ORIGINAL RESEARCH ARTICLE
Women with isolated acute cystitis and macroscopic haematuria. Is further investigation needed?
Rula Hassana, Rasmus Ljungstedtb, Elsa Ågrena, Salome Olssonc, Emad Sabirb and Suleiman Abuhasaneina,d,e
aDepartment of Surgery, Urology Section, NU-Hospital Group, Uddevalla, Region Västra Götaland, Sweden; bDepartment of Urology, Varberg/Halmstad Hospital, Region Halland, Sweden; cDepartment of Pediatrics, Queen Silvia Children’s Hospital, Sahlgrenska University Hospital, Gothenburg, Sweden; dDepartment of Urology, Institute of Clinical Science, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden; eDepartment of Research and Development, NU-Hospital Group, Trollhättan, Region Västra Götaland, Sweden
ABSTRACT
Objective: To determine if women aged 50–70 years with a single episode of isolated acute haemorrhagic cystitis have a significantly lower risk of developing urological cancers, potentially indicating that further evaluation for macroscopic haematuria may be unnecessary.
Materials and methods: A retrospective study was conducted on all women assessed for macroscopic haematuria at two participating centres in Sweden between 2020 and 2022. The standard evaluation included computed tomography urography and cystoscopy. Patients were divided into two groups: AHG (acute haemorrhagic cystitis group), which was defined by the presence of macroscopic haematuria and symptoms resembling acute cystitis (dysuria, frequency or urgency), and non-AHG (non-acute haemorrhagic cystitis group), consisting of women with chronic, complicated or recurrent irritative symptoms or no cystitis-like symptoms at all. The characteristics of the women and their tumours were documented.
Results: A total of 1,084 women were evaluated for macroscopic haematuria. The median age was 67 years, with 652 women (60%) aged 50–70. Urological malignancies were detected in 71 women (7%). In the younger group, the AHG had a low cumulative cancer incidence (1%), whereas the non-AHG had a significantly higher rate (10%), P < 0.001. Asymptomatic haematuria showed the highest cumulative cancer incidence (11%). A multivariable Cox regression analysis (for all patients in the study) indicated that women in non-AHG have a seven-fold higher risk of developing urological cancer over time than women in AHG (hazard ratio [HR]: 7.19; 95% confidence interval [CI]: 3.64–14.21; P < 0.001).
Conclusion: Women aged 50–70 years with isolated acute haemorrhagic cystitis have a significantly low risk of urological malignancies, indicating that invasive investigations, such as cystoscopy and computed tomography urography, may not always be necessary. Nonetheless, further large-scale prospective studies are needed to validate these findings.
KEYWORDS: Computed tomography urography; cystitis; cystoscopy; female; haematuria; standardised care pathway; urinary tract infection; urological malignancy; woman
Citation: Scandinavian Journal of Urology 2025, VOL. 60, 195–203. https://doi.org/10.2340/sju.v60.44702.
Copyright: © 2025 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 26 March 2025; Accepted: 19 August 2025; Published: 13 October 2025
CONTACT: Suleiman Abuhasanein suleiman.abuhasanein@gu.se Department of Urology Institute of Clinical Science, Sahlgrenska Academy, University of Gothenburg, 413 90 Göteborg, Sweden
Supplemental data for this article can be accessed online at https://doi.org/10.2340/sju.v60.44702
Competing interests and funding: The authors have no conflict of interest to declare.
This study was supported by grants from the Department of Research and Development, NU-Hospital Group.
Introduction
Macroscopic haematuria is the primary symptom of urinary bladder cancer [1]. In Sweden, approximately 220 per 100,000 individuals are referred annually to a urologist for macroscopic haematuria evaluation [2]. In 2016, Sweden introduced a nationwide standardised care pathway (SCP) specifically for patients aged 50 years or older presenting with macroscopic, but not microscopic, haematuria. The pathway ensures timely diagnostic evaluation, including cystoscopy, computed tomography urography and urine cytology [3–5]. Significantly, Sweden’s selective policy of not investigating microscopic haematuria has not been associated with decreased survival amongst patients with urinary bladder cancer [6].
Cystoscopy and computed tomography urography are time-consuming procedures with known risks [7–9], and excessive examination of macroscopic haematuria imposes a significant financial burden on healthcare facilities [10]. A single nephrographic-phase dual-energy Computed Tomography (CT) may be adequate for assessing such patients, potentially simplifying the diagnostic process [11]. Additionally, efforts to enhance Computed Tomography Urography (CTU) image analysis using AI models have shown promising results, demonstrating high detection rates and excellent negative predictive value (NPV) in identifying urinary bladder cancer [12].
