ORIGINAL RESEARCH ARTICLE
Use of Photodynamic diagnosis (PDD) at primary TURB: Potential influence on recurrence and progression rates in NMIBC: a registry-based study using a country cohort
Linea Blichert-Refsgaarda, Maria S. Lindgrena, Maria O. Sundelina, Charlotte Graugaard-Jensena, Mette Nørgaardb and Jørgen B. Jensena
aDepartment of Urology, Aarhus University Hospital, Aarhus N, Denmark; bDepartment of Clinical Epidemiology, Aarhus University Hospital, Aarhus N, Denmark
ABSTRACT
Objective: To investigate whether department-level use of photodynamic diagnosis (PDD) for primary transurethral bladder resections (TURBs) is associated with recurrence and progression rates in a non-selected, national cohort. Non-muscle invasive bladder cancer (NMIBC) has high global prevalence, and is characterized by high recurrence risk and risk of progression to muscle-invasive bladder cancer. Treatment effects and long-term outcomes rely on diagnostic accuracy, which may be enhanced using PDD for TURB. PDD-use in Denmark has varied between departments.
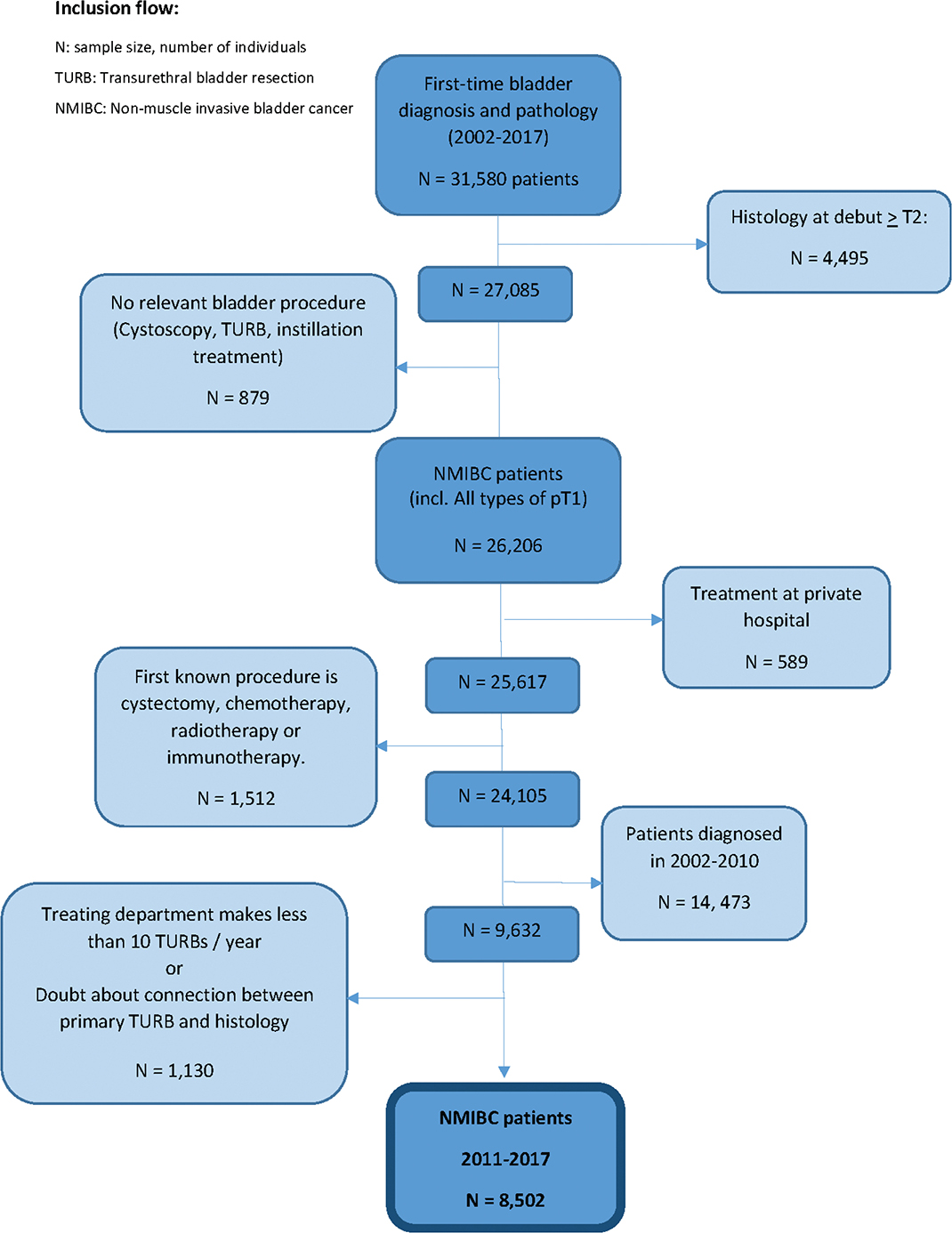
Material and Methods: We identified all Danish patients with primary NMIBC during 2011–2017 via the Danish National Patient Registry (DNPR) and divided them into four groups based on the treating department’s annual PDD use. We included 8,502 patients; 76% men, median age at diagnosis: 70 years (interquartile range [IQR]: 63, 77). Primary outcomes were recurrence- and progression risk differences (RDs) at 2 and 5 years depending on the PDD-exposure group. Results were additionally stratified by baseline pathological risk group.
Results: The PDD-use varied from <40% of primary TURBs in group 1 to >74% in group 4. Overall 2- and 5 years recurrence risks were 39.9% [95% CI: 38.8; 41.0] and 48.1% [95% CI: 46.9; 49.3], while risks of progression were 17.5% [95% CI: 16.7; 18.4] and 22.9% [95% CI: 21.9; 23.9]. PDD-exposure groups 2–4 had lower recurrence- and progression risks compared to group 1, most pronounced for high-risk NMIBC.
