ORIGINAL RESEARCH ARTICLE
Prostate artery embolization for benign prostatic hyperplasia: a retrospective single-center study of clinical outcome
Jon Bjarnasona,b , Johann Pall Ingimarssonc, Hjalti Thorissonb, Kristbjorn Reynissonb, Jon Orn Fridrikssonc, Baldvin Thorkell Kristjanssonc, and Fernando Bazanb
, Johann Pall Ingimarssonc, Hjalti Thorissonb, Kristbjorn Reynissonb, Jon Orn Fridrikssonc, Baldvin Thorkell Kristjanssonc, and Fernando Bazanb
aDepartment of Radiology, Landspitali University Hospital, Reykjavik, Iceland; bDepartment of Interventional Radiology, Landspitali University Hospital, Reykjavik, Iceland; cDepartment of Urology, Landspitali University Hospital, Reykjavik, Iceland
ABSTRACT
Objective: To evaluate clinical outcome and complications of prostate artery embolization (PAE) in Iceland, using the International Prostate Symptom Score (IPSS), quality of life (QoL) and catheter freedom to measure clinical success.
Materials and methods: Retrospective single-center study, including patients who underwent PAE from August 2019 to February 2024 due to benign prostatic hyperplasia (BPH). Patients completed a questionnaire on lower urinary tract symptoms (LUTS), QoL, catheter status and use of medication. All additional data were retrieved from the medical records.
Results: A total of 34 patients were included, with a mean age of 75 during PAE and a technical success rate of 91%. Patients had significant clinical improvement, with a mean reduction in IPSS score from 20.0 to 9.0 (p < 0.001) and QoL score from 5.5 to 1.8 (p < 0.001). PAE also resulted in a 69% reduction (p < 0.001) in urinary catheter dependency. Post-PAE complications were uncommon (3/34) and all resolved without long-term effects.
Conclusion: PAE is an effective and safe treatment option for LUTS and/or urinary retention in men with BPH, offering catheter freedom and significant improvement in urological symptoms and quality of life.
KEYWORDS: Prostate artery embolization; PAE; benign prostatic hyperplasia; BPH; IPSS; QoL; LUTS
Citation: Scandinavian Journal of Urology 2025, VOL. 60, 130–134. https://doi.org/10.2340/sju.v60.44137.
Copyright: © 2025 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 5 March 2025; Accepted: 12 June 2025; Published: 10 July 2025
CONTACT: Jon Bjarnason jonbjarnason92@gmail.com Department of Radiology, Akademiska Sjukhuset, Uppsala, Sweden, Sjukhusvägen, 75185 Uppsala, Sweden
Competing interests and funding: The authors report no conflicts of interest.
This study has received no funding as of now.
Introduction
Benign prostatic hyperplasia (BPH) is a common cause of lower urinary tract symptoms (LUTS) in men. It results from hyperproliferation of the prostatic transitional zone. The exact etiology is considered multifactorial, with age being a major risk factor. Prevalence increases markedly with age, with the majority of men being symptomatic by the age of 70 [1, 2].
LUTS is often assessed with the International Prostate Symptom Score (IPSS), and the presence of these symptoms is often associated with reduced quality of life (QoL) [3, 4].
Multiple treatment options are available, from lifestyle modifications to surgical interventions. Among surgical interventions, the transurethral resection of the prostate (TURP) remains the gold standard for prostate volumes < 80 ml. However, other alternatives, such as holmium laser enucleation (HoLEP), transurethral microwave thermotherapy (TUMT), thermo-expandable intraprostatic stents and prostate artery embolization (PAE), have emerged as minimally invasive options for selected patients in an attempt to reduce complication risk [2, 5–8]. A recent Finnish nationwide study demonstrated a trend towards increasing use of minimally invasive surgical techniques, although TURP volumes remained stable [9]. In line with these efforts, technical modifications such as intraprostatic injections of mepivacaine-adrenaline prior to TURP have also been explored [10].
PAE is an evolving treatment modality, first performed successfully in 2010 [11]. PAE has demonstrated efficacy in both medium- and large-sized prostates and is considered an alternative to TURP and HoLEP, offering shorter recovery times and lower complication rates [6, 12–14]. In addition, the therapeutic potential of embolization techniques has been successfully applied in other urological areas, such as selective arterial embolization of renal angiomyolipomas [15].
Although evidence remains limited regarding optimal patient selection, PAE is generally recommended in moderate to severe LUTS, large prostates (> 80 ml), non-surgical candidates or patients who opt for less invasive treatment [2, 16].
