ORIGINAL RESEARCH ARTICLE
Primary and revision artificial urinary sphincter for stress urinary incontinence post-radical prostatectomy: a surgery with high rewards but high risks?
Ingunn Rotha,b, Karin Margrethe Hjellea,b, Charlotte Josefine Johansenb, Christian Arvei Moena,b, Christian Beislanda,b and Patrick Juliebø-Jonesa,b
aDepartment of Urology, Haukeland University Hospital, Bergen, Norway; bDepartment of Clinical Medicine, University of Bergen, Bergen, Norway
ABSTRACT
Objectives: To evaluate the efficacy of artificial urinary sphincter (AUS) implantation in men with stress urinary incontinence post-radical prostatectomy and the complication burden with a focus on identifying potential risk factors for reoperation as well as determining the fate of revision surgeries.
Methods: Retrospective analysis of consecutive patients undergoing primary AUS (pAUS) and revision AUS (rAUS) implantation at a tertiary centre. Logistic regression was employed to identify risk factors for reoperation associated with non-mechanical failures. Kaplan Meier method was applied to generate implant patency curves.
Results: Over 11-years, 108 and 28 patients underwent pAUS and rAUS, respectively. Amongst the former group, a 30-day complication rate of 20.4% was found with a complete (zero pad) dryness rate at follow-up of 49.1%. Post-operative infection was the commonest occurring complication in 7.4%. After pAUS, 27.8% underwent reoperation with cuff erosion being the top indication in 46.7%. Diabetes was a significant predictor for reoperation with an associated 3.6-fold increased risk. The 3-year and 5-year device survival rates without reoperation for pAUS were 80% and 76%, respectively. For rAUS, complete dryness rates achieved were lower at 32.1%. The rate of reoperation was higher at 42.9% with a significantly worse survival probability compared to pAUS (p = 0.024).
Conclusions: Whilst men may achieve complete dryness after pAUS, the potential complication burden and risk of reoperation are not low, and patients need to be counselled regarding this. Chances of continence success are lower when revision surgery is performed with a worse implant survival probability.
KEYWORDS: Artificial urinary sphincter; Stress urinary incontinence; Prostheses and Implants; Surgical outcomes; Prostate cancer
Citation: Scandinavian Journal of Urology 2024, VOL. 59, 185–189. https://doi.org/10.2340/sju.v59.42340.
Copyright: © 2024 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 1 August 2024; Accepted: 23 October 2024; Published: 10 December 2024
CONTACT: Patrick Juliebø-Jones jonesurology@gmail.com Department of Urology, Haukeland University Hospital, Bergen, Norway
Supplemental data for this article can be accessed online at https://doi.org/10.2340/sju.v59.42340
Competing interests and funding: Nil to declare.
Introduction
Stress urinary incontinence (SUI) is one of the core long-term complications associated with radical prostatectomy (RP), and the burden that it renders upon many facets of patients’ lives can be severely debilitating [1–3]. To this end, approximately 3–5% will ultimately undergo incontinence surgery [4, 5]. Whilst alternatives such as slings are available, the artificial urinary sphincter (AUS) has long served as the mainstay intervention [6]. A meta-analysis of 33 studies found that 60% of patients receiving AUS achieved complete symptom relief [7]. Patient satisfaction rates are also high. Linder et al reported that 96% of patients who had undergone AUS would recommend the treatment to a family member [8]. However, despite these merits, the European Association of Urology (EAU) guidelines recommend that clinicians warn potential patients that the risks for both complications and explanation are high [9]. Similarly, the American Urological Association (AUA) guidelines highlight that clinicians should counsel patients that reoperations are common [4]. In a series of 1,082 men undergoing AUS implantation, 31.2% required repeat surgery [10]. It can therefore be argued that despite AUS being established in clinical practice for several decades, there is still a need for more research to better understand, which patients are most at risk of such adverse events in order to optimise patient selection. AUS is also a costly procedure, and therefore further research that can potentially reduce readmissions is also welcomed.
The aim of this study was to evaluate the efficacy of AUS implantation and the complication burden with a focus on identifying potential risk factors for reoperation as well as determining the fate of revision surgeries.