Conclusions: PDD-use in primary TURBs correlates with reduced 2- and 5 years recurrence- and progression risks in NMIBC. The PDD benefit was most noticeable in higher risk NMIBC. Photodynamic diagnosis, primary Trans Urethral Resection of the Bladder (TURB), progression risk, recurrence risk
KEYWORDS: Photodynamic diagnosis; primary Trans Urethral Resection of the Bladder (TURB); progression risk; recurrence risk
Citation: Scandinavian Journal of Urology 2025, VOL. 60, 115–123. https://doi.org/10.2340/sju.v60.43993.
Copyright: © 2025 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 31 March 2024; Accepted: 27 May 2025; Published: 24 June 2025
CONTACT: Linea Blichert-Refsgaard lineblic@rm.dk Department of Urology, Aarhus University Hospital, Palle Juul-Jensens Boulevard 35, 8200 Aarhus N, Denmark
Supplemental data for this article can be accessed online at https://doi.org/10.2340/sju.v60.43993
Competing interests and funding: This study was financially supported by Photocure ASA, Norway and Aarhus University.
The Danish Health Data Authority approved this study (reference ID: 137eb8eUTng14728865). The study is registered in the internal inventory of Region Midt (previously known as: Danish Data Protection Agency) (record number: 1-16-02-330-18).
Introduction
Annually, 2,000 new patients are diagnosed with bladder cancer (BC) in Denmark [1]. Approximately 75% of BC patients present with non-muscle invasive bladder cancer (NMIBC). Based on the high risk of recurrence up to 78% [2, 3], adjuvant intravesical instillation therapy with mitomycin C (MMC) or bacillus Calmette-Guerin vaccine (BCG) is recommended in guidelines [4–6].
Due to repeated transurethral resections of the bladder (TURBs), follow-up cystoscopies, and instillation therapy, NMIBC is one of the most costly cancers from diagnosis to death [7], and a disease with a potentially large influence on the patient’s quality of life.
Photodynamic diagnosis (PDD) is a well-established diagnostic enhancing tool. In several clinical studies, PDD provided a higher detection rate of carcinoma in situ (CIS) during TURB than conventional white light cystoscopy [8, 9]. Moreover, some randomized clinical trials have shown a reduced recurrence rate associated with the use of PDD [10–12] while another reported no recurrence-reducing effect of PDD [13].
We aimed to assess whether the 2- and 5-year recurrence- and progression risks of NMIBC, depended on the treating department’s level of PDD-use during primary TURBs through a nationwide, population-based study.
Materials and methods
Setting
The Danish population was approximately 5.7 million people in 2017 [14]. The public Danish Health Care system provides free medical services to all Danes. In Denmark, PDD was implemented in 2007. In the period 2011–2017, Denmark had 16 individual public urological departments. Because of centralization, this number decreased to 14 departments during this period. The Danish National Patient Registry (DNPR) was created in 1977 and is internationally considered one of the most comprehensive of its kind [15]. The validity of the coding in the DNPR is generally found to be high, which also applies to the codes related to NMIBC treatment [16, 17]. The DNPR is daily updated by the treating department and contains all information on TURBs, PDD-use, and treatment courses of adjuvant instillation therapy [18]. Both TURB, PDD usage, and instillation therapy have their own specific codes in the DNPR (Supplementary Table 1). Following a TURB, pathological diagnoses are registered in the National Pathology Registry using SNOMED codes that contain information on histological subtype, tumor stage, and tumor grade. Because of the unique Civil Personal Register (CPR) number assigned to all Danes, diagnoses, treatments, and pathological data can be linked on an individual level [19].
In Denmark the majority of patients are treated for NMIBC at public hospitals and the DNPR registration from private hospitals is known to be less complete [15].
Study population
Through the DNPR, we identified all Danish patients diagnosed with primary NMIBC from 2011 to 2017. Inclusion additionally required the following diagnoses registered in DNPR: BC, pathological diagnosis of neoplastic bladder lesions, and one of the following procedures as the first registered procedure: cystoscopy alone, cystoscopy with a biopsy, or TURB. The codebook shows all codes used in the sampling (Supplementary Table 1).
We excluded all patients with a cancer diagnosis other than bladder cancer, prostate cancer, and non-melanoma skin cancer at the time of diagnose. Furthermore, we excluded all patients treated at private hospitals because of the lower completeness of registration [15].
To avoid confounding by indication in direct PDD-use, we divided the urological departments into exposure groups depending on the annual percentage of total primary TURBs performed with PDD. We used the national quartiles of PDD-use at primary TURBs as cut-off points, leaving four exposure groups (PDD-exposure group 1–4). The patients were classified according to the exposure group of their treating department in the year of their primary TURB.
We included information on smoking related comorbidity in Table 1 as surrogate markers of significant smoking.
