaa and Christina Havstamb
aDepartment of Plastic Surgery, Sahlgrenska University Hospital and Institute of Clinical Sciences at Sahlgrenska Academy, University of Gothenburg, Sweden; bDepartment of Otorhinolaryngology, Division of Speech-Language Pathology, Sahlgrenska University Hospital and Institute of neuroscience and physiology, Department of Health and Rehabilitation, Speech and Language Pathology Unit, Sahlgrenska Academy, University of Gothenburg, Sweden
Background: Delayed hard palate closure in unilateral cleft lip and palate (UCLP) patients show on a safe surgical method and good speech outcome, however, occurrence of orally retracted articulation before hard palate closure at 8 years. The aim of this study was to describe surgical and speech outcome in UCLP patients closing the hard palate at 3 years.
Methods: A consecutive of 28 participants were operated with Gothenburg two-stage method including soft palate closure at 6 months and hard palate at 3 years. Surgical and speech outcome were evaluated. Recordings of sentences and spontaneous speech at 5, 10, 16, and 19 years were analyzed blindly and independently by three speech-language pathologists. Compensatory articulation, hypernasality, hyponasality, weak pressure consonants, and nasal air leakage were evaluated on ordinal four-point and intelligibility and perceived velopharyngeal function on three-point scales.
Results: Long-term follow-up revealed a safe surgical method. Articulation disorders were present in 25–30% at 5-year but largely not later. About 20% had incompetent velopharyngeal function at 5 years but none at 19 years. Most participants were well intelligible after 5 years. Hard palate closure at 3 years indicated less occurrence of orally retracted articulation compared with a cohort who had hard palate closure at 8.2 years.
Conclusions: Long-term, follow-up of individuals with UCLP after Gothenburg two-stage palate closure including closure of the soft palate closure at 6 months and hard palate at 3 years of age shows a safe surgical method and indicates less retracted oral articulation compared with hard palate closure at 8 years.
KEYWORDS: Cleft; Speech; Retracted articulation; Palatal repair
Citation: Journal of Plastic Surgery and Hand Surgery 2023; 58: 19–25. DOI: https://doi.org/10.2340/jphs.v58.7317.
Copyright: © 2023 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material for non-commercial purposes, provided proper attribution to the original work.
Received: 18 October 2022; Accepted: 02 February 2023; Published: 14 June 2023
CONTACT Hans Mark hans.mark@vgregion.se Department of Plastic Surgery, Sahlgrenska University Hospital and Institute of Clinical Sciences at Sahlgrenska Academy, University of Gothenburg, Sweden.
Introduction
Decades of extensive effort have been dedicated to identifying the optimal timing and method of surgery to achieve the best outcome of facial growth and speech in unilateral cleft lip and palate (UCLP) treatment. Finding the optimal balance between waiting to close the cleft in order not to disturb palatal growth and hurrying to close the cleft to benefit speech development has been an ongoing challenge [1,2]. Both timing and type of surgery are presumed to influence results. Surgical trauma of the palate is generally considered to adversely affect the growth of the maxilla. It has been shown that a palatal scar created by velar surgery impairs maxillary development. If this scar is posteriorly located close to the posterior border of the hard palate, it might result in less growth restriction [3].
Also, the timing of surgery can affect growth and early surgical treatment of the palate can lead to major growth restriction [4,5]. However, results from a previous study indicate that there is no significant difference in growth on closing the hard palate between age 3–5 compared with 5–7 years of age [6,7]. Previous data on the development of the residual cleft during the growth after delayed palate closure show a reduction of the width of the residual cleft, with the greatest reduction until about 18 months of age when closing the soft palate at 6 months of age [8]. However, there is further reduction in width after that and 82% is functionally closed at 7 years [3].
