ORIGINAL RESEARCH ARTICLE
Quadratus lumborum block is feasible alternative to epidural block for postoperative analgesia after open radical cystectomy: surgical and oncological outcomes of a randomised clinical trial
Erik Veskimäea,b*, Andrus Korgveeb,c*, Heini Huhtalad, Heikki Koskinenb,c, Maija-Liisa Kalliomakib,c, Teuvo Tammelaa,b and Eija Junttilab,c
aDepartment of Urology, Tampere University Hospital, Tampere, Finland; bFaculty of Medicine and Health Technology, Tampere University, Tampere, Finland; cDepartment of Anaesthesia, Tampere University Hospital, Tampere, Finland; dFaculty of Social Sciences, Tampere University, Tampere, Finland
ABSTRACT
Objective: The current lack of standardised perioperative pain management protocols for open radical cystectomy (ORC) underscores the need for alternative approaches to the longstanding tradition of epidural block. The aim of this study was to assess the impact of bilateral single injection quadratum lumborum block (QLB) on patients’ recovery and complication rates compared with epidural analgesia after ORC in a single-centre, randomised, parallel-group trial including adult patients with bladder cancer.
Material and methods: Consecutive ORC patients were randomly allocated into QLB and the epidural group. The primary endpoint of this study was related to opioid consumption, and the results have been published earlier. This report focuses on secondary outcomes.
Results: This study included a total of 41 patients, with 20 patients in the QLB group and 21 patients in the epidural group. Finally, 39 patients were included in the analysis.
There was a trend for more frequent need for postoperative norepinephrine and fluid support in the epidural group but without statistical significance. Postoperative complication rate was similar. Two patients in the epidural group compared to none in the QLB group were rehospitalised within 30 and 90 days. Mortality rate within 90 days was higher in the epidural group (4 vs. 0 patients, P = 0.064).
Conclusions: In this trial, there were no significant differences in surgical and oncological outcomes after ORC when QLB is compared with epidural block for postoperative analgesia.
Trial registration: ClinicalTrials.gov Identifier: NCT03328988
KEYWORDS: Bladder cancer; radical cystectomy; epidural analgesia; quadratum lumborum block
Citation: Scandinavian Journal of Urology 2025, VOL. 60, 59–65. https://doi.org/10.2340/sju.v60.43105.
Copyright: © 2025 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 24 October 2024; Accepted: 3 February 2025; Published: 13 March 2025
CONTACT: Erik Veskimäe erikveskimae@gmail.com Department of Urology, Tampere University Hospital PO Box 2000, 33521 Tampere, Finland
*These authors contributed equally to this work.
Competing interests and funding: The authors have no relevant financial or non-financial interests to disclose.
This work was supported by Grant of Finnish Cancer Foundation.
Introduction
Radical cystectomy (RC) is the method of choice to treat high-risk non-metastatic bladder cancer (BC) [1]. As BC is commonly affecting the elderly and patients with comorbidities, more than half of the patients undergoing open radical cystectomy (ORC) face complications of all grades [2]. Recovery from major surgery depends on multiple factors that at best can be handled by continuously redesigning perioperative management based on updated evidence [3].
Enhanced recovery protocol (ERAS) as part of RC has proven to reduce hospital stay (length of stay [LOS]) and re-admission rates [4]. Encouraging results about ERAS were first seen in patients after colorectal surgery [5, 6]. Perioperative thoracic epidural anaesthesia continues to play crucial role in enhancing clinical outcomes [7, 8]. This is attributed not only to its superior pain management but also to its ability to reduce the postoperative stress response, promote quicker recovery of the bowel function and lower rates of postoperative complications and mortality [9–12]. Still, due to the differences between gastrointestinal and urinary tract surgery, not all of ERAS components are suitable for ORC patients. Notable is, contrary to colorectal surgery, regional (spinal/epidural) analgesia as part of the ERAS protocol during and after ORC appears to be an independent factor for prolonged LOS [13].
Epidural analgesia has long been the golden standard for pain management in abdominal surgery [14]. In addition to reducing the postoperative consumption of opioids, positive effects of epidural analgesia compared to oral analgesia are promoting gastrointestinal recovery [15], reduced cardiovascular effects [16] and improved lung function [17]. On contrary, epidural use at time of RC has been shown to be associated with elevated risk of perioperative complications, hospital re-admission and longer hospitalisation [18].