| Overall | Group 1 | Group 2 | Group 3 | Group 4 | |
| PDDusea | < 40% | 40–58% | 59–73% | ≥ 74% | |
| Number of departmentsb | 26 | 28 | 25 | 25 | |
| Individual patients | 8,502 | 1,410 | 2,570 | 1,779 | 2,743 |
| Median age (IQR) | 70 (63,77) | 70 (63,77) | 70 (63,76) | 71 (64,78) | 70 (63,77) |
| Sex | |||||
| Males | 6,466 (76%) | 1,075 (76%) | 1,954 (76%) | 1,343 (75%) | 2,094 (76%) |
| Females | 2,036 (24%) | 335 (24%) | 616 (24%) | 436 (25%) | 649 (24%) |
| PDD use (individuals) | 4,585 (54%) | 338 (24%) | 1,044 (41%) | 1,058 (59%) | 2,145 (78%) |
| SS MMC | 38 (0.4%) | 25 (1.8%) | 0 (0%) | 3 (0.2%) | 10 (0.4%) |
| Adjuvant MMC | 52 (0.6%) | 15 (1.1%) | 12 (0.5%) | 15 (0.8%) | 10 (0.4%) |
| Adjuvant BCG | 1,146 (13%) | 158 (11%) | 429 (17%) | 279 (16%) | 280 (10%) |
| Adjuvant treatment totalc | 1,184 (14%) | 169 (12%) | 436 (17%) | 291 (16%) | 288 (10%) |
| Cystectomy within 60 days | 270 (3.2%) | 83 (5.9%) | 112 (4.4%) | 41 (2.3%) | 34 (1.2%) |
| Radiotherapy within 60 days | 108 (1.3%) | 18 (1.3%) | 29 (1.1%) | 12 (0.7%) | 49 (1.8%) |
| Histologyd | |||||
| PUNLMP | 39 (0.5%) | 9 (0.6%) | 7 (0.3%) | 4 (0.2%) | 19 (0.7%) |
| pTa low grade | 3,738 (44%) | 605 (43%) | 1,089 (42%) | 747 (42%) | 1,297 (47%) |
| pTa undefined | 177 (2.1%) | 19 (1.3%) | 44 (1.7%) | 30 (1.7%) | 84 (3.1%) |
| pTa high grade | 1,566 (18%) | 229 (16%) | 468 (18%) | 335 (19%) | 534 (19%) |
| CIS | 553 (6.5%) | 71 (5.0%) | 163 (6.3%) | 109 (6.1%) | 210 (7.7%) |
| pT1a | 1,057 (12%) | 188 (13%) | 324 (13%) | 266 (15%) | 279 (10%) |
| pT1 undefined | 471 (5.5%) | 99 (7.0%) | 177 (6.9%) | 104 (5.8%) | 91 (3.3%) |
| pT1b | 715 (8.4%) | 150 (11%) | 246 (9.6%) | 163 (9.2%) | 156 (5.7%) |
| T undefinede | 186 (2.2%) | 40 (2.8%) | 52 (2.0%) | 21 (1.2%) | 73 (2.7%) |
| Total CIS detectionf | 902 (11%) | 118 (8.4%) | 287 (11%) | 194 (11%) | 303 (11%) |
| Smoking-related comorbidity | |||||
| COPD or Emphysema | 199 (2.3%) | 44 (3.1%) | 65 (2.5%) | 33 (1.9%) | 57 (2.1%) |
| AA | 46 (0.5%) | 9 (0.6%) | 21 (0.8%) | 6 (0.3%) | 10 (0.4%) |
| HDg | 138 (1.6%) | 36 (2.6%) | 47 (1.8%) | 31 (1.7%) | 24 (0.9%) |
| Period (time) | |||||
| 2011–2013 | 4,869 (57%) | 1,130 (80%) | 1,927 (75%) | 334 (19%) | 1,478 (54%) |
| 2014–2017 | 3,633 (43%) | 280 (20%) | 643 (25%) | 1,445 (81%) | 1,265 (46%) |
| IQR: interquartile range; SS: single shot; MMC: mitomycin C; BCG: Bacillus Calmette-Guérin; COPD: Chronic obstructive pulmonary disease; AA: Atherosclerosis and/or Aneurysm. aPercentage of primary transurethral bladder resections (TURBs) performed with PDD. bEvery department count for one every year – the department’s percentage PDD-use is calculated on an annual basis as the number of TURBs per year performed with PDD out of the total number of TURBs. cAdjuvant intravesical treatment with either MMC or BCG. dBaseline histology (primary TURB). pT1a: superficial subepithelial invasion, pT1b: deep subepithelial invasion. eT undefined: The majority of patients in the T_undefined-group had a pathological registration of ‘at least pT1’, which could represent a more invasive tumor stage than registered. fIncludes concomitant carcinoma in situ (CIS). gHeart Disease: Angina pectoris, unstable angina pectoris, AMI and chronic ischemic heart disease. |
|||||
Definitions
According to the Danish clinical guidelines, the first follow-up flexible cystoscopy is scheduled 4 months after the primary TURB [5].
A repeat TURB (reTURB) was defined as an additional pathological BC diagnosis registered in the National Pathology Registry within 60 days from the primary pathological NMIBC registration if no cystectomy code was registered in DNPR during this period. In the case of reTURB, the patient is classified according to the most advanced histological finding as the primary histology.
Recurrence was defined as registration of an additional pathological bladder cancer diagnosis in the National Pathology Registry at least 60 days after primary TURB.
As recommended by the International Bladder Cancer Group (IBCG) [20], the definition of progression in this study was defined as an increase in T stage from pTa or CIS to pT1, development of pT2 or greater or lymph node (N+) disease or distant metastasizes (M1), or an increase in grade from low grade to high grade including CIS. In addition, transition to more radical treatment (cystectomy, systemic chemotherapy, or radiation therapy) at least 60 days after primary TURB was also considered as progression in our study. Cystectomy, systemic chemotherapy, or radiation therapy provided within 60 days was considered as treatment of the primary diagnosis, and therefore not a progression.
Statistical analysis
We started follow-up at date of primary NMIBC diagnosis and calculated pseudo-observations for the cumulative incidence proportion under competing risk of death at 2 and 5 years. We used pseudo-observations in a generalized linear model resulting in estimates of risks and risk differences (RDs) using PDD exposure group as the explanatory variable. The outcomes were recurrence or progression within 2 and 5 years (risks and RDs), PDD exposure group 1 was the reference.
Aalen-Johansen curves were used to present the unadjusted estimates (cumulative incidents over time under the competing risk of death).
All estimates were presented with 95% confidence intervals. We adjusted the estimates for the calendar year of the primary TURB (2011–2013 or 2014–2017), baseline tumor pathological risk group (low/intermediate vs. high), and the use of adjuvant instillation therapy (yes or no).
In sub-analyses, we stratified the analyses by baseline pathological risk group; patients with pTa low grade (EORTC low- and intermediate risk) were included in the low-grade analysis, while patients with pTa high grade, CIS, and pT1 were included in the high-risk analysis.