Timing of both hard and soft palate closure is assumed to influence speech development, and several researchers have suggested that speech results seem to benefit from early timing of soft palate repair [9–11]. A functioning velum with competent velopharyngeal function enables pressure consonants in the posterior part of the oral cavity and thus counteracts the development of glottal or pharyngeal placement of articulation in a young child. A residual cleft in the hard palate compromises the production of pressure consonants in the anterior part of the oral cavity, and this may result in retracted oral articulation to a velar position (e.g., the consonant/t/produced as [k]). Several studies have reported speech development after different timing of hard palate repair. A study from Gothenburg investigated results on long-term speech when the hard palate was closed between 38 and 89 months of age and revealed no difference in articulation related to timing of hard palate repair [12]. The participants were divided into two subgroups: early delayed hard palate closure (DHPC) (hard palate closed at a mean age of 42 months) and late DHPC (hard palate closed at a mean age of 73 months), and the comparison showed only one statistically significant difference; the later the operation of the hard palate, the more the audible nasal airflow at age 7 years. Assessment of signs of velopharyngeal incompetence showed somewhat divergent results and the expected improvement of oral articulation errors was not evident. The authors suggested that the closure of the hard palate probably needed to be performed earlier for significant results but also small numbers and great variability in age of closure within each group make it difficult to draw safe conclusions. The Scandcleft multicenter study [13] did observe a statistically significant difference between a group that had a long delay in hard palate closure (at around 36 months) compared to a short delay in hard palate closure (at around 12 months), where earlier closure resulted in less retracted oral articulation errors. Another study investigated whether a temporary covering of the residual cleft in the hard palate with early infant jaw-orthopedics would have a beneficial effect on early speech production at 18 months of age. No such effects were seen, but the number of participants was small as only 10 children were included in each group.25
In Gothenburg, DHPC was performed in patients with UCLP between 1975 and 1993. The soft palate was closed at 6 months and a DHPC was performed at around 8 years of age. The DHPC method is a surgical protocol developed after long-term follow-up of different previous surgical methods for closing UCLP. These methods indicate that early bone grafting as well as creating surgical scars interfering with vomero-premaxillary sutures significantly contributes to growth restriction of the maxilla [3,14]. In contrast, long-term results of maxillary growth of patients with DHPC measured from roentgencephalograms at 5, 10, 16, and 19 years of age showed very good maxillary growth even up to the final examination, a finding supported by the low need for orthognathic surgery (10%) [3,15]. An evaluation of speech results used standardized audio recordings of 55 patients from the same cohort of patients with DHPC, and they were analyzed blindly for cleft speech characteristics at 5, 7, 16, and 19 years of age and at the clinic at age 10 [11,16]. Prominent hypernasality and oral articulation errors at age 5 years were markedly reduced throughout the years with low prevalence at ages 16 and 19 years. Pharyngeal flap surgery was performed in six of the 55 patients (11%). Retracted oral articulation was present in 39% of the participants at 5 years of age and in 23% at age 7 (before hard palate closure). However, at age 10, retracted oral articulation was present in only 6%, and at age 19, only in one out of the 55 participants was present. In an effort to improve articulation results, a modified version with less delay in closing the hard palate named two-stage palate closure was introduced in 1993, closing the soft palate as at 6 months and the hard palate at 3 years of age. The main purpose of this investigation was to study the surgical and speech outcome after the modified two-stage palate closure. More specifically, would the occurrences of retracted oral articulation decrease in this cohort compared with the group with earlier DHPC closure?
Methods
A total of 28 consecutive patients, born with UCLP between 1993 and 1996, were surgically treated with two-stage palate closure including lip and soft palate closure at 6 months and hard palate closure at 3 years at Sahlgrenska University Hospital, Gothenburg, Sweden. The surgical protocol is described in detail by Mark and Lilja [17].
The surgical method of the soft palate repair at 6 months was the same as used in DHPC closing the hard palate at 8 years. In summary, the soft palate closure includes incisions that follow a zig-zag route at the border between the hard and soft palate, posterior to the greater palatine artery. A posterior-based vomer flap is dissected and raised. Oral mucosal flaps in the soft palate are raised by blunt dissection. The insertions of velar muscles at the posterior border of the hard palate are cut, including the nasal mucosa. The muscle-mucosal flap is dissected free and mobilised posterior to the level of the opening of the Eustachian tube. Musculus levator veli palatine is included in the muscular bulk, which is sutured over the midline from both sides and also to the vomer flap. Oral mucosal flaps finally cover the raw surfaces of the muscle, nasal layer, and vomer flap. Seven of the patients, however, were operated in the soft palate with at different method of soft palate closure according to leg A in the Scandcleft study [18]. Therefore, these patients were excluded for speech evaluation resulting in a group of 21 patients. The surgical method of the hard palate repair at 3 years is as follows: A vomer flap is raised on the non-cleft side and an incision is made at the cleft border on the cleft side followed by subperiosteal dissection where the palatal mucosa is raised, and the vomer flap was tucked in and sutured. Twenty-eight patients were followed up on a regular basis at 18 months, 3, 5, 7, 10, 13, 16, and 19 years of age regarding the surgical outcome. In DHPC, the residual cleft was closed at the time of mixed dentition at 8 years in conjunction with the secondary alveolar bone grafting. The same surgical method closing the residual cleft with a ‘tuck in’ vomer flap from the non-cleft side was used.