Materials and methods
Retrospective chart review was performed of all patients undergoing AUS implantation between June 2012 and December 2023 at Haukeland University Hospital, a tertiary centre in Western Norway. Only male patients with SUI post-RP were included. Patients with SUI post benign prostate surgery such as transurethral resection of the prostate (TURP) (n = 7) were excluded as they were males with neurogenic SUI (n = 4). To be considered for surgery, men were required to have had persistent SUI for at least 12 months since RP. These men had all been considered in a dedicated post-prostatectomy incontinence pathway where the following investigations were routinely performed: 24-h pad count and weight, frequency volume charts, uroflowmetry, cystoscopy and urodynamic evaluation [11]. In the context of this study, normal urodynamic studies refer to a patient not having any evidence of terminal overactivity and/or reduced compliance. Severity of SUI was graded as follows: mild (1–2 pads/day), moderate (3–5 pads/day) and severe (>5 pads/day). Social continence was defined as use of zero or one pad daily. All patients received AMS 800™ (American Medical Systems, Minnetonka, MN, USA) using a surgical technique that was standardised and has been described previously [12]. The pressure interval of the pressure-regulated ballon was 61–70 cm H2O in all cases. Of note, a perineal approach was employed in all cases. The operation was carried out under general anaesthesia with prophylactic antibiotics. All patients underwent a clinical assessment at 6 weeks post-operatively, where device activation was also performed. Further assessment was carried out at 3 months post-operatively. All patients attended these scheduled follow-up appointments, and there was no loss to follow-up in this regard. Follow-up beyond this was at the discretion of the treating clinician. Reasons included patient wishes, persistent leakage and any complications. Follow-up data concerning any late events associated with the AUS as well as mortality status at the end of the study period were available in all patients.
Data collected included (but was not limited to) age, diabetes mellitus (DM) status and previous radiotherapy (RT). Complete dryness was defined as zero pad usage. AUS implantations were categorised as either primary AUS (pAUS) or revision AUS (rAUS). For all patients in this study undergoing rAUS, this referred to their second AUS surgery, that is, their first revision. In 2012, AUS surgery became regionalised, and therefore, all patients in this study belonged to the Western Norway catchment area. Patients in the rAUS group included patients who had undergone pAUS at either our centre since 2012 or at another centre before the service was regionalised. As a clinical audit, local regulations did not require ethical approval. Patients were not contacted as part of this study. Complications within 30 days were graded according to the Clavien-Dindo system. Logistic regression was employed to identify risk factors for reoperation associated with non-mechanical failures. Kaplan Meier method was applied to generate implant patency curves. The Fischer’s exact test was used to compare continence outcomes according to the RT status. All analyses were performed using R version v4.1.1 [13]. Statistical significance was determined at p < 0.05.
Results
Patient characteristics
Over the 11-year study period, 136 patients underwent AUS implantation (primary: 108, revision: 28). Six different primary surgeons performed the implantations. In the pAUS group, the median age at time of RP and subsequent implantation were 64 years (interquartile range [IQR]: 62–68) and 69 years (IQR: 64–72), respectively. Median follow-up time was 80 months (IQR: 48–99 months) in the pAUS group, and 65 months (35–76) in the rAUS group. A history of RT was recorded in 37 patients (34.3%). Nine of the patients (8.3%) had undergone previous sling surgery. Median age at the time of the original prostate surgery and subsequent implantation was 64 years (IQR: 62–68) and 69 years (IQR: 64–72), respectively. The majority of patients (85.2%, n = 92) in the pAUS group had normal urodynamic studies. Most patients had either moderate (44.4%) or severe (41.7%) SUI (Table 1).
Operative data
The median operative time for pAUS was 59 min (IQR: 52–69). The most commonly used AUS cuff size was 4.5 cm (58.3%), followed by 4.0 cm (30.6%) (Supplementary Table 1). Only one in 10 patients stayed beyond one night in hospital after the operation.
Follow-up, complications and reoperation
In the pAUS group, 49.1% reported complete dryness, whilst 85.2% were socially continent. The early (within 30 days) complication rate was 20.4%. Post-operative infection (CDII) was the most commonly occurring complication in 7.4% (Table 2). No mortalities were recorded.
| n (%) | Management | |
| Early complications | 22 (20.4) | |
| Grade I | ||
| Scrotal hematoma | 5 (4.6) | Conservative treatment |
| Pain | 1 (0.9) | Conservative treatment |
| Grade II | ||
| Infection* | 8 (7.4) | Peroral antibiotics |
| Grade III | ||
| Acute urinary retention | 6 (5.6) | Suprapubic cystotomy catheter placement |
| Scrotal hematoma | 1 (0.9) | Scrotal hematoma removal |
| Grade IIIb | ||
| Infection | 1 (0.9) | AUS removal |
| *Grade II Infection: registered 1 pneumonia, 4 superficial wounds infections, 2 UTI and 1 epididymitis. UTI: urinary tract infection; AUS: artificial urinary sphincter. |
||
The overall rate of reoperation in the pAUS group was 27.8%, and most were due to non-mechanical failures (83.3%). The top indication was cuff erosion in 46.7%. Device explanation was required in 20.4% (Table 3). When considering early complications and reoperations, 47.2% experienced some kind of adverse advent.