We used STATA 17 in all data management, analyses, and graphics manufacturing.
Results
We identified 8,502 patients diagnosed with primary NMIBC in Denmark from 2011 to 2017; 76% men, with a median age at diagnosis of 70 years (interquartile range [IQR]: 63, 77) (Figure 1).
Using the national quartiles of the annual percentage PDD-use in primary TURBs in the distribution of departments into PDD-exposure groups resulted in four exposure groups (Table 1). Departments in group 1 used PDD in less than 40% of primary TURBs, departments in group 2 in 40–58%, departments in group 3 in 59–73%, and departments in group 4 in 74% or more.
The differences in patient volume in the Danish urological departments caused a slightly unequal individual patient distribution in the PDD-exposure groups (Table 1).
Figure 2 shows the Aalen-Johansen graphs of the overall, unadjusted recurrence and progression risks under the competing risk of death (2.1) and the cumulative incidences according to PDD exposure groups (2.2).
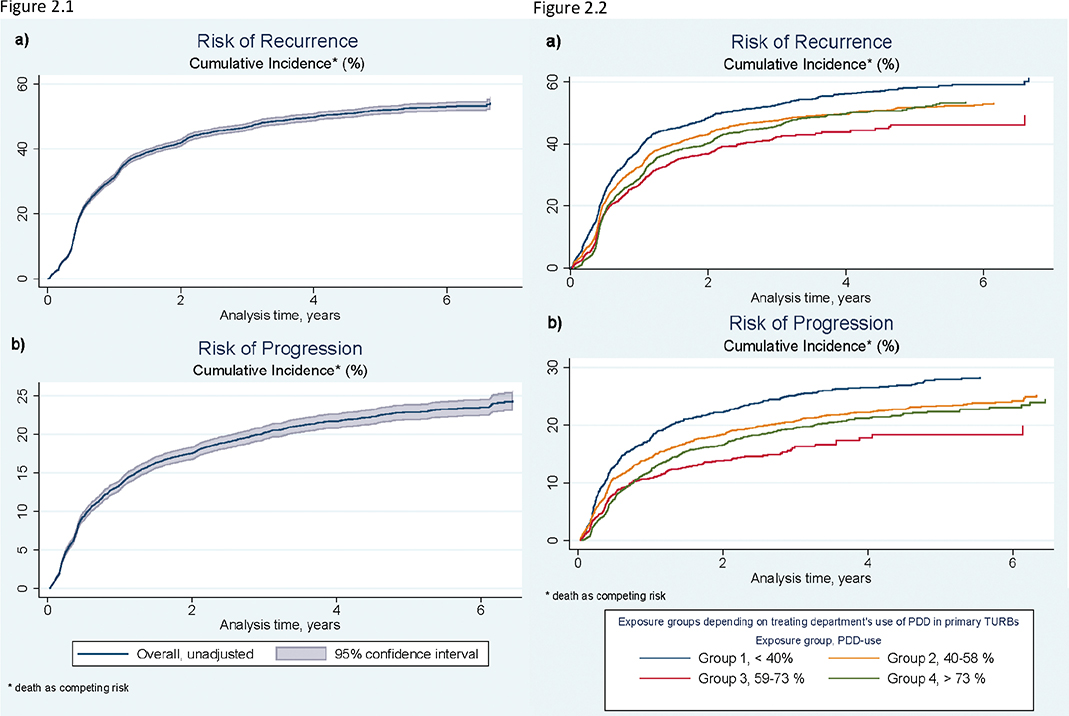
Figure 2. The risk of recurrence (a) and progression (b) of non-muscle invasive bladder cancer over time: The unadjusted overall risks (2.1) and risks depending on the treatment department’s use of Photo Dynamic diagnosis (PDD) in primary Trans Urethral Resections of the Bladder (TURBs) (2.2).
The overall risks of recurrence after 2 and 5 years were 39.9% [95% CI: 38.8; 41.0] and 48.1% [95% CI: 46.9; 49.3] (Table 2). The risk of recurrence was lower after both 2 and 5 years in PDD-exposure groups 2, 3, and 4 compared to group 1. PDD-use > 40%, low baseline pathological risk group, and the use of adjuvant instillation therapy all resulted in reduced 2-year recurrence risk (Table 2).