PAE has also proven effective for successful urinary catheter removal, with the majority of patients achieving catheter freedom, which is especially beneficial as patients with chronic catheters are often unsuitable for surgery [2, 5, 17].
Pre-procedural cross-sectional imaging is generally recommended with either CT or MRI to determine if patients are suitable candidates for PAE, as vessel tortuosity, atherosclerosis and anatomic variants may render PAE challenging or even impossible [2, 12].
Systematic reviews of PAE have demonstrated significant improvements in IPSS and QoL at 12 months, with a mean IPSS score improvement of 9.31 from a baseline of 23.75 and a mean QoL of 2.11 from a mean baseline of 4.63 [18].
Significant clinical improvement is typically seen 1 month after PAE and is often sustained over a significant time. However, re-intervention rates tend to increase due to symptomatic recurrence, with roughly 20% of patients requiring re-intervention within the first 5 years [19–21].
PAE was recently introduced as an alternative treatment option for BPH in Iceland. The aim of this study is to evaluate the effectiveness and safety profile of PAE at our institution.
Materials and methods
This retrospective single-center study included patients with BPH and a prostate volume > 40 ml who underwent PAE at our institution between August 2019 and February 2024 due to LUTS and/or urinary retention. All patients were referred by a urologist. Patients with a primary indication of acute hematuria and/or bilateral internal iliac artery occlusion on preoperative multiplanar reformation (MPR) computed tomography (CT) angiography were excluded.
A Foley catheter was placed in all patients 1 day prior to the procedure. The balloon was filled with 30% contrast mixture to aid urinary bladder visualization during the procedure. Vascular access was with a 5-Fr sheath under ultrasound guidance, either via the left radial (85%) or the common femoral artery (15%). Hemostasis was achieved with a TR-band® for radial access and a vascular closure device (Starclose® or Angioseal®) for femoral access. For all patients, Embospheres® (300–500 μm; Merit Medical) were used as embolization, which was delivered through a 2-Fr angled Pursuit Merit™ microcatheter (Merit Medical). Postoperatively, all patients were monitored for at least 4 h in a day-care ward. Patients were discharged with an indwelling Foley catheter, which was subsequently removed after 1 week if possible.
The data collection was conducted between May 2024 and August 2024, in which patients were contacted and asked to complete a questionnaire assessing LUTS, QoL, use of medication, and urinary catheter status. Each patient reported these parameters retrospectively 1 month prior to the PAE and at the current date of the questionnaire. Follow-up was based on the time from the procedure and the date of questionnaire.
Technical success was defined as successful bilateral PAE. Clinical success was defined at follow-up as an improvement of IPSS by ≥ 3 points, QoL by > 2 points or successful catheter removal, similar to previous studies [5, 17]. Post-embolization syndrome (PES) was considered an expected postprocedural event rather than a procedural complication.
The IPSS and QoL scales were used to assess symptom severity when applicable. The IPSS score ranges from 0 to 35, with higher scores indicating more severe symptoms, while QoL ranges from 0 (delighted) to 6 (terrible). All additional relevant data were retrospectively obtained from the medical records. For data analysis, we utilized Microsoft Excel and the statistical software R.
This study was conducted in accordance with ethical standards and approved by the Bioethics Committee of Iceland (license number VSN-24-027). All participants provided informed patient consent.
Results
A total of 34 patients agreed to participate in this study, with a mean age of 75 at the time of embolization and a mean prostate volume of 155 ml (49 – 290). The mean procedure time was 93 min (40 – 167) and technical success rate was 91%, while unilateral PAE was achieved in the remaining cases. Among patients who underwent unilateral embolization, one had subsequent successful contralateral embolization 35 months from the previous procedure with a different arterial approach. In the other two cases, only a unilateral embolization was performed due to difficult tortuous vessel anatomy and/or deemed unsafe for embolization due to risk of non-target embolization.
Baseline parameters of patients prior to embolization are presented in Table 1. The mean follow-up was 28.2 months, ranging from 4.2 to 54.1 months.
Prior to PAE, 47% of patients experienced urinary retention requiring either intermittent or indwelling catheterization. At the time of follow-up, 69% of these patients had achieved complete catheter freedom (p = 0.004), with a mean follow-up of 28.8 months.
The majority of patients (79%) were on pharmacological treatment prior to embolization, either 5α-reductase inhibitors and/or α-blockers. Significant reduction in medication use was observed after PAE, with 59% of them requiring continued, unchanged pharmacological management (p < 0.001).