Ultrasound-guided truncal block, quadratum lumborum block (QLB), has proven to reduce postoperative opioid consumption and to diminish postoperative nausea and vomiting after abdominal and hip surgery. Furthermore, QLB appears to be a safe procedure [19]. To date, there are no studies evaluating the feasibility of QLB in ORC patients.
We have previously reported the outcomes for postoperative analgesia of this randomised controlled trial, in which opioid consumption did not differ between bilateral single shot posterior QLB and an epidural infusion [20]. The aim of this study is to present the data from our randomised study comparing a bilateral single injection posterior QLB compared to an epidural block with aspects of enhanced bowel recovery, shorter LOS and reductions in complication rates.
Materials and methods
Study design and participants
This randomised controlled trial was conducted in a university-affiliated tertiary hospital from April 2017 to August 2020. The protocol had been approved by the Regional Ethics Committee of Tampere University Hospital (approval number: R17008). Consecutive patients with high-risk BC scheduled to ORC were recruited. This study adhered to CONSORT guidelines [21]. Written informed consents were obtained from all patients.
Eligible participants were BC patients, aged 18–85 years, scheduled for ORC, pelvic lymph node dissection and urinary diversion.
Exclusion criteria were complicated diabetes mellitus type 1, inadequate cooperation skills and chronic pain due to other cause than BC.
Randomisation
Participants were randomised into two groups. Randomisation was conducted in a block size of 10 using a computerised randomisation sequence by independent research assistant. The randomisation allocation number for each subject was written on paper and concealed in an opaque envelope. The envelope was opened by the anaesthesiologist who was appointed to perform epidural or QLB procedure. Blinding care givers and patients was not possible as analgetic procedures were technically different. Patients in the intervention group received QLB. Control group received continued epidural analgesia.
Perioperative care
General perioperative anaesthesiologic protocol was conducted and followed, and details are reported previously [20]. The technique of both bilateral US-guided single injection posterior QLB and epidural block is described elsewhere [20]. An epidural catheter was placed preoperatively before anaesthesia induction. Bilateral US-guided posterior QLB was performed before emergency from anaesthesia. All blocks were performed by highly experienced anaesthesiologists (A.K. and M-L.K.)
Operation technique was standardised and performed through infraumbilical incision. In males, cystoprostatectomy included also the removal of the seminal vesicles, and in female patients, RC included the removal of uterus, fallopian tubes and anterior vaginal wall, when necessary. Pelvic lymph node dissection included obturator and internal and external iliac chains to the level of the ureteric crossing of the common iliac artery. Bricker technique was used for incontinent ileal conduit, and the Studer method for a neobladder.
Postoperatively, on day 0, patients were moved to general urological ward and were treated based on the ERAS protocol. In short, on day 1, patients were allowed chewing gum and clear oral fluids and were encouraged to sit out of bed and to stand/walk. Light diet was introduced as soon as patient passed flatus, and normal diet soon after. In case of vomiting, nasogastric tube was recommended. Patients were discharged as soon as they managed without external assistance, had resumed full diet and managed with their stoma by themselves.
Outcome measures
The primary endpoint was related to postoperative cumulative rescue opioid consumption and is reported elsewhere [20].
Secondary outcomes included the following: postoperative length of in-hospital stay (LOS), recovery from surgery (days from surgery to oral fluids and solid food, flatus, bowel movement, ability to sit, stand and walk <10 and >10 m after the surgery), surgical complications during the in-hospital stay (Clavien-Dindo classification), re-admission rates <30 and < 90 days postoperatively and mortality rate <90 days postoperatively.
Prospectively collected baseline characteristics included data about patients age, gender, body mass index (BMI), ASA physical status index, neoadjuvant chemotherapy (yes/no), pathological stage, lymph node (LN) dissection template, LN count and number of LN positive cases; urinary diversion (ileal conduit; neobladder); surgical time (min); blood loss during the operation and in the recovery room (mL); fluid infusion during the surgery and in the recovery room (mL); need for noradrenalin infusion in the recovery room (yes/no).