| Cumulative two- and five-year risks*: | ||||
| Recurrence risks | Progression risks | |||
| Unadjusted risks: | Two-year risk (%) [95% CI] | Five-year risk (%) [95% CI] | Two-year risk (%) [95% CI] | Five-year risk (%) [95% CI] |
| Overall | 39.9 [38.8; 41.0] | 48.1 [46.9; 49.3] | 17.5 [16.7; 18.4] | 22.9 [21.9; 23.9] |
| Adjusted risks: | Risk (%) (RD (%)) (RD) [95% CI] |
Risk (%) (RD (%)) (RD) [95% CI] |
Risk (%) (RD (%)) (RD) [95% CI] |
Risk (%) (RD (%)) (RD) [95% CI] |
| PDD exposure group**: | ||||
| 1 (< 40%) *** | 46.7 [43.8; 49.6] | 54.6 [51.2; 58.0] | 22.4 [20.0; 24.8] | 28.5 [25.5; 31.5] |
| 2 (40–58%) | (−5.5) ([−9.0; −1.9]) | (−6.5) ([−10.6; −2.3]) | (−4.0) ([−6.9; −1.2]) | (−5.2) ([−8.8; −1.6]) |
| 3 (59–73%) | (−11.4) ([−15.0; −7.7]) | (−10.9) ([−15.0; −6.8]) | (−8.3) ([−11.2; −5.5]) | (−9.5) ([−13.0; −6.0]) |
| 4 (≥ 74%) | (−8.4) ([−11.9; −4.9]) | (−7.0) ([−11.0; −3.0]) | (−5.9) ([−8.6; −3.1]) | (−6.2) ([−9.7; −2.7]) |
| Calendar year group: | ||||
| Group 1: 2011–2013*** | 40.8 [39.2; 42.3] | 48.5 [46.6; 50.4] | 17.7 [16.5; 18.9] | 23.2 [21.6; 24.8] |
| Group 2: 2014–2017 | (−2.0) ([−4.2; 0.2]) | (−1.0) ([−3.3; 1.4]) | (−0.3) ([−2.0; 1.4]) | (−0.7) ([−2.7; 1.3]) |
| Pathological risk group: | ||||
| Low/intermediate risk*** | 35.3 [33.7; 37.0] | 46.0 [44.0; 47.9] | 11.0 [9.9; 12.0] | 17.1 [15.6; 18.5] |
| High risk | (9.1) ([6.9; 11.4]) | (4.4) ([1.8; 6.9]) | (12.0) ([10.5; 13.8]) | (10.6) ([8.5; 12.7]) |
| Total adjuvant instillation treatment****: | ||||
| No*** | 40.7 [39.5; 41.9] | 49.0 [47.7; 50.4] | 18.1 [17.1; 19.0] | 23.4 [22.3; 24.6] |
| Yes | (−5.8) ([−8.9; −2.6]) | (−6.8) ([−10.3; −3.2]) | (−3.8) ([−6.1; −1.5]) | (−3.9) ([−6.8; −1.0]) |
| Multivariate, adjusted risks: | ||||
| PDD exposure group 1, low/intermediate, and no adjuvant instillation treatment*** | 42.0 [38.8; 45.1] | 52.2 [48.4; 55.9] | 15.5 [13.1; 18.0] | 21.9 [18.7; 25.0] |
| PDD exposure group: • 2 • 3 • 4 |
(−5.2) ([−8.8;−1.6]) (−11.2) ([−14.9; −7.5]) (−7.9) ([−11.4; −4.4]) |
(−5.7) ([−9.9;−1.5]) (−10.6) ([−14.7; −6.4]) (−6.5) ([−10.5; −2.5]) |
(−3.6) ([−6.4;−0.7]) (−8.0) ([−10.8; −5.1]) (−5.2) ([−8.0; −2.5]) |
(−4.1) ([−7.7; −0.5]) (−8.7) ([−12.1; −5.2]) (−5.1) ([−8.6; −1.6]) |
| High grade/high risk: | (12.0) ([9.6; 14.3]) | (6.8) ([4.2; 9.5]) | (14.7) ([12.9; 16.6]) | (13.0) ([10.7; 15.3]) |
| Adjuvant instillation: | (−12.0) ([−15.3; −8.6]) | (−10.2) ([−14.0; −6.2]) | (−11.0) ([−13.6; −8.4]) | (−10.0) ([−13.2; −6.8]) |
| RD: Risk difference; PDD: Photodynamic diagnosis. * Death as competing risk. ** Percentage of primary TURBs performed with PDD at department-level. *** Reference group. **** Adjuvant instillation with MMC or BCG after primary TURB (re-TURB). |
||||
The overall 2 and 5-year progression risks was 17.5% [95% CI: 16.7; 18.4] and 22.9% [95% CI: 21.9; 23.9], respectively (Table 2). The progression risk was lower in PDD-exposure groups 2, 3, and 4 compared to group 1. The most influential factor to the progression risk was the baseline pathological risk group. Use of adjuvant instillation therapy also reduced the 2- and 5 year progression risks.
Table 3 shows estimates of the 2- and 5-year cumulative recurrence and progression risks stratified by baseline pathological risk group: low-grade pTa (low- and intermediate risk) versus high-risk NMIBC. In the low-grade analysis, only PDD-exposure group 3 had a lower risk of recurrence and progression as compared to the reference. In the high-risk analysis, PDD-exposure groups 2, 3, and 4 were associated with a reduced risk of recurrence and progression compared to PDD-exposure group 1.
| Cumulative two- and five-year recurrence- and progression risks*: | ||||
| Low/intermediate risk (pTa low grade): N = 3,738 | High risk (pTa high grade, CIS and pT1): N = 4,518 | |||
| Risk of recurrence: | ||||
| Unadjusted risks: | Two-year risk (%) [95% conf. interval] | Five-year risk (%) [95% conf. interval] | Two-year risk (%) [95% conf. interval] | Five-year risk (%) [95% conf. interval] |
| Overall | 35.3 [33.7; 37.0] | 46.0 [44.1; 47.9] | 44.5 [42.9; 46.0] | 50.4 [48.7; 52.0] |
| Adjusted risks: | Risk (%) (RD (%)) (RD) [95% conf. interval] |
Risk (%) (RD (%)) (RD) [95% conf. interval] |
Risk (%) (RD (%)) (RD) [95% conf. interval] |
Risk (%) (RD (%)) (RD) [95% conf. interval] |
| PDD exposure group**: | ||||
| 1 (< 40%) *** | 37.7 [33.3; 42.1] | 49.4 [44.0; 54.8] | 54.6 [50.8; 58.5] | 58.9 [54.6; 63.2] |
| 2 (40–58%) | (−1.6) ([−7.0; 3.8]) | (−3.5) ([−10.1; 3.2]) | (−9.1) ([−13.9; −4.3]) | (−8.4) ([−13.7; −3.0]) |
| 3 (59–73%) | (−7.6) ([−13.1; −2.1]) | (−10.0) ([−16.4; −3.5]) | (−14.9) ([−20.0; −10.0]) | (−11.9) ([−17.2; −6.6]) |
| 4 (≥ 74%) | (−1.1) ([−6.3; 4.1]) | (−1.2) ([−7.5; 5.1]) | (−13.6) ([−18.4; −8.9]) | (−11.1) ([−16.4; −5.9]) |
| Risk of progression: | ||||
| Unadjusted risks: | Two-year risk (%) [95% conf. interval] | Five-year risk (%) [95% conf. interval] | Two-year risk (%) [95% conf. interval] | Five-year risk (%) [95% conf. interval] |
| Overall | 11.0 [9.9; 12.0] | 17.1 [15.6; 18.5] | 23.1 [21.8; 24.4] | 27.7 [26.2; 26.1] |
| Adjusted risks: | Risk (%) (RD (%)) (RD) [95% conf. interval] |
Risk (%) (RD (%)) (RD) [95% conf. interval] |
Risk (%) (RD (%)) (RD) [95% conf. interval] |
Risk (%) (RD (%)) (RD) [95% conf. interval] |
| PDD exposure group**: | ||||
| 1 (< 40%) *** | 13.4 [10.3; 16.4] | 20.4 [16.1; 28.6] | 29.6 [26.1; 33.1] | 33.9 [29.8; 38.0] |