Notably, up to 83% of patients undergoing routine evaluations for macroscopic haematuria do not have an underlying urological malignancy [3]. However, many women with macroscopic haematuria also suffer from urinary tract infections (UTIs), particularly acute haemorrhagic cystitis, which is characterised by bladder mucosal bleeding and irritative symptoms such as dysuria, frequency or urgency [13]. Since more than 50% of women are likely to experience at least one UTI in their lifetime, acute haemorrhagic cystitis poses a significant challenge [14–16]. Although some researchers argue that acute haemorrhagic cystitis represents a benign condition, given the low likelihood of urological malignancies in individuals aged 75 years or younger [17], others have identified a link between UTI treatments and delayed urinary bladder cancer diagnosis [14], highlighting a gap in knowledge in this regard.
Therefore, this study aimed to determine whether women aged 50–70 years with a single episode of isolated acute cystitis accompanied by macroscopic haematuria (acute haemorrhagic cystitis) have a low enough risk of urological cancer to justify a more targeted approach to further tests, potentially reducing the need for invasive procedures such as cystoscopy and computed tomography urography.
Material and methods
Patients
A cohort study with a retrospective, observational and longitudinal design was conducted. This study incorporated all women undergoing assessments for macroscopic haematuria at two Swedish medical centres: the NU-Hospital Group/Uddevalla (September 2020–December 2022) and Hallands Hospital (June 2021–December 2022). The inclusion criteria were one or more episodes of macroscopic haematuria in women aged 50 years or older.
The standard investigation involved computed tomography urography and flexible cystoscopy; however, urinary cytology was not routinely performed in all centres. We selected a limit of 50 years because it resembles the existing SCP criteria. A cut-off age of 70 years was selected based on clinical experience and previous studies, indicating a low risk of urological malignancy in patients with macroscopic haematuria within this age range [18]. The investigation was deemed negative if no malignant urological abnormalities were detected by the end of the study period, which encompassed any subsequent diagnoses of urinary bladder cancer, upper tract urothelial carcinoma (UTUC) or kidney cancer.
Definitions
Women were classified as having an acute haemorrhagic cystitis if they experienced macroscopic haematuria accompanied by an acute-onset of irritative cystitis-like symptoms, such as dysuria, frequency or urgency, less than 1 week before the haematuria episode. Moreover, a urine dipstick test was considered positive if either leukocytes or nitrites were detected (any trace of nitrites or leukocytes was classified as positive). Furthermore, a urine culture was considered valid if it was performed during the initial visit for acute haemorrhagic cystitis. Thus, a patient was classified as lab-positive if she had either a positive urine dipstick test or a positive urine culture (Table 2).
Data analysis
Consequently, the study cohort was divided into two main groups: the acute haemorrhagic cystitis group (AHG), which consisted of women with macroscopic haematuria accompanied by short-term irritative cystitis-like symptoms (dysuria, frequency or urgency), and the non-acute haemorrhagic cystitis group (non-AHG), which included all other women with macroscopic haematuria. The non-AHG included patients with chronic irritative symptoms (lasting more than 4 weeks), recurrent UTIs (defined as at least two UTIs within 6 months or three or more within 1 year), febrile UTIs or cases where no irritative cystitis-like symptoms presented [19].
The rationale for grouping all women with short-term irritative symptoms together, regardless of laboratory results, and distinguishing between acute-onset and other cases is based on the fact that diagnosing acute cystitis and initiating antibiotic treatment primarily rely on symptoms rather than routine urine testing (urine dipstick or urine culture). According to the European Association of Urology (EAU) guidelines, acute cystitis can be diagnosed with a high probability based solely on a focused history of lower urinary tract symptoms, as urine culture and/or urine dipstick only provide a minimal increase in diagnostic accuracy [13, 19]. Similarly, the Swedish Strategic Program Against Antibiotic Resistance, known as The Swedish Strategic Program Against Antibiotic Resistance (STRAMA), also notes that in non-pregnant women, a high likelihood of acute cystitis exists when at least two severe irritative cystitis-like symptoms, such as burning during urination, frequency or urgency, are present without vaginal symptoms. In such cases, antibiotics should be immediately prescribed without the need for prior urine testing [20].
Subgroup analysis was performed by further analysing non-AHG subgroups separately, including women without irritative symptoms (asymptomatic haematuria) in one subgroup and those with chronic irritative symptoms and/or recurrent UTIs and/or febrile UTIs as another subgroup (complex haematuria). Patient characteristics were registered at the initial assessment for