Based on multivariable analysis (Table 4), DM was a significant predictor for reoperation with an associated 3.6-fold increased risk. However, none of the following was identified as significant predictors of reoperation: age, body mass index, history of RT, smoking and SUI grade. In addition, RT had no significant impact on continence outcomes (Supplementary table 2). The 3-year and 5-year device survival rates without reoperation for pAUS were 80% and 76%, respectively (Figure 1). Stratified by DM status, implant survival probability was significantly worse in those affected (p = 0.0033) (Supplementary figure 1).
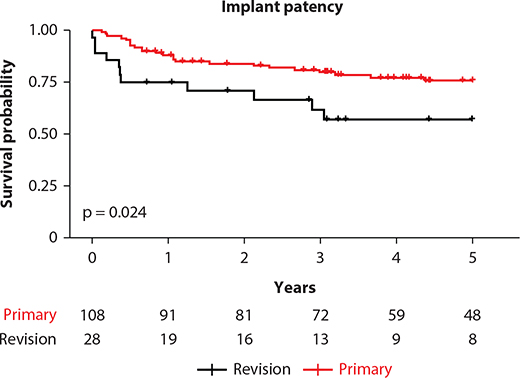
Figure 1. Kaplan-Meier survival analysis of implant stratified by primary versus revision surgery.
At 3 years post-surgery, 72 patients were still at risk of losing the implant or at risk of death in the pAUS group, whilst at 5 years post-surgery, there were 48 patients (Figure 1). In the rAUS group, out of 28 who underwent surgery, there were 13 patients at 3 years post-surgery and 8 at 5 years post-surgery, who were still alive and still had their implant in situ. By the end of the period, 15 patients in total had died of medical causes unrelated to their incontinence surgery.
Outcomes of revision AUS
Complete dryness rates achieved were lower compared to pAUS at 32.1%, and overall, 46.4% achieved social continence. These results were not significantly inferior to the pAUS group. The early complication rate was 17.9%, and the rate of reoperation was higher at 42.9%. The 3-year and 5-year device survival rates without reoperation for rAUS were 62% and 57%, respectively (Figure 1). Survival probability was significantly worse in the rAUS group (p = 0.024).
Discussion
Key findings
In this study, nearly one in two men achieved complete dryness when undergoing pAUS for SUI post-RP. However, nearly the same proportion suffered some kind of adverse event at some point after their surgery. Furthermore, revision surgery delivers lower odds of achieving dry status whilst carrying a higher risk of reoperation and a significantly worse probability of device survival. Patients therefore need to be counselled carefully regarding the chances of treatment success and the risk of complications in both primary and revision AUS settings but especially the latter. Patients’ expectations need to be managed accordingly.
Shaw et al performed a qualitative study of men who had undergone incontinence surgery [14]. One of the main themes identified was how men regretted how they had delayed seeking treatment and would have undergone the surgery earlier. The authors also found that patients often placed more emphasis on outcomes such as sexual function as being important rather than dryness [14]. Hampson et al studied the perspectives of a cohort of men who had attended a male SUI clinic [15]. Men who had elected not to have incontinence surgery recorded significantly higher levels of regret compared to those who had elected to undergo AUS (34.7% vs. 8.2%, p < 0.001). Treatment satisfaction does therefore appear to be high. From another perspective, it may also highlight that SUI post-RP impedes quality of life so much, and that regardless of potential complications, patients still deem the surgery to be worth it, in order to improve continence status. Of note, in another study, Dunbar et al found that amongst men who have experienced revision/explant, they do report significantly higher levels of decisional regret regarding having had incontinence surgery [16].