Non-catheterized patients (n = 18) showed a significant improvement in IPSS score after embolization, with a mean improvement of 11 points (p < 0.001) and a mean follow-up of 27.6 months (Figure 1). Patients who achieved complete catheter freedom (n = 11) had a mean IPSS score of 6 after PAE, with a mean follow-up of 31.4 months.
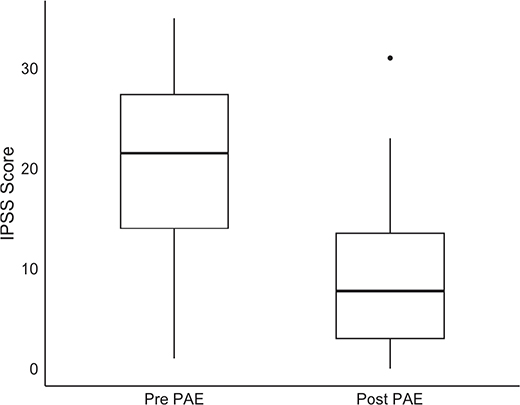
Figure 1. International Prostate Symptom Score (IPSS) score before and after prostate artery embolization (n = 18). Box = 25th and 75th percentiles; lines show minimum and maximum values (1.5 * IQR); bold line = median. Outliers are presented as black circles. Abbreviations: IPSS: International Prostate Symptom Score; PAE: prostatic artery embolization; IQR: interquartile range.
When divided into two follow-up periods prior to and after 24 months, the mean improvement in IPSS score was 10.1 in patients prior to 24 months and 12.6 for patients with follow-up beyond 24 months. This difference was not significant (p = 0.617).
Table 2 shows the mean improvements in IPSS and QoL scores following PAE, stratified by follow-up periods. While QoL improvement was statistically significant across most follow-up periods, IPSS improvement did not reach statistical significance during the same intervals. Furthermore, there was no significant difference in IPSS and QoL improvements when compared between the follow-up periods (p = 0.396 and p = 0.313, respectively).
Patients showed an overall significant improvement in QoL after PAE (Figure 2). The mean QoL score was 5.5 with a median score of 6.0 prior to embolization and 1.8 and 1.0 after embolization, respectively (p < 0.001). One outlier had a prior median QoL score of 0 as the patient presented with acute obstruction within 1 month of PAE.
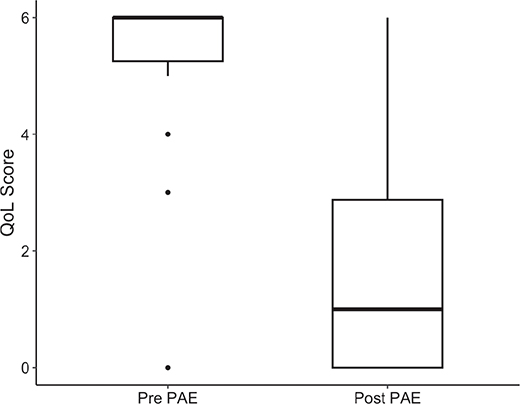
Figure 2. Quality of life (QoL) score before and after prostate artery embolization (n = 34). Box = 25th and 75th percentiles; lines show minimum and maximum values (1.5 * IQR); bold line = median. Outliers are presented as black circles. Abbreviations: PAE: prostate artery embolization; IQR: interquartile range; QoL: quality of life.
We found no alternative etiology among patients who showed no clinical improvement in IPSS score after PAE, such as bladder stones or urinary bladder diverticulum. Larger prostate volume was a significant risk factor for poorer outcome (p = 0.0159).
Two patients who underwent unilateral embolization showed no clinical improvement. However, unilateral embolization was not a statistically significant risk factor for poorer outcome in IPSS (p = 0.0624). Four patients (12%) without any clinical improvement following PAE required surgical intervention, with a mean duration of 27.1 months after PAE. Notably, no patient underwent surgical intervention or re-embolization due to symptomatic recurrence after clinically successful bilateral embolization during the follow-up period.
We observed post-procedural complications among three patients (Table 3). One patient had two documented complications. The majority of these are widely considered minor; however, one patient had acute tubular necrosis following embolization. Ten patients experienced PES, most commonly post-procedural bladder spasm, fever, and pelvic pain. All patients with adverse events and/or complications recovered without any lasting effects. Three patients with PES were treated with a short course of corticosteroids with favorable clinical response.
Discussion
In our cohort, PAE resulted in significant improvement in both IPSS and QoL scores, consistent with previously reported results [5, 17, 22], although our follow-up ranged widely.