Statistical analysis
This report focuses on secondary outcomes of the randomised trial. The primary objective was a cumulative opioid consumption during the first 24 h postoperatively. Sample size calculation was made based on primary outcome and is reported elsewhere [20]. Based on the power of 0.8 and a type I probability of 0.05, the calculated sample size for each group was 18 patients. However, to account for potential dropouts or incomplete data, a sample size of 22 patients per group was chosen for this study.
Mean or medians were calculated for all the quantitative variables. Normality of the data was reviewed using the Shapiro–Wilk test. Normally distributed continues variables were reported with mean and standard deviations. The rest of the continuous variables were summarised by their median values and ranges.
For normally distributed data, means of two groups were compared using the Student’s t-test. For skewed data, the Mann–Whitney U-test was applied. Two tailed P-values were reported, and statistical significance was set at a P-value of less than 0.05. Qualitative or categorical variables were described as frequencies and proportions. Statistical analysis was conducted using SPSS Version 26 (IBM Corporation, Armonk, NY).
Results
Study population
Study participant flow and reasons for exclusion are presented in Figure 1. Overall, 41 patients met the study criteria, signed the informed consent and were randomised to take part in this study. The participants were randomly assigned into two groups and underwent ORC followed by urinary diversion. Two patients were excluded for further analysis: the recorded data had not been saved in one patient and one of the recruited patients had an inoperable BC. In total, 39 patients were finally analysed, 20 patients in the intervention group and 19 patients in the control group (Figure 1).
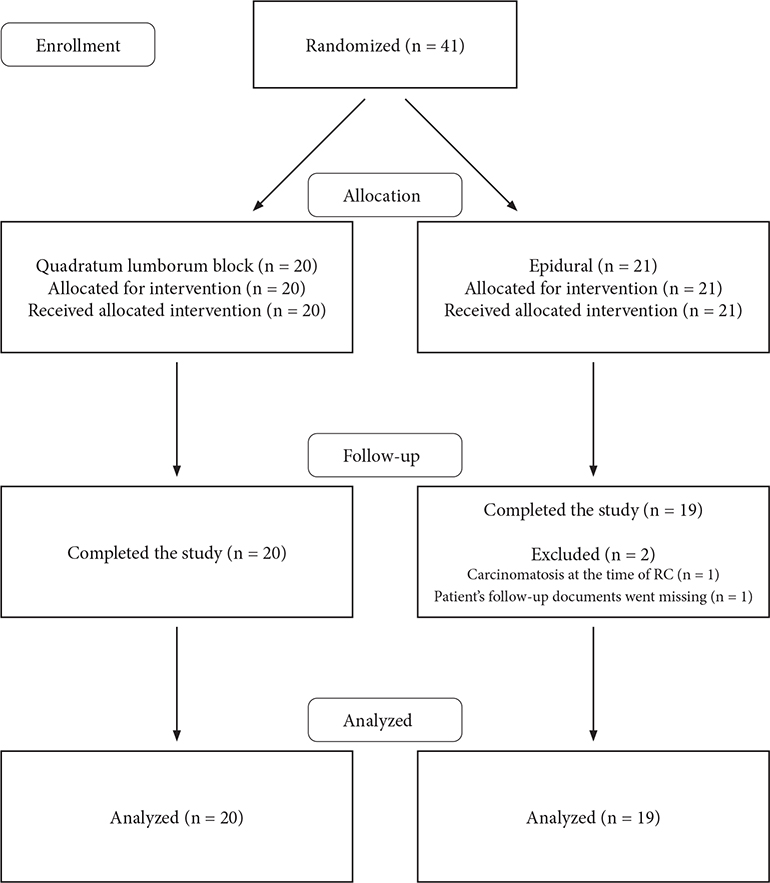
Figure 1. The flowchart of the study
Participants and perioperative details
Baseline and intraoperative characteristics of the two groups were similar, except gender distribution (P = 0.031) (Table 1).
Surgical approach was similar in male patients but varied in female patients. Decision about surgical range was based on patients’ preferences, clinical T-stage and previous operations. Gynaecological organs (incl. removal of the uterus, salpingo-oophorectomy and resection of anterior vaginal wall) were removed from two patients in the epidural group. Isolated salpingo-oophorectomy was done in one patient from both groups. Pelvic organ-preserving cysto-urethrectomy was done for five patients in the epidural group and one patient in the QLB group.