| 2 (40–58%) | (−1.2) ([−4.9; 2.5]) | (−2.4) ([−7.6; 2.9]) | (−6.3) ([−10.5; −2.2]) | (−6.3) ([−11.3; −1.4]) |
| 3 (59–73%) | (−5.4) ([−9.1; −1.8]) | (−7.4) ([−12.3; −2.6]) | (−10.8) ([−15.0; −6.5]) | (−10.4) ([−15.2; −5.6]) |
| 4 (≥ 74%) | (−2.8) ([−6.3; 0.7]) | (−3.3) ([−8.3; 1.7]) | (−7.1) ([−11.3; −3.0]) | (−6.5) ([−11.4; −1.7]) |
| RD: Risk difference; N: number of individuals; CIS: Carcinoma in situ; PDD: Photodynamic diagnosis. * Death as competing risk. ** Percentage of primary TURBs performed with PDD at department-level. *** Reference group. |
||||
Discussion
In this nationwide cohort study, we found a lowered risk of recurrence and progression of NMIBC among patients treated in departments with a percentage PDD-use at the primary TURBs of more than 40%. We did not find the risk reduction to be directly correlated to increasing use of PDD; patients in PDD-exposure group 3 (department PDD-use: 59–73%) had a lower risk of both recurrence and progression than patients in PDD-exposure group 4 (department PDD-use: ≥74%). Theoretically, this non-direct correlation, and the fact that PDD used at primary TURB, seemed to have a long-term (5 years) positive impact on recurrence and progression, may indicate that departments in PDD-exposure group 3 differ in ways not apparent in this study. This could be, for example, a generally larger use of instillation therapy outside of primary treatment, which would not be covered by this study. However, a newer systematic review and meta-analysis indicates that a recurrence-reducing effect of PDD persists for at least 2 years and appears to continue after 5 years [21].
A randomized trial conducted on 426 patients in 22 U.K. hospitals reports no recurrence-reducing effect of PDD after 3 years when compared to white light [13]. However, it is well known that patients enrolled in clinical trials obtain better outcomes than non-trial patients simply because recruitment into trials is a driver for quality improvement [22]. In the case of NMIBC, enrolment into an RCT could result in higher quality white light TURB and thereby lowering the effect of a visual diagnostic enhancing toll as PDD. This may not reflect real-life clinical settings, where procedures are often performed by less experienced surgeons. Gallagher and colleagues attempted ‘real-life experience’ in a prospective cohort study published in 2017 comparing recurrence rates (PDD vs. white light) at 3 years; they reported a significantly reduced 3-year recurrence rate associated with PDD [23]. Thus, we do find our results based on large-scale non-selected national data conducted prospectively in an everyday setting relevant in accomplishing NMIBC research.
The distribution of patients into PDD exposure groups in our study is different from most other studies where exposure is categorized as the direct, individual PDD use per patient (yes or no). Looking at the direct use will increase confounding by indication bias, for example, in patients with very large tumors: They will not receive PDD in an everyday setting since it is simply not necessary to enhance the visualization of the tumor. This will however, potentially place a larger proportion of patients with high risk tumors in the ‘no PDD-use’- group and thereby increase the estimated risk-reducing effect of PDD. The Danish urological departments have a varying use of PDD. This fact together with the large size of the Danish registries, and thereby the large study cohort, provided the opportunity to assess the influence of PDD outside a clinical study setting without the risk of confounding by indication. However, looking at PDD-use at department level might slightly underestimate the risk-reducing effect of PDD in the patients who are candidates for PDD, because non-candidates are included in all PDD exposure-groups and thereby dilutes the risk-reducing effect. Nevertheless, we do believe this underestimation to be smaller than the risk of overestimating the risk-reducing effect associated with the direct PDD-use.
Our 2- and 5-year recurrence- and progression risks were comparable with the estimates found by both the Spanish Club Urológico Español de Tratamiento Oncológico (CUETO) group and the European Organisation for Research and Treatment of Cancer (EORTC) group [2, 24].
The use of adjuvant installation therapy appears extremely low when comparing guidelines and the registered primary histology. At least patients with primary histology of pTa high-grade, CIS, or pT1 should receive BCG according to EAU guidelines [4, 6]. The adherence to guidelines with regard to BCG therapy in high-risk NMIBC has previously been assessed and found to be relatively low worldwide, in Europe/Australia the adherence rate is estimated to be 65%, no Danish studies were included in the analyses [25]. The reported BCG-use in this study seems reliable regarding treatment after primary TURBs in Denmark. Data on adjuvant instillation therapy after recurrent NMIBC were not included in this study.
Compared to the EAU guidelines, the Danish guidelines have lower strength of recommendation on perioperative single shot (SS) MMC use [4–6, 26]. Use of perioperative SS MMC is not included in the analysis of this study. We found an extremely sparse recording of this code in the primary TURB registration in all PDD-exposure groups. We do not deem this exclusion likely to significantly affect the outcome, especially not the results of the high-risk NMIBC [27].