Nearly half of the patients were dependent on a urinary catheter prior to PAE, with the majority achieving complete catheter freedom. These findings are compatible with recently published studies of PAE where most patients achieved catheter freedom [5, 17, 23]. These findings may prove particularly beneficial, as these patients are often less suitable for surgical treatment [2].
When stratified by follow-up periods, we observed a trend toward greater IPSS improvement beyond 24 months, although not statistically significant. This trend appeared to be sustained throughout the follow-up period. Notably, no patient in our cohort had reached a follow-up period beyond 5 years, where recurrence is more likely to occur [19–21].
Improvement in QoL was consistent with previous reports [22] and statistically significant across most follow-up periods. Unlike IPSS, no apparent trend was observed when stratified into follow-up periods.
Unilateral embolization showed a trend toward poorer outcome in our cohort, and is recognized as an independent risk factor for poorer outcome [24]. However, we observed only a borderline p-value, which is likely attributed to a small sample size.
Adverse events were uncommon, although PES was observed in nearly one-third of patients. We considered PES as an expected postprocedural event rather than a true complication [25]. Among adverse events, we found one major adverse effect, acute tubular necrosis, likely secondary to contrast-induced nephropathy [26]. However, all patients recovered without any long-term lasting effects.
Recall bias is a major limitation to this study as patients attempt to estimate urological symptoms retrospectively months or even years prior. Another significant limitation is the small cohort size and the retrospective study design, which becomes even more apparent when subjects are divided into different follow-up periods.
Conclusion
In our cohort, PAE was effective and safe in the treatment of BPH, resulting in significant improvements in both IPSS and QoL scores from baseline. Additionally, this study highlights that PAE may offer catheter freedom in the majority of patients. These effects were sustained throughout our follow-up period.
Author contributions
The corresponding author made substantial contributions to the acquisition of the data and data analysis. The corresponding author performed statistical analysis and drafted the manuscript. Fernando Bazan made contributions to the data acquisition and manuscript. All other authors made revisions of the manuscript.
References
- [1] Lee CL, Kuo HC. Pathophysiology of benign prostate enlargement and lower urinary tract symptoms: Current concepts. Tzu Chi Med J. 2017;29(2):79–83. https://doi.org/10.4103/tcmj.tcmj_20_17
- [2] Naidu SG, Narayanan H, Saini G, et al. Prostate artery embolization-review of indications, patient selection, techniques and results. J Clin Med. 2021;10(21). https://doi.org/10.3390/jcm10215139
- [3] Davis C, Golzarian J, White S, et al. Development of research agenda in prostate artery embolization: summary of society of interventional radiology consensus panel. J Vasc Interv Radiol. 2020;31(1):108–113. https://doi.org/10.1016/j.jvir.2019.09.019
- [4] Fujimura T, Kume H, Nishimatsu H, et al. Assessment of lower urinary tract symptoms in men by international prostate symptom score and core lower urinary tract symptom score. BJU Int. 2012;109(10):1512–1516. https://doi.org/10.1111/j.1464-410X.2011.10445.x
- [5] Majbar E, Swanberg J, Alamdari F, et al. Early experience of prostate artery embolization: a retrospective single-centre study. Scand J Urol. 2025;60:1–7. https://doi.org/10.2340/sju.v60.42495
- [6] Bhatia A, Porto JG, Maini A, et al. One-year outcomes after prostate artery embolization versus laser enucleation: a network meta-analysis. BJUI Compass. 2024;5(2):189–206. https://doi.org/10.1002/bco2.302
- [7] Stenmark F, Brudin L, Kjölhede H, et al. Treatment with CoreTherm in 570 patients with prostate volumes of 80–366 ml: an evaluation of short- and long-term retreatment risk. Scand J Urol. 2022;56(4):336–341. https://doi.org/10.1080/21681805.2022.2108139
- [8] Arch A, Thamsborg A, Winck-Flyvholm L, et al. Thermo-expandable intraprostatic nitinol stents in the treatment of bladder outlet obstruction: a consecutive case series. Scand J Urol. 2024;59:169–172. https://doi.org/10.2340/sju.v59.41991