Patients in both groups had similar perioperative treatment in respect of neoadjuvant chemotherapy and lymph node dissection (dissection template and lymph node count) and urinary diversion. Furthermore, surgical time and blood loss during surgery and in the recovery room were comparable. Based on our anaesthesiologic protocol, patients received similar amount of fluids during the surgery. Patients with epidural analgesia tended, but not statistically significantly, to receive more fluids in the recovery room (mean [SD] 1,257 [825.1] mL vs. 1,573 [1115.9] mL in QLB vs. epidural, respectively; P = 0.509). Patients with epidural block were more dependent on noradrenalin infusion in the recovery room (10% vs. 37% of patients, P = 0.065). No other side-effects of QLB or epidural block were recorded.
Pathological tumour stage being similar in both groups, and the only statistically significant difference identified was related to lymph node metastasis, as 35% (7/20) of patients in the QLB group versus 5% (1/19) in the epidural cohort had metastatic disease (P = 0.044).
Postoperative outcomes
Postoperative outcomes are summarised in Table 2 and Figure 2 Patients in the QLB group showed slightly faster recovery by means of earlier oral fluids intake (postoperative day [POD] 3.8 vs. 4.2, P = 0.147) and bowel movement (POD 6.2 vs. 7, P = 0.237), although differences were not statistically significant. There was no significant difference in mobilising patients or in nausea and vomiting between the two groups. The in-hospital stay was slightly longer for the epidural group, but the difference was not significant (12 vs. 10 days, P = 0.932).
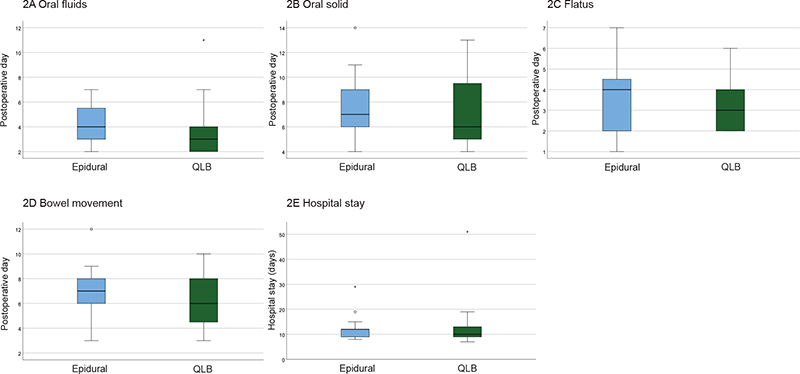
Figure 2. Postoperative recovery during hospital stay after open radical cystectomy
Postoperative complication rate was similar, and the Clavien-Dindo 3–5 complication rate was low in both cohorts. In the QLB cohort, one patient had an angiovascular treatment for lower-extremity arterial embolus, and one patient had a fistula that was operated. In the epidural group, one patient died due to aspiration pneumonia. The re-hospitalisation rate within 30 days of the surgery was higher in the epidural group (2 vs. 0, P = 0.106) and similar within 90 days postoperatively. The mortality rate within 90 days was worse in the epidural cohort, with four patients died compared to none in the QLB group (P = 0.064). One patient died due to aspiration pneumonia, whilst three patients due to a rapid course of the disease with different T-stages in RC specimen (one patient with T4-stage, second patient T3-stage and the third patient T4b-stage with lymph node metastases). However, these differences in mortality rates were not statistically significant.
Discussion
This prospective randomised trial demonstrated feasibility of bilateral single injection QLB as an alternative to continuous epidural block in respect of adequate pain management after ORC [20] without compromising postoperative recovery. This study is the first to compare the effects of QLB with epidural block in this patient group.
Open radical cystectomy, being a large pelvic surgical procedure, requires sufficient peri- and postoperative analgesia. The method of analgesia used can affect various outcomes such as patient recovery, complication rate, LOS and oncological outcomes [18]. This prompted us to test the impact of bilateral single injection QLB on above-mentioned outcomes compared with continuous epidural block. The primary goal of this study was to assess the efficacy of QLB in postoperative analgesia with these patients. These encouraging results of this study are reported elsewhere [20].