Speech outcome
Seven children who were born after March 1996 were operated in the soft palate with the same technique later used in the Scandcleft study and were therefore excluded from the follow-up of speech results. The remaining 21 participants who had been recorded at their routine follow-ups were reassessed for speech recording at ages 5, 10, 16, and 19 years. One boy had moved to another part of Sweden after 5 years of age and therefore had not attended the later follow-ups. Thirteen participants were involved in an evaluation of the use of pre-surgical infant jaw-orthopedics, but no significant beneficial effects for early speech production were found at 18 months of age [12]. Therefore, they were not singled out in the present study, and all children treated with the same surgical protocol were considered as one group. In the previously studied group with DHPC, 39% of the 5-year-olds had retracted oral articulation (i.e., a palatal or velar place of articulation for dental high-pressure consonants). As an aim of this study was to assess whether an earlier closure of the hard palate had a positive impact on dental articulation, this speech variable was singled out for statistical comparison between the group with DHPC at around 8 years and the present group with hard palate closure at around 3 years of age.
Fistulas and speech improving surgery
Fistulas present posterior to the alveolar region before bone grafting affecting the speech were considered as true fistulas. Fistulas occurring after the bone grafting were considered as failures of the bone transplantation. Speech improving surgery includes velar re-repair and pharyngoplasty.
Hearing
Hearing and ear status were regularly followed up as part of our clinical routine. Not all participants attended all follow-up visits, but a majority (13/21) had consistent data from 5, 10, 16, and 19 years of age. Fourteen participants had been treated with grommets/ventilation tubes during their early years. At 19 years of age, 16 of the 21 participants had audiograms on the same day as the speech recording; 15 participants had normal hearing and one had a mild (20–40 dB) unilateral hearing loss.
Speech therapy
A chart review revealed inconsistent data collection with regard to speech therapy at the hospital or pre-school/school. Two participants had extensive speech therapy because of glottal articulation in their preschool years, and a total of 11 participants had had speech therapy to some degree, primarily at 3–10 years of age.
Speech analysis
Not all 21 children had available recordings from all ages but a majority did; 19 recordings were available from the follow-up at 5 years, 17 at 10 years, 15 from 16 years, and 17 from 19 years of age. From the available recordings the repeated sentences with pressure consonants, nasals and consonant clusters routinely used at Swedish cleft centers were edited out together with about 2 min of spontaneous speech elicited during play or retelling a story or film. These speech samples were put together for blinded independent assessments performed by three speech-language pathologists (SLPs) experienced in assessing cleft palate speech: two from the cleft center in Gothenburg and one from another cleft team in Sweden, to include an external rater. All judges assessed all speech material. When they disagreed, the median value was used. In addition, 30% of the material was re-assessed for calculation of intra-rater reliability. Both intra- and interrater reliability was calculated with percent exact agreement. The sentences were evaluated at all ages for retracted oral articulation of plosives, glottal plosives, and glottal, pharyngeal or nasal realisation of fricatives on four-point-scales. For the teenagers, distorted/s/-sounds were also assessed since this is more deviant from the norm at these ages. The sentences were also rated for signs of velopharyngeal incompetence; hypernasality, audible nasal airflow, and weak pressure consonants on four-point scales. The speech variables were identical to the ones used in the Swedish Articulation and Nasality Test (SVANTE), that all three raters were well accustomed to and use in clinical evaluations as it is a standardised used test by all Swedish cleft centers [19]. The definitions of the scale are displayed in Table 1.
The connected speech was rated at all ages for intelligibility on a three-point scale where 0 = normal/everything is intelligible, 1 = mildly reduced, and 2 = moderately to severely reduced. In addition, all speech material was used for judging the overall perceived velopharyngeal function on a three-point scale where 0 = normal/competent, 1 = marginally incompetent, and 2 = incompetent. Intrarater agreement was 97, 89, and 94%, respectively, for the three judges, and interrater agreement was calculated pairwise; between judges 1 and 2; 82%, judges 1 and 3; 82%, and judges 2 and 3; 81%.
Statistical analysis
In order to compare retracted oral articulation in this study with a previous study where the hard palate had been closed at a mean age of 8.2 years, both data sets were entered into the Statistical Package for the Social Sciences (SPSS). A non-parametric method was used as data were ordinal and distribution was skewed. A comparison of independent samples with two-tailed Mann–Whitney U-tests was performed at 5, 10, 16, and 19 years of age.
Ethical approval
This study was approved by the local ethics committee (Dnr 1020-12).
Results
Surgical results in total of 28 patients with two-staged palate closure
Soft palate closure was performed at a mean age of 6.25 months, and the median age was 6 months. The hard palate closure was performed at a mean age of 3 years and 4 months and a median age of 3 years and 3 months. Bone transplantation was performed at a mean age of 7 years and 10 months, and the median age was 7 years and 8 months.
Re-bone transplantation occurred in two patients (7%) and orthognathic surgery in one patient (4%). True fistulas were closed in two patients (7%), and fistula closure because of failure of bone transplantation was performed in four patients (14%). Both types of fistulas were symptomatic, in total 21%.
In the group with 21 patients (whose speech was assessed in the present study), speech improving surgery with secondary re-repair with intraveloveloplasty was performed in two patients (11%) and with pharyngealplasty in another two (11%). This resulted in a total frequency of 19% having speech improving procedures.