- [9] Salmivalli A, Boström P, Nurminen P, et al. National trends of surgery for benign prostatic hyperplasia in Finland. Scand J Urol. 2024;59:70–75. https://doi.org/10.2340/sju.v59.32425
- [10] Stenmark F, Brundin L, Gunnarsson O, et al. A randomised study of TURP after intraprostatic injection of mepicacaine/adrenaline versus regular TURP in patients with LUTS/BPO. Scand J Urol. 2023;58:46–51. https://doi.org/10.2340/sju.v58.7798
- [11] Carnevale FC, Antunes AA, da Motta Leal Filho JM, et al. Prostatic artery embolization as a primary treatment for benign prostatic hyperplasia: preliminary results in two patients. Cardiovasc Intervent Radiol. 2010;33(2):355–361. https://doi.org/10.1007/s00270-009-9727-z
- [12] Yu H, Isaacson AJ, Burke CT. Review of current literature for prostatic artery embolization. Semin Intervent Radiol. 2016;33(3):231–235. https://doi.org/10.1055/s-0036-1586141
- [13] Elkoushy MA, Elhilali MM. Management of benign prostatic hyperplasia larger than 100 ml: simple open enucleation versus transurethral laser prostatectomy. Curr Urol Rep. 2016;17(6):44. https://doi.org/10.1007/s11934-016-0601-7
- [14] Xiang P, Guan D, Du Z, et al. Efficacy and safety of prostatic artery embolization for benign prostatic hyperplasia: a systematic review and meta-analysis of randomized controlled trials. Eur Radiol. 2021;31(7):4929–4946. https://doi.org/10.1007/s00330-020-07663-2
- [15] Swärd J, Bohlin K, Henrikson O, et al. Long-term efficacy of selective arterial embolisation of renal angiomyolipoma. Scand J Urol. 2023;58:86–92. https://doi.org/10.2340/sju.v58.12318
- [16] Dias US, Jr, de Moura MRL, et al. Prostatic artery embolization: indications, preparation, techniques, imaging evaluation, reporting, and complications. Radiographics. 2021;41(5):1509–1530. https://doi.org/10.1148/rg.2021200144
- [17] Lindgren H, Bläckberg M. Introduction of prostate artery embolization (PAE) in Sweden. Scand J Urol. 2019;53(2–3):151–155. https://doi.org/10.1080/21681805.2019.1610494
- [18] Kuang M, Vu A, Athreya S. A systematic review of prostatic artery embolization in the treatment of symptomatic benign prostatic hyperplasia. Cardiovasc Intervent Radiol. 2017;40(5):655–663. https://doi.org/10.1007/s00270-016-1539-3
- [19] Leng B, Zhou CG, Liu S, et al. Prostatic artery embolization to achieve freedom from catheterization in patients with acute urinary retention caused by benign prostatic hyperplasia. J Vasc Interv Radiol. 2021;32(7):1062–1067. https://doi.org/10.1016/j.jvir.2021.03.530
- [20] Pisco JM, Bilhim T, Pinheiro LC, et al. Medium- and long-term outcome of prostate artery embolization for patients with benign prostatic hyperplasia: results in 630 patients. J Vasc Interv Radiol. 2016;27(8):1115–1122. https://doi.org/10.1016/j.jvir.2016.04.001
- [21] Bilhim T, Costa NV, Torres D, et al. Long-term outcome of prostatic artery embolization for patients with benign prostatic hyperplasia: single-centre retrospective study in 1072 patients over a 10-year period. Cardiovasc Intervent Radiol. 2022;45(9):1324–1336. https://doi.org/10.1007/s00270-022-03199-8
- [22] Wang XY, Chai YM, Huang WH, et al. Prostate artery embolization on lower urinary tract symptoms related to benign prostatic hyperplasia: a systematic review and meta-analysis. World J Clin Cases. 2022;10(32):11812–11826. https://doi.org/10.12998/wjcc.v10.i32.11812
- [23] Insausti I, Galbete A, Lucas-Cava V, et al. Prostatic Artery Embolization (PAE) using polyethylene glycol microspheres: safety and efficacy in 81 patients. Cardiovasc Intervent Radiol. 2022;45(9):1339–1348. https://doi.org/10.1007/s00270-022-03165-4
- [24] Xu ZW, Zhou CG, Tian W, et al. Long-term efficacy and recurrence prediction of prostatic artery embolization for lower urinary tract symptoms secondary to benign prostatic hyperplasia. Cardiovasc Intervent Radiol. 2022;45(12):1801–1809. https://doi.org/10.1007/s00270-022-03272-2
- [25] Svarc P, Taudorf M, Nielsen MB, et al. Postembolization syndrome after prostatic artery embolization: a systematic review. Diagnostics (Basel). 2020;10(9). https://doi.org/10.3390/diagnostics10090659
- [26] Shuka N, Hasimi E, Kristo A, et al. Contrast-induced nephropathy in interventional cardiology: incidence, risk factors, and identification of high-risk patients. Cureus. 2023;15(12):e51283. https://doi.org/10.7759/cureus.51283