The patients in our study were elderly (with a median age of 74 years) and with generally high ASA class. Almost 70% had ASA class 3–4 in the QLB group versus 74% in the epidural group. Hence, our patients were older and with a high er ASA-class compared to other centres [22]. Despite that, the recovery from ORC was comparable to what has been reported elsewhere in the literature [23]. This study was able to show a trend towards enhanced postoperative bowel movement, reduced complication rate and shorter LOS in the QLB group compared to patients having continuous epidural analgesia. Although none of these outcomes were significantly better than those observed in patients with continuous epidural analgesia, QLB appears to be an excellent alternative to continuous epidural block. Compared to the literature, the re-admission rate in both groups was very low. Miller et al. found in a population-based study that patients with epidural analgesia had a longer LOS, increased 30-day re-admission rate and decreased likelihood of being discharged directly at home compared to omitting epidural block [18]. Similarly, Williams et al. reported in their individual patient data meta-analysis that local anaesthetic blocks compared with spinal/epidural analgesia shortened the LOS [23]. Rahman et al. conducted a systematic review about the effect of epidural analgesia compared to opiate-based analgesia on short- and long-term outcomes after RC [24]. Finally, only nine studies were included, and eight of them were retrospective cohorts. They found that the evidence related to the perioperative analgesia is poor, and that postoperative complications are more frequent when incorporating epidural block. Additionally, the potential role of local blocks was discussed referring to the encouraging results by Matulewicz et al. In their recent study, Transversus Abdominal Plane Block was used as part of a ERAS protocol, and as a result, an LOS reduction was 1.5 days [25]. Although Burkhard et al., in their recent matched cohort study involving 44 patients, demonstrated the possibility of enhancing epidural block outcomes by avoiding opioids, they still recognise the potential advantages of local blocks over epidural block [26].
Vasodilatation-related hypotension is a well-known side-effect of epidural block. In the control cohort of this study, this effect was observed in the recovery room where patients required more noradrenalin support and parenteral fluids. This could explain the slightly slower bowel recovery observed in patients with continuous epidural analgesia. Postoperative ileus is a common complication after RC [27]. Although the intraoperative restricted fluid therapy approach on bowel recovery has shown promise, the results are still inconclusive [28–30].
In addition, patients in the epidural cohort had higher mortality rate, although patients in the QLB group had similar tumour stage and higher prevalence of lymph node metastases (35% vs. 5%, respectively). The absence of power calculation clearly limits the reliability of the observed differences in lymph node metastasis prevalence, method of analgesia and their potential impact on survival or disease progression. Although epidural use at the time of abdominal surgery has shown improved cancer outcomes, there are limited data about the impact in RC and the oncological outcomes of BC [18]. Miller et al. found in a large population-based analysis that epidural analgesia did not improve cancer specific or overall survival and questioned the benefits of epidural block in this group of patients [18].
This study has several limitations that should be taken into consideration when interpreting the results.
First, this study was conducted at a single tertiary medical centre, which may limit the generalisability of the findings. Second, this study was terminated before reaching the initially planned sample size. Specifically, the sample size calculation for this study was based on the need for cumulative rescue opioid consumption (primary outcome), and this study was terminated before reaching the sample size goal but still achieved the lower limit. Furthermore, the recruitment period would have been extended if it were not for the change in operation technique from ORC to robotic RC in our hospital. Third, the blocks were performed by highly experienced anaesthesiologists. Different practitioners may have slightly different techniques, which could affect the consistency and standardisation of the blocks. Fourth, there was a statistically significant difference in gender distribution between the study groups, but it is in line with the typical gender distribution of BC and unlikely to affect the results. Furthermore, epidural block was established without epidural opioid, which may have diminished its effectiveness. These factors may limit the generalisability of the study’s finding.
Conclusion
The results of this randomised trial indicate that bilateral quadratum lumborum single injection block is the feasible alternative to continuous epidural analgesia by providing similar postoperative analgesia and trend towards enhanced recovery from surgery.
Authors’ contribution
E. Veskimäe: Protocol/project development, Data collection or management, Data analysis, Manuscript writing/editing.
A. Korgvee: Protocol/project development, Data collection or management, Data analysis, Manuscript writing/editing.
H. Huhtala: Data analysis, Manuscript writing/editing.
Heikki Koskinen: Data analysis, Manuscript writing/editing.