Entry into the register (2011–2013 or 2014–2017) is unequally distributed between the PDD exposure groups; one could argue that newer cystoscopies etc. would provide a reduced risk due to entering time alone, but the adjusted analyses did not confirm this hypothesis. The Aalen-Johansen curves of the unadjusted, estimated cumulative risks showed a difference already after 2 years. Therefore, the shorter registered follow-up in PDD-exposure group 3 did likely not influence the results of the recurrence and progression risks.
When stratifying on baseline pathological risk group, PDD appeared to have the largest risk reducing effect in high-risk NMIBC, with regard to both recurrence and progression. Unfortunately, we lacked information on tumor size and numbers and therefore, the baseline pathological risk groups included all pTa high grade in the high-risk group. The single pTa high grade tumors smaller than three centimeters is included in the EORTC intermediate risk group and are therefore misclassified in our analyses. Although this introduced a misclassification bias in the sub-analyses, it would most likely bias our results toward no difference, and we would therefore underestimate the difference in PDD’s risk reducing effect depending on pathological risk group. Burger and colleagues published a meta-analysis in 2013 reviewing raw data from prospective studies assessing the 1-year recurrence rates in normal white light TURB versus blue light TURB, and found the beneficial effect of PDD to be independent of risk-group [28]. Gallagher et al. have also assessed the association between PDD-use and a lower 1-year recurrence rate in all risk groups compared to white light TURBs, but the significant difference was only maintained until 3 years in the high-risk group in the all patients analyses [23]. A Cochrane systematic review from 2021 including 16 randomized controlled trails, 4325 patients, assessing the effect of PDD-enhanced TURB compared to white light-based TURB on recurrence and progression of NMIBC also found that the risk reducing effect of PDD depended on the pathological baseline risk-group. Similar to our findings, they concluded that low-risk patients may have little or no risk-reducing effect of PDD with regard to either recurrence or progression, PDD may reduce the risk of recurrence in intermediate- and high-risk patients, and the risk of progression with regard to high-risk patients (low-certainty evidence) [29]. It has been estimated that the majority of recurrences in intermediate- and high risk T1 is due to overlooked and/or residual tumors [30]. This could be a part of the explanation to why the diagnostic enhancing tool of PDD shows the greatest effect in the high-risk analyses. Since the histology is unknown before primary TURB, another strategy could be to focus PDD-use at high-risk recurrence. However, in this study we focused on the primary TURB since this cohort would be homogenous regarding previous TURBs and instillation therapies. Future studies should assess the effect of PDD on recurrent NMIBC.
Additional limitations of our study are mainly due to design. It was not possible to extract information on tumor size and the amount of tumors from the registry; these factors are included in the EORTC and the CUETO (only number of tumors) NMIBC risk scoring systems [2, 24]. The education level and skills of the surgeon, who performed the TURB, are not available either and it is reasonable to assume this has an impact on the risk of recurrence and progression of NMIBC as well. If one or more of these factors systematically differed between the groups, it could potentially influence the result. However, we do not have any reason to believe this to be the case. The work-up of hematuria and primary diagnosis of NMIBC are performed at all Danish urological departments without any patient-selection, and the education of Danish urologists are standardized at a national level.
In conclusion, high use of PDD in primary TURBs appears to be associated with lower risk of recurrence and progression of NMIBC after both 2 and 5 years. Stratified on primary pathological NMIBC risk-group, the risk reducing effect of PDD-use appears most pronounced for high-risk tumors.
Acknowledgments
The authors would like to thank Vibeke Juul Morrison for her help in language editing.
References
- [1] DaBlaCa-data. Annual Report 2020, Bladder Cancer, Denmark. DaBlaCa-data; [updated 26-2-2021]. Available from: https://www.sundhed.dk/content/cms/86/15686_dablaca_aarsrapport_2020_offentlig_260221.pdf [cited july 31. 2022]
- [2] Sylvester RJ, van der Meijden AP, Oosterlinck W, et al. Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: a combined analysis of 2596 patients from seven EORTC trials. Eur Urol. 2006;49(3):466–465; discussion 75–77. https://doi.org/10.1016/j.eururo.2005.12.031
- [3] Ray ER, O’Brien TS. Should urologists be spending more time on the golf course? BJU Int. 2007;100(4):728–729. https://doi.org/10.1111/j.1464-410X.2007.06876.x
- [4] Babjuk M, Burger M, Compérat EM, et al. European Association of Urology Guidelines on non-muscle-invasive bladder cancer (TaT1 and carcinoma in situ) – 2019 Update. Eur Urol. 2019;76(5):639–657. https://doi.org/10.1016/j.eururo.2019.08.016
- [5] DaBlaCa. National guidelines, bladder cancer. DaBlaCa; 2024. Available from: https://www.dmcg.dk/kliniske-retningslinjer/kliniske-retningslinjer-opdelt-paa-dmcg/cancer-i-urinvejene/blaerekraeft/ [cited may 19. 2025]
- [6] EAU. EAU guidelines on non-muscle invasive bladder cancer. 2025. Available from: https://d56bochluxqnz.cloudfront.net/documents/full-guideline/EAU-Guidelines-on-Non-muscle-invasive-Bladder-Cancer-2025.pdf [cited may 21. 2025]