Speech results
Retracted oral articulation was assessed at 5, 10, 16, and 19 years of age. It was prevalent to some degree for approximately 25% of the 5-year-olds and was resolved at 10 years of age (Figure 1). The statistical comparisons of retracted oral articulation in this study and the previous study of DHPC (8.2 years) revealed no statistically significant difference, but there was a statistical trend at 5 years of age, p = 0.0507, Z = 1962. At later ages, the comparisons were far from statistical significance; at 10 years of age p = 0.188, Z = −1317, at 16 years of age p = 0.435, Z = −0.781, and at 19 years of age p = 0.543, Z = −0.608.
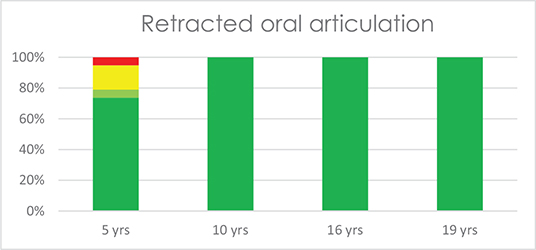
Figure 1. Occurrence of retracted oral articulation at 5, 10, 16, and 19 years of age where green = normal/no occurrence, light green = occurring once or twice, yellow = occurring often, red = occurring always or almost always.
Glottal plosives were present to some degree in about one-third of the group at 5 years of age but had reduced considerably at age 10 (Figure 2).

Figure 2. Retracted articulation to a glottal or pharyngeal level.
Two participants had one or two minor/s/-deviations in their late teens.
Signs of velopharyngeal incompetence were present mainly at 5 years of age. The overall impression of perceived velopharyngeal function on the three-point scale showed four participants with incompetent velopharyngeal function at 5 years of age, one at 10 and 16 years of age, and none at 19 years (Figure 3).
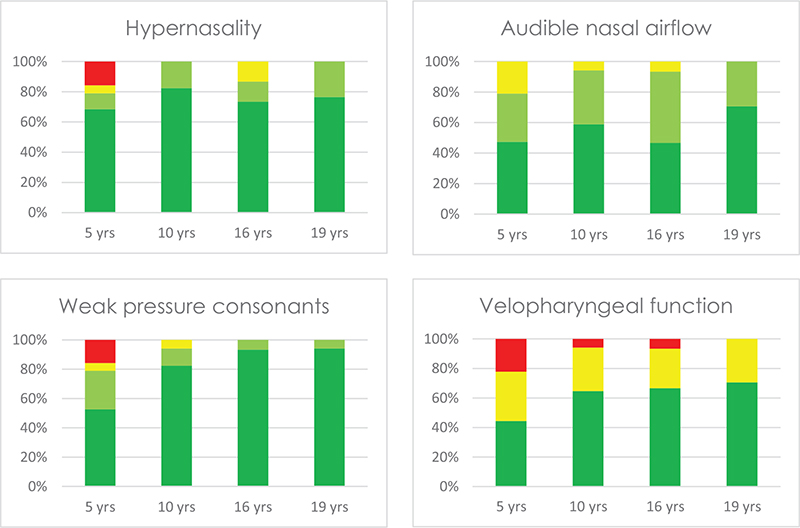
Figure 3. Signs of velopharyngeal dysfunction.
Hyponasality was present to a mild degree in approximately 20% of the participants at 5 and 10 years of age, not at all at 16 and in two individuals (13%) at 19 years of age. Two of the four individuals with mild hyponasality at 10 years of age had had pharyngal flaps at around 5 years of age. Both had available speech recordings from all ages, and no hyponasality was found when they were 16 or 19 years of age.
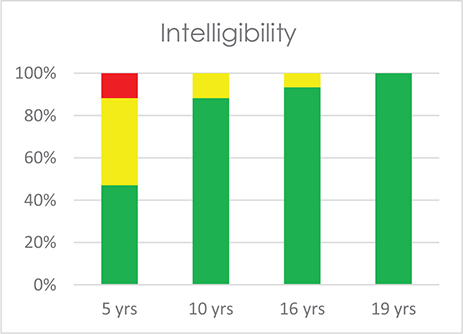
Intelligibility was reduced in about haft the group at 5 years of age. At 10 years, 88% of the patients were well intelligible and at 19 years of age all of them (Figure 4).