M.-L. Kalliomäki: Protocol/project development, Manuscript writing/editing.
T. Tammela: Protocol/project development, Manuscript writing/editing.
E. Junttila: Protocol/project development, Data collection or management, Data analysis, Manuscript writing/editing.
References
- [1] Witjes JA, Babjuk M, Horwich A, et al. EAU-ESMO consensus statements on the management of advanced and variant bladder cancer – an international collaborative Multistakeholder effort†: Under the auspices of the EAU-ESMO guidelines committees. Eur Urol. 2020;77(2):223–250. https://doi.org/10.1016/j.eururo.2019.09.035
- [2] Shabsigh A, Korets R, Donat SM, et al. Defining early morbidity of radical cystectomy for patients with bladder cancer using a standardized reporting methodology. Eur Urol. 2009;55(1):164–174. https://doi.org/10.1016/j.eururo.2008.07.031
- [3] Matulewicz RS, Brennan J, Meeks JJ, et al. Radical cystectomy perioperative care redesign. Urology. 2015;86(6):1076–1086. https://doi.org/10.1016/j.urology.2015.09.001
- [4] Pang KH, Groves R, Catto JWF, et al. Prospective implementation of enhanced recovery after surgery protocols to radical cystectomy. Eur Urol. 2018;73(3):363–371. https://doi.org/10.1016/j.eururo.2017.07.031
- [5] Lohsiriwat V. Enhanced recovery after surgery vs conventional care in emergency colorectal surgery. World J Gastroenterol. 2014;20(38):13950. https://doi.org/10.3748/wjg.v20.i38.13950
- [6] Varadhan KK, Neal KR, Lobo DM, et al. The enhanced recovery after surgery (ERAS) pathway for patients undergoing major elective open colorectal surgery: a meta-analysis of randomized controlled trials. Clin Nutr. 2010;29(4):434–440. https://doi.org/10.1016/j.clnu.2010.01.004
- [7] Feldheiser A, Aziz O, Carli F, et al. Enhanced recovery after surgery (ERAS) for gastrointestinal surgery, part 2: consensus statement for anaesthesia practice. Acta Anaesthesiol Scand. 2016;60(3):289–334. https://doi.org/10.1111/aas.12651
- [8] Scott MJ, Baldini G, Carli F, et al. Enhanced recovery after surgery (ERAS) for gastrointestinal surgery, part 1: pathophysiological considerations. Acta Anaesthesiol Scand. 2015;59(10):1212–1231. https://doi.org/10.1111/aas.12601
- [9] Block BM, Liu SS, Wu CL, et al. Efficacy of postoperative epidural analgesia: a meta-analysis. JAMA. 2003;290(18):2455. https://doi.org/10.1001/jama.290.18.2455
- [10] Pöpping DM, Elia N, Tramer MR, et al. Impact of epidural analgesia on mortality and morbidity after surgery: systematic review and meta-analysis of randomized controlled trials. Ann Surg. 2014;259(6): 1056–1067. https://doi.org/10.1097/SLA.0000000000000237
- [11] Ahlers O, Nachtigall I, Keh D, et al. Intraoperative thoracic epidural anaesthesia attenuates stress-induced immunosuppression in patients undergoing major abdominal surgery. Br J Anaesth. 2008;101(6):781–787. https://doi.org/10.1093/bja/aen287
- [12] Freise H, Van Aken HK. Risks and benefits of thoracic epidural anaesthesia. Br J Anaesth. 2011;107(6):859–868. https://doi.org/10.1093/bja/aer339
- [13] Daneshmand S, Ahmadi H, Djaladat H, et al. Enhanced recovery protocol after radical Cystectomy for Bladder Cancer. J Urol. 2014;192(1):50–56. https://doi.org/10.1016/j.juro.2014.01.097
- [14] Weiss R, Pöpping DM. Is epidural analgesia still a viable option for enhanced recovery after abdominal surgery. Curr Opin Anaesthesiol. 2018;31(5):622–629. https://doi.org/10.1097/ACO.0000000000000640
- [15] Freise H, Fischer LG. Intestinal effects of thoracic epidural anesthesia. Curr Opin Anaesthesiol. 2009;22(5):644–648. https://doi.org/10.1097/ACO.0b013e32832eb7e8
- [16] Rodgers A, Walker N, MacMahon S, et al. Reduction of postoperative mortality and morbidity with epidural or spinal anaesthesia: results from overview of randomised trials. BMJ. 2000;321(7275):1493. https://doi.org/10.1136/bmj.321.7275.1493
- [17] Pöpping DM, Elia N, Tramer MR, et al. Protective effects of epidural analgesia on pulmonary complications after abdominal and thoracic surgery: a meta-analysis. Arch Surg Chic Ill 1960. 2008;143(10):990–909; discussion 1000. https://doi.org/10.1001/archsurg.143.10.990
- [18] Miller BL, Abel EJ, Richards KA, et al. Trends in epidural anesthesia use at the time of radical cystectomy and its association with perioperative and survival outcomes: a population-based analysis. Am J Clin Exp Urol. 2020;8(1):28–37.