There is discordance in the literature regarding the impact of RT on both complication burdens and degree of continence improvement associated with AUS implantation as well as sling surgeries [17, 18]. Numerous studies have shown that RT does influence these outcomes, and this does seem logical, given the associated pernicious sequelae in terms of tissue vascularity and fibrosis [19]. DM can have similar detrimental effects on small vessel function, and Viers et al reported it to yield a 2.3-fold increased risk of erosion or infection in their 90-patient series [20]. Our study mirrored those findings and found an even higher risk when considering non-mechanical failures.
Ventimiglia et al reported that whilst the number of RPs being performed in Sweden between 2000 and 2014 had increased threefold, the number of incontinence surgeries performed had increased eightfold [5]. The demand for incontinence surgeries appears therefore to be increasing. As countries like Norway experience a growing elderly demographic as well as a general increased awareness of the importance of continence in terms of quality of life, this demand will likely increase further. Understanding complication burdens that can help guide patients to select a surgical option that is best suited for their individual needs is crucial.
Since AUS was introduced to clinical practice several decades ago, there have been relatively few modifications to the device itself. In terms of future prospects, an electronically activated AUS has been studied at an experimental level [21], and adjustable AUS devices have also been described in pilot clinical setting [22]. Surgical technique for AUS has been studied over time. Most recently, in a multicentre French study, no difference in complications was found when a penoscrotal approach was compared with perineal [23]. Sacco et al also recently reported their experiences with a novel albugineal technique [24].
Limitations in this study include the retrospective design, single centre status and lack of subjective outcome measures to determine, for example, patient satisfaction. Another limitation to acknowledge is that patients who underwent surgery later in the study period had a shorter follow-up, and therefore, potential late complications would not be captured. However, the study is strengthened by not pooling patients with different aetiologies of SUI. Furthermore, patients undergoing primary and revision AUS implantation have been differentiated and not pooled as is also found in numerous studies. It is also, to our knowledge, the first study of its kind evaluating outcomes of pAUS and rAUS from Norway.
Conclusion
In men with SUI post-RP, AUS implantation can deliver high chance of achieving either zero pad usage or one pad only. However, this is matched by the potential for early complications and/or reoperation. The latter is even higher when undergoing revision surgery. The probability of an implant surviving is worse when repeat surgery is performed. DM was identified as a significant risk factor for reoperation. Careful case selection as well as clear patient communication is therefore key when considering potential incontinence surgery.
Data availability statement
The datasets generated and/or analysed during the current study are available from the corresponding author upon reasonable request.
Ethical approval
As a clinical audit, local regulations did not require ethical approval.
References
- Hoyland K, Vasdev N, Abrof A, et al. Post-radical prostatectomy incontinence: etiology and prevention. Rev Urol. 2014;16(4):181–188.
- Katsimperis S, Juliebø-Jones P, Ta A, Tandogdu Z, Al-Bermani O, Bellos T, Esperto F, Tonyali S, Mitsogiannis I, Skolarikos A, Varkarakis I, Somani BK, Tzelves L. Surgical techniques to preserve continence after robot-assisted radical prostatectomy. Front Surg. 2023 Nov 3;10:1289765. https://doi.org/10.3389/fsurg.2023.1289765. PMID: 38026481; PMCID: PMC10655003
- Bernardes M, Chagas SC, Izidoro LCR, et al. Impact of urinary incontinence on the quality of life of individuals undergoing radical prostatectomy. Rev Lat Am Enfermagem. 2019;27:e3131. https://doi.org/10.1590/1518-8345.2757.3131
- Sandhu JS, Breyer B, Comiter C, et al. Incontinence after prostate treatment: AUA/SUFU guideline. J Urol. 2019;202(2):369–378. https://doi.org/10.1097/JU.0000000000000314
- Ventimiglia E, Folkvaljon Y, Carlsson S, et al. Nationwide, population-based study of post radical prostatectomy urinary incontinence correction surgery. J Surg Oncol. 2018;117(2):321–327. https://doi.org/10.1002/jso.24816
- Ameli G, Chartier-Kastler EJ, Anding RG, et al. Artificial urinary sphincters in males and females and neurogenic patients, techniques, and indications. Continence Rep. 2023;6:100028. https://doi.org/10.1016/j.contre.2023.100028
- Chen YC, Lin PH, Jou YY, Lin VC. Surgical treatment for urinary incontinence after prostatectomy: a meta-analysis and systematic review. PLoS One. 2017;12(5):e0130867. https://doi.org/10.1371/journal.pone.0130867
- Smith WJ, VanDyke ME, Venishetty N, et al. Surgical management of male stress incontinence: techniques, indications, and pearls for success. Res Rep Urol. 2023;15:217–232. https://doi.org/10.2147/RRU.S395359
- Gravas S, Cornu J, Gacci M, et al. EAU Guidelines on management of non-neurogenic male LUTS including benign prostatic obstruction. European Association of Urology: Arnhem, The Netherland; 2022.