Discussion
There is still no conclusive scientific evidence for the recommended age for palatal closure. However, there is evidence showing that late palatal surgery is beneficial for palatal and midface growth, and on the other hand, early repair is beneficial for speech development [10]. In order to further understand this contradictory relation in cleft treatment, investigations aiming at reliable scientific follow-up of long-term treatment results are therefore crucial. It is complicated to perform such investigations internationally, because different health care systems, available scientific resources, and continuity of healthcare providers in different countries may have adverse effects on how data is collected, assessed, and interpreted. In an effort to achieve reliable long-term results, the present study used a careful follow-up timing of up to 19 years of age. Even though the 21 participants in the speech evaluation constitute a relatively small group, we believe the results point to a reduction of oral retracted articulation at 5 years of age when the hard palate closure was performed at a mean age of 3 years instead of 8 years. The statistical analysis of the difference was not statistically significant but did indicate a trend. This is probably because of small numbers in the present study. In our opinion, the clinical relevance of a reduction from 39% of the patients having a high incidence of retracted oral articulation in the previous DHPC study compared to one individual (5%) in the present study is still considerable (Figure 5).

Figure 5. Occurrence of retracted oral articulation in the previously studied cohort with delayed hard palate closure to the left and in the present study closing the hard palate at 3 years to the right.
The focus on p-values below 0.05 is questioned among several researchers where small numbers are investigated, and a transition to discussing whether the difference is of clinical relevance is suggested [20,21]. We interpret the findings of this study to indicate that an earlier closure of the residual cleft in the hard palate improved the opportunities for speech development of anterior pressure consonants. However, the Scandcleft study found that hard palate closure as early as age 12 months is preferable, when it was compared to hard palate closure at 3 years [13]. Another study focusing on primarily one stage palate repair investigated speech and vocabulary at 3 years of age and found that palate closure at age of 11 months instead of 15 months resulted in better articulation [22]. At our center, further long-term studies are in progress, evaluating the development of retracted oral articulation and its effect on speech with closing the residual cleft at 2 years. These studies must, however, be performed in conjunction with evaluation of the facial growth to find an optimal time point for closing the cleft with a two-stage procedure.
It could also be argued that with time, most patients born with a cleft palate develop normal speech, so the relatively small differences at younger ages are of less importance. However, a child may develop at less favorable attitude to communication if they speak in a way that is deviant from the norm and perhaps are less intelligible during their pre-school years [12,23]. A study of 10-year-olds’ communication attitudes revealed a more negative attitude in children born with a cleft involving the palate compared with children without clefts [24,25]. Studies of peers’ attitudes to 7- and 10-year-olds with cleft-specific speech errors revealed that they noticed even slight articulation errors and described them in less favorable ways [26,27]. These findings underline the importance of giving children the prerequisites to develop normal speech as early as possible to facilitate their communicative participation.
Intelligibility at 5 years of age was lower (47% were completely intelligible) compared to the results in the previous study of DHPC (64%) and a study by Sell et al. [28], where approximately 57% of the 5-year-olds had good intelligibility. The measurement of intellibility is difficult and different methods and standards are applied; to let SLPs, lay persons or parents rate the child’s speech or to investigate how many of the words are perceived correctly in a controlled test situation [29]. This makes the results subjective in nature and difficult to compare between different studies. Since we believe intelligibility is an important measure of speech function in a person’s everyday context, it is reported in this study despite its limitations. In future, we hope to be able to use internationally agreed standards for rating speech variables including articulation and signs of velopharyngeal insufficiency (VPI) as well as intellibility and to include and calibrate raters from different countries to be able to compare results, as was done in the Scandcleft project [30].
In order to compare the speech as accurately as possible, seven patients were excluded in the speech evaluation because of the difference in the method of soft palate closure. However, this method of soft palate closure is considered not to affect the growth, which is why it is included in the results of the surgical treatment as well as and as well as in a growth study of the same cohort. In this study, 22% of the participants had secondary velopharyngeal surgery which is a comparatively high number, but in line with the speech results of many other studies; a recent study of two cohorts of patients born with UCLP in Sweden showed 24 and 53% rates of pharyngeal flap surgery, respectively [23]. To use the prevalence of secondary velopharyngeal surgery as an evaluation method of speech results after primary surgery is difficult, as indications for surgical intervention can vary over time. The prevalence is influenced by other factors as well, such as the surgeons’ and SLPs’ opinions and the parents’ and patients’ own choice. Therefore, the indication for surgical intervention can vary between studies. Nevertheless, it must be considered an indication of the velopharyngeal function when comparing different methods of primary palate closure. The fact remains that a competent velopharyngeal function is a fundamental objective in cleft surgery, and it is unexpected and problematic that the occurrence of signs of VPI in this study was higher than before. The frequency of VPIs treated with pharyngeal flap in DHPC was 10% (5 out of 50), and 11% (2 out of 21) in the present study as well. To minimize the use of pharyngoplasty; an extensive procedure in the palate, a secondary palatoplasty including intravelar veloplasty was introduced in the beginning of the 1990s. This method therefore was an option for the cohort in the present study who closed the residual cleft in the hard palate at 3 years of age. In this group, two additional secondary speech improving procedures were therefore performed, 22% in total including the pharyngeal flaps. As before, the decision for speech improving surgery was based on the evaluation of VPI by a SLP, videofluoroscopy, and nasendoscopy but as there were no set criteria for the decisions either for pharyngealplasty or secondary palatoplasty including intravelar veloplasty, the decision basis for VPI-surgery could have changed from the previous cohort.