- [7] Svatek RS, Hollenbeck BK, Holmäng S, et al. The economics of bladder cancer: costs and considerations of caring for this disease. Eur Urol. 2014;66(2):253–262. https://doi.org/10.1016/j.eururo.2014.01.006
- [8] Fradet Y, Grossman HB, Gomella L, et al. A comparison of hexaminolevulinate fluorescence cystoscopy and white light cystoscopy for the detection of carcinoma in situ in patients with bladder cancer: a phase III, multicenter study. J Urol. 2007;178(1):68–73. https://doi.org/10.1016/j.juro.2007.03.028
- [9] Schmidbauer JA, Witjes F, Schmeller N, et al. Improved detection of urothelial carcinoma in situ with hexaminolevulinate fluorescence cystoscopy. J Urol. 2004;171(1):135–138. https://doi.org/10.1097/01.ju.0000100480.70769.0e
- [10] Geavlete B, Multescu R, Georgescu D, et al. Treatment changes and long-term recurrence rates after hexaminolevulinate (HAL) fluorescence cystoscopy: does it really make a difference in patients with non-muscle-invasive bladder cancer (NMIBC)? BJU Int. 2012;109(4):549–556. https://doi.org/10.1111/j.1464-410X.2011.10374.x
- [11] Grossman HB, Gomella L, Fradet Y, et al. A phase III, multicenter comparison of hexaminolevulinate fluorescence cystoscopy and white light cystoscopy for the detection of superficial papillary lesions in patients with bladder cancer. J Urol. 2007;178(1):62–67. https://doi.org/10.1016/j.juro.2007.03.034
- [12] Hermann GG, Mogensen K, Carlsson S, et al. Fluorescence-guided transurethral resection of bladder tumours reduces bladder tumour recurrence due to less residual tumour tissue in Ta/T1 patients: a randomized two-centre study. BJUInt. 2011;108(8 Pt 2):E297–E303. https://doi.org/10.1111/j.1464-410X.2011.10090.x
- [13] Heer R, Lewis R, Vadiveloo T, et al. A randomized trial of PHOTOdynamic surgery in non-muscle-invasive bladder cancer. NEJM Evid. 2022;1(10):EVIDoa2200092. https://doi.org/10.1056/EVIDoa2200092
- [14] statestik D. Available from: https://www.dst.dk/da/Statistik/nyheder-analyser-publ/Publikationer/VisPub?cid=214992017 [ cited july 28. 2022]
- [15] Lynge E, Sandegaard JL, Rebolj M. The Danish National Patient Register. Scand J Public Health. 2011;39(7 Suppl):30–33. https://doi.org/10.1177/1403494811401482
- [16] Schmidt M, Schmidt SA, Sandegaard JL, et al. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. https://doi.org/10.2147/CLEP.S91125
- [17] Blichert-Refsgaard L, Nørgaard M, Bengtsen MB, et al. Positive predictive values of procedure codes on the treatment of non-muscle invasive bladder cancer in the Danish National Patient Registry. Clin Epidemiol. 2022;14:1317–1325. https://doi.org/10.2147/CLEP.S376566
- [18] eSundhed. Documentation of the Danish National Patient Registry. [cited 18-11-2016]. Available from: https://www.esundhed.dk/Dokumentation/DocumentationExtended?id=52016
- [19] Frank L. Epidemiology. When an entire country is a cohort. Science. 2000;287(5462):2398–2399. https://doi.org/10.1126/science.287.5462.2398
- [20] Lamm D, Persad R, Brausi M, et al. Defining progression in nonmuscle invasive bladder cancer: it is time for a new, standard definition. J Urol. 2014;191(1):20–27. https://doi.org/10.1016/j.juro.2013.07.102
- [21] Veeratterapillay R, Gravestock P, Nambiar A, et al. Time to turn on the blue lights: a systematic review and meta-analysis of photodynamic diagnosis for bladder cancer. Eur Urol Open Sci. 2021;31:17–27. https://doi.org/10.1016/j.euros.2021.06.011
- [22] Ray ER, Coker B, Chatterton K, et al. Improving bladder cancer outcomes: the impact of initiating a phase IV randomised controlled clinical trial. Br J Med Surg Urol. 2009;2(2):67–72. https://doi.org/10.1016/j.bjmsu.2008.11.006
- [23] Gallagher KM, Gray K, Anderson CH, et al. ‘Real-life experience’: recurrence rate at 3 years with Hexvix(®) photodynamic diagnosis-assisted TURBT compared with good quality white light TURBT in new NMIBC – a prospective controlled study. World J Urol. 2017;35(12):1871–1877. https://doi.org/10.1007/s00345-017-2077-6
- [24] Fernandez-Gomez J, Madero R, Solsona E, et al. Predicting nonmuscle invasive bladder cancer recurrence and progression in patients treated with bacillus Calmette-GuerIn: the CUETO scoring model. J Urol. 2009;182(5):2195–2203. https://doi.org/10.1016/j.juro.2009.07.016
- [25] Van Rhijn BWG, Burger M. Low adherence to guidelines in non-muscle-invasive disease. Nat Rev Urol. 2016;13(10):570–571. https://doi.org/10.1038/nrurol.2016.165
- [26] DaBlaCa. National guidelines, bladder cancer. DaBlaCa; 2020. Available from: http://www.skejby.net/DaBlaCa-web/DaBlaCaWEB.htm [cited july 31. 2022]
- [27] Sylvester RJ, Oosterlinck W, Holmang S, et al. Systematic review and individual patient data meta-analysis of randomized trials comparing a single immediate instillation of chemotherapy after transurethral resection with transurethral resection alone in patients with stage pTa-pT1 urothelial carcinoma of the bladder: which patients benefit from the instillation? EurUrol. 2016;69(2):231–244. https://doi.org/10.1016/j.eururo.2015.05.050
- [28] Burger M, Grossman HB, Droller M, et al. Photodynamic diagnosis of non-muscle-invasive bladder cancer with hexaminolevulinate cystoscopy: a meta-analysis of detection and recurrence based on raw data. EurUrol. 2013;64(5):846–854. https://doi.org/10.1016/j.eururo.2013.03.059
- [29] Maisch P, Koziarz A, Vajgrt J, et al. Blue versus white light for transurethral resection of non-muscle invasive bladder cancer. Cochrane Database Syst Rev. 2021;12(12):Cd013776. https://doi.org/10.1002/14651858.CD013776.pub2
- [30] Herr HW. The value of a second transurethral resection in evaluating patients with bladder tumors. J Urol. 1999;162(1):74–76. https://doi.org/10.1097/00005392-199907000-00018