- Linder BJ, Rivera ME, Ziegelmann MJ, et al. Long-term outcomes following artificial urinary sphincter placement: an analysis of 1082 cases at Mayo Clinic. Urology. 2015;86(3):602–607. https://doi.org/10.1016/j.urology.2015.05.029
- Roth I, Juliebo-Jones P, Arvei Moen C, et al. Outcomes with the Adjustable Transobturator Male System (ATOMS) for the treatment of male stress urinary incontinence after prostate surgery and the impact of previous radiotherapy. Eur Urol Open Sci. 2024;62:68–73. https://doi.org/10.1016/j.euros.2024.02.016
- Brant WO, Martins FE. Artificial urinary sphincter. Transl Androl Urol. 2017;6(4):682–694. https://doi.org/10.21037/tau.2017.07.31
- R Core Team R. R: a language and environment for statistical computing [Internet]. R Found. Stat. Comput; 2017 [cited 2022 Sep 20]. Available from: http://www.r-project.org/
- Shaw NM, Nik-Ahd F, Jones C, et al. Patient decision-making for surgical treatment of post-prostatectomy stress urinary incontinence: a mixed-methods exploratory pilot study. Transl Androl Urol. 2023;12(5):849–858. https://doi.org/10.21037/tau-22-618
- Hampson LA, Suskind AM, Breyer BN, et al. Predictors of regret among older men after stress urinary incontinence treatment decisions. J Urol. 2022;207(4):885–892. https://doi.org/10.1097/JU.0000000000002352
- Dunbar A, Heinlen J, Slobodov G, et al. Application of the decisional regret scale (DRS) in men undergoing anti-incontinence procedures for stress urinary incontinence. Transl Androl Urol. 2023;12(9): 1408–1415. https://doi.org/10.21037/tau-23-105
- Juliebo-Jones P, Roth I, Tzelves L, et al. Current status of the adjustable transobturator male system (ATOMS(TM)) for male stress urinary incontinence. Front Surg. 2024;11:1377788. https://doi.org/10.3389/fsurg.2024.1377788
- Bhatt NR, Pavithran A, Ilie C, Smith L, Doherty R. Post-prostatectomy incontinence: a guideline of guidelines. BJU Int. 2024 May;133(5):513-523. https://doi.org/10.1111/bju.16233. Epub 2023 Dec 13. PMID: 38009420
- Mamane J, Sanchez S, Lellouch AG, et al. Impact of radiation therapy on artificial urinary sphincter implantation in male patients: a multicenter study. Neurourol Urodyn. 2022;41(1):332–339. https://doi.org/10.1002/nau.24825
- Viers BR, Linder BJ, Rivera ME, et al. The impact of diabetes mellitus and obesity on artificial urinary sphincter outcomes in men. Urology. 2016;98:176–182. https://doi.org/10.1016/j.urology.2016.06.038
- Biardeau X, Hached S, Loutochin O, et al. Montreal electronic artificial urinary sphincters: our futuristic alternatives to the AMS800. Can Urol Assoc J. 2017;11(10):E396–E404. https://doi.org/10.5489/cuaj.4493
- Weibl P, Hoelzel R, Rutkowski M, et al. VICTO and VICTO-plus – novel alternative for the mangement of postprostatectomy incontinence. Early perioperative and postoperative experience. Cent Eur J Urol. 2018;71(2):248–249.
- Bernard C, Bentellis I, El-Akri M, et al. Primary implantation of an artificial urinary sphincter using the perineal and penoscrotal approaches: functional results and assessment of reoperative procedures. Fr J Urol. 2024;34(3):102604. https://doi.org/10.1016/j.fjurol.2024.102604
- Sacco E, Marino F, Gandi C, Bientinesi R, Totaro A, Moretto S, Gavi F, Campetella M, Racioppi M. Transalbugineal Artificial Urinary Sphincter: A Refined Implantation Technique to Improve Surgical Outcomes. J Clin Med. 2023 Apr 21;12(8):3021. https://doi.org/10.3390/jcm12083021. PMID: 37109357; PMCID: PMC10141998