Over the years, the scientific organization in Sahlgrenska University hospital cleft team has aimed at regular long-term follow-up regarding growth, occlusion, speech, and appearance. The long-term outcome of growth and speech in DHPC has been reported to achieve very good maxillary growth as well as good speech. However, the typical retracted oral articulation related to the residual cleft was quite frequent during the early ages, especially before the repair of the hard palate and alveolus at 8 years of age. Interestingly though, the retracted oral articulation decreased even before the residual cleft was closed at 7 years in patients with DHPC, which is interpreted as an effect of a functionally closed residual cleft.
The present study of two-stage palate closure introduced in 1993 involves closing the hard palate earlier, that is a soft palate closure at 6 months and hard palate closure at 3 years, and it showed the same surgical results as in DHPC; low rates of symptomatic fistulas affecting the speech (7, respectively, 6%) but higher symptomatic fistulas in total (21%), re-bone grafting (7, respectively, 8%), and orthognathic surgery (4, respectively, 10%). These results must be considered acceptable in comparison to many other reported results of surgical methods [31]. The two-stage palatal closure can therefore, as the DHPC-method, can be considered a safe surgical method with acceptable risk for surgical complication in treatment of patients with UCLP.
The soft palate repair at 6 months of age is shown to guide the growth of the palate and therefore decrease the residual cleft to approximately 18 months of age. However, some residual clefts continue to decrease in width until 7 years of age. The development of a narrow and often functionally closed residual cleft has surgical advantages when closing it. A procedure closing a residual cleft at 3 years can, therefore, be made using a ‘tuck in’ flap from the vomer. This surgical method causes limited trauma in the palate earlier shown to be advantageous for less restriction of future palate growth. The need for mucoperiosteal flaps, less favorable for the growth because of scar formation, is limited. The 4% frequency of orthognathic surgery in this study indicates a very good growth. A detailed Goslon and encephalogram analysis of long-term outcome of maxillary growth after the HPC3 has been performed [32]. The frequency of surgical complications reported in this study is low and can be compared to other methods reported in the literature [31]. The reported growth and the presented surgical as well as the speech results in this study show on a acceptable safe surgical method.
Limitations
The methodology for assessing speech was largely copied from the article by Lohmander et al. [33], to facilitate comparison with the different surgical protocols. The method commonly used today is a phonetic transcription of each phoneme for the assessment of articulation, nasal air emission and weak pressure consonants. A limitation of the present study is that an earlier and outdated assessment method was used; however, the direct comparison with data from a previously used surgical protocol at the same center in Gothenburg was prioritized.
Not all children had speech recordings at all ages, and this limits the possibilities to follow speech development closely. This is a common problem when the time frame for follow-up is almost 20 years, as in our clinical routine. As just over 90% of the patients had available recordings of good quality at 5 years of age and in their late teens (either at 16 or 19 years of age), we propose that it is sufficient data to draw conclusions from.
Another limitation is the lack of consistent and detailed information on speech therapy, especially as the focus is on articulation errors, which are the most accessible cleft speech characteristics to correct with speech training. This is a common problem in cleft research where the aim is to tease out effects of a surgical protocol. An exception is the Scandcleft study where detailed information was collected, and a significantly negative correlation between correct consonants and number of speech therapy visits was found [13]. This was interpreted as an accurate identification of children with articulation disorders, but that the intervention that was offered was not efficient. Better and more detailed studies on effects of different types of speech therapy is highly needed for the cleft population, as pointed out by Bessell et al. [34], among others.
The fact that only 21 of the 28 participants were operated with the same method for soft palate closure and hence were included in the speech assessments is another unfortunate fact. Possibly, this reduction of participants contributed to the lack of statistical significance in the comparison of oral retracted articulation between this study group and the earlier study where closure of the had palate was performed at around 8 years of age.
Conclusions and implications for further research
Long-term, longitudinal follow-up of individuals with UCLP after Gothenburg two-stage palate closure including soft palate closure at 6 months and hard palate at 3 years shows a safe surgical method with acceptable rate of surgical complications and less retracted oral articulation compared to closure of the hard palate at 8 years. However, oral retraction of articulation was noted often or all the time in about 20% of the patients at 5 years of age. The possibility to close the hard palate earlier is thought to be beneficial for speech development and at present the hard palate is routinely closed at 2 years of age. Further follow-up of growth and speech in patients born with oral clefts with different timing and types of surgery is needed.