- [19] Korgvee A, Junttila E, Kalliomaki M-L, et al. Ultrasound-guided quadratus lumborum block for postoperative analgesia: a systematic review and meta-analysis. Eur J Anaesthesiol. 2020;38(2):115–129. https://doi.org/10.1097/EJA.0000000000001368
- [20] Korgvee A, Veskimae E, Kalliomaki M-L, et al. Posterior quadratus lumborum block versus epidural analgesia for postoperative pain management after open radical cystectomy: a randomized clinical trial. Acta Anaesthesiol Scand. 2022;67(3):347–355. https://doi.org/10.1111/aas.14188
- [21] Moher D, Hopewell S, Altman DG, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. Int J Surg Lond Engl. 2012;10(1):28–55. https://doi.org/10.1016/j.ijsu.2011.10.001
- [22] Liedberg F, Hagberg O, Jerlström T, et al. Cystectomy for bladder cancer in Sweden – short-term outcomes after centralization. Scand J Urol. 2024;59:84–89. https://doi.org/10.2340/sju.v59.40120
- [23] Williams SB, Cumberbatch MGK, Daneshmand S, et al. Reporting radical cystectomy outcomes following implementation of enhanced recovery after surgery protocols: a systematic review and individual patient data meta-analysis. Eur Urol. 2020;78(5):719–730.
- [24] Rahman SN, Cao DJ, Winer AG, et al. Impact of neuraxial analgesia on outcomes following radical cystectomy: a systematic review. Urol Oncol Semin Orig Investig. 2021;39(2):100–108. https://doi.org/10.1016/j.urolonc.2020.10.073
- [25] Matulewicz RS, Patel M, Meeks JJ, et al. Transversus abdominis plane blockade as part of a multimodal postoperative analgesia plan in patients undergoing radical cystectomy. Bladder Cancer Amst Neth. 2018;4(2):161–167. https://doi.org/10.3233/BLC-170157
- [26] Burkhard JP, Jardot F, Wuethrich PY, et al. Opioid-free anesthesia for open radical cystectomy is feasible and accelerates return of bowel function: a matched cohort study. J Clin Med. 2023;12(11):3657. https://doi.org/10.3390/jcm12113657
- [27] Froehner M, Brausi MA, Studer UE, et al. Complications following radical cystectomy for bladder cancer in the elderly. Eur Urol. 2009;56(3):443–454. https://doi.org/10.1016/j.eururo.2009.05.008
- [28] Arslan-Carlon V, Tan KS, Donat SM, et al. Goal-directed versus standard fluid therapy to decrease ileus after open radical cystectomy. Anesthesiology. 2020;133(2):293–303. https://doi.org/10.1097/ALN.0000000000003367
- [29] Calvo-Vecino JM, Ripollés-Melchor J, De Lis SA, et al. Effect of goal-directed haemodynamic therapy on postoperative complications in low–moderate risk surgical patients: a multicentre randomised controlled trial (FEDORA trial). Br J Anaesth. 2018;120(4):734–744.
- [30] Wuethrich PY, Burkhard FC, Studer UE, et al. Restrictive deferred hydration combined with preemptive norepinephrine infusion during radical cystectomy reduces postoperative complications and hospitalization time. Anesthesiology. 2014;120(2):365–377. https://doi.org/10.1097/ALN.0b013e3182a44440