References
[1] Shi B, Losee JE. The impact of cleft lip and palate repair on maxillofacial growth. Int J Oral Sci. 2015;7(1):14–17. https://doi.org/10.1038/ijos.2014.59
[2] Crowley JS, Friesen TL, Gabriel RA, et al. Speech and audiology outcomes after single-stage versus early 2-stage cleft palate repair. Ann Plast Surg. 2021;86(5 Suppl 3):S360–S366. https://doi.org/10.1097/SAP.0000000000002747
[3] Friede H, Lilja J, Lohmander A. Cleft palate craniofac J. long-term, longitudinal follow-up of individuals with UCLP after the Gothenburg primary early veloplasty and delayed hard palate closure protocol: maxillofacial growth outcome. Cleft Palate Craniofac J. 2012;49(6):649–656. https://doi.org/10.1597/10-252
[4] Johanson B, Lilja J, Friede H. The evolution of the therapeutic approach to cleft lip and palate in Gothenburg. In: Hotz M, Gnoinski W, Perko M, Nussbaumer H, Hof E, Haubensak R, eds. Early Treatment of Cleft Lip and Palate. Toronto: Hans Huber; 1986, pp. 85–89.
[5] Friede H, Lilja J. Dentofacial morphology in adolescent or early adult patient with cleft lip and palate after a treatment regimen that included vomer flap surgery and pushback palatal repair. Scand J Plast Reconstr Hand Surg. 1994;28(2):113–121. https://doi.org/10.3109/02844319409071188
[6] Friede H, Lilja J, Lohmander A, et al. Maxillary dental arch and occlusion in patients with unilateral cleft lip and palate treated with different delays in closure of the hard palate after early velar repair. Scand J Plast Reconstr Surg Hand Surg. 2006;40(5):261–266. https://doi.org/10.1080/02844310600973605
[7] Lilja J, Friede H, Johanson J. Changing philosophy of surgery of the cleft lip and palate in Göteborg, Sweden. In: Berkowitz S, ed. Cleft lip and palate perspectives on management. San Diego, CA: Singular Publishing Group; 1996, pp. 155–170.
[8] Owman-Moll P, Katsaros C, Friede H. Development of the residual cleft in the hard palate after velar repair in a 2-stage palatal repair regimen. J Orofac Orthop. 1998;59:286–300. https://doi.org/10.1007/BF01321795
[9] Randall P, LaRossa D, Fakhraee M, et al. Cleft palate closure at 3 to 7 months of age: a preliminary report. Plast Reconstr Surg. 1983;71(5):624–628. https://doi.org/10.1097/00006534-198305000-00007
[10] Rohrich RJ, Love EJ, Byrd HS, et al. Optimal timing of cleft palate closure. Plast Reconstr Surg. 2000;106(2):413–421; quiz 422; discussion 423–425. https://doi.org/10.1097/00006534-200008000-00026
[11] Lohmander A, Friede H, Lilja J. Long-term, longitudinal follow-up of individuals with unilateral cleft lip and palate after the Gothenburg primary early veloplasty and delayed hard palate closure protocol: speech outcome. Cleft Palate Craniofac J. 2012;49(6):657–671. https://doi.org/10.1597/11-085
[12] Lohmander A, Friede H, Elander A, et al. Speech development in patients with unilateral cleft lip and palate treated with different delays in closure of the hard palate after early velar repair: a longitudinal perspective. Scand J Plast Reconstr Surg Hand Surg. 2006;40(5):267–274. https://doi.org/10.1080/02844310600973621
[13] Willadsen E, Lohmander A, Persson C, et al. Scandcleft randomised trials of primary surgery for unilateral cleft lip and palate: 5. Speech outcomes in 5-year-olds – consonant proficiency and errors. J Plast Surg Hand Surg. 2017;51(1):38–51. https://doi.org/10.1080/2000656X.2016.1254647
[14] Lilja J, Möller M, Friede H, et al. Bone grafting at the stage of mixed dentition in cleft lip and palate patients. Scand J Plast Reconstr Surg Hand Surg. 1987;21(1):73–79. https://doi.org/10.3109/02844318709083583
[15] Friede H, Lilja J, Johanson B. Cleft lip and palate treatment with delayed closure of the hard palate. Scand J Plast Reconstr Hand Surg. 1980;14(1):49–53. https://doi.org/10.3109/02844318009105734
[16] Lohmander A, Persson C. A longitudinal study of speech production in Swedish children with unilateral cleft lip and palate and two-stage palatal repair. Cleft Palate Craniofac J. 2008;45(1):32–41. https://doi.org/10.1597/06-123.1
[17] Mark H, Lilja J. Staged palate repair – soft palate first. In: Hamdan U, Rogers-Vizena C, Vyas M, et al., eds. Interdisciplinary cleft care. Global perspectives. San Diego: Plural publishing inc.; 2022, pp. 327–334.
[18] Rautio J, Andersen M, Bolund S, et al. Scandcleft randomised trials of primary surgery for unilateral cleft lip and palate: 2. Surgical results. J Plast Surg Hand Surg. 2017;51(1):14–20. https://doi.org/10.1080/2000656X.2016.1254646
[19] Lohmander A, Lundeborg I, Persson C. SVANTE – the Swedish Articulation and Nasality Test – normative data and a minimum standard set for cross-linguistic comparison. Clin Linguist Phon. 2017;31(2):137–154. https://doi.org/10.1080/02699206.2016.1205666
[20] Sand A, Hagberg E, Lohmander A. On the benefits of speech-language therapy for individuals born with cleft palate: a systematic review and meta-analysis of individual participant data. J Speech Lang Hear Res. 2022;65(2):555–573. https://doi.org/10.1044/2021_JSLHR-21-00367
[21] Wasserstein RL, Schirm AL, Lazar NA. Moving to a world beyond ‘p < 0.05’. Am Statist. 2019;73:1–19. https://doi.org/10.1080/00031305.2019.1583913
[22] Chapman KL, Hardin-Jones MA, Goldstein JA, et al. Timing of palatal surgery and speech outcome. Cleft Palate Craniofacial J. 2008;45(3):297–308. https://doi.org/10.1597/06-244
[23] Peterson P, Nyberg J, Persson C, et al. Speech outcome and self-reported communicative ability in young adults born with unilateral cleft lip and palate: comparing long-term results after 2 different surgical methods for palatal repair. Cleft Palate Craniofac J. 2022;59(6):751–764. https://doi.org/10.1177/10556656211025926
[24] Havstam C, Sandberg AD, Lohmander A. Communication attitude and speech in 10-year-old children with cleft (lip and) palate: an ICF perspective. Int J Speech Lang Pathol. 2011;13(2):156–164. https://doi.org/10.3109/17549507.2011.514946
[25] Lohmander A, Persson C, Owman-Moll P. Unrepaired clefts in the hard palate: speech deficits at the ages of 5 and 7 years and their relationship to size of the cleft. Scand J Plast Reconstr Surg Hand Surg. 2002;36(6):332–339. https://doi.org/10.1080/028443102321096320
[26] Nyberg J, Havstam C. Speech in 10-year-olds born with cleft lip and palate: what do peers say? Cleft Palate Craniofac J. 2016;53(5):516–526. https://doi.org/10.1597/15-140
[27] Nyberg J, Hagberg E, Havstam C. ‘She sounds like a small child or perhaps she has problems’-peers’ descriptions of speech in 7-year-olds born with cleft palate. Cleft Palate Craniofac J. 2020;57(6):707–714. https://doi.org/10.1177/1055665619890785
[28] Sell D, Southby L, Wren Y, et al. Centre-level variation in speech outcome and interventions, and factors associated with poor speech outcomes in 5-year-old children with non-syndromic unilateral cleft lip and palate: the cleft care UK study. Part 4. Orthod Craniofac Res. 2017;20(Suppl 2):27–39. https://doi.org/10.1111/ocr.12186
[29] Van Lierde KM, Luyten A, Van Borsel J, et al. Speech intelligibility of children with unilateral cleft lip and palate (Dutch cleft) following a one-stage Wardill-Kilner palatoplasty, as judged by their parents. Int J Oral Maxillofac Surg. 2010;39(7):641–646. https://doi.org/10.1016/j.ijom.2010.02.025
[30] Semb G, Enemark H, Friede H, et al. A scandcleft randomised trials of primary surgery for unilateral cleft lip and palate: 1. Planning and management. J Plastic Surg Hand Surg. 2017;51:2–13. https://doi.org/10.1080/2000656X.2016.1263202
[31] Salimi N, Aleksejūnienė J, Yen EH, et al. Fistula in cleft lip and palate patients – a systematic scoping review. Ann Plast Surg. 2017;78(1):91–102. https://doi.org/10.1097/SAP.0000000000000819
[32] Chalien MN, Mark H, Lilja J, et al. Long-term outcome for two-stage palatal closure with different timing of hard palate surgery: craniofacial growth and dental arch relation. Cleft Palate Craniofac J. 2023;Jan 3. https://doi.org/10.1177/10556656221140676
[33] Lohmander A, Lillvik M, Friede H. The impact of early infant jaw-orthopaedics on early speech production in toddlers with unilateral cleft lip and palate. Clin Linguist Phon. 2004;18(4–5):259–284. https://doi.org/10.1080/02699200410001663353
[34] Bessell A, Sell D, Whiting P, et al. Speech and language therapy interventions for children with cleft palate: a systematic review. Cleft Palate Craniofac J. 2013;50(1):e1–e17. https://doi.org/10.1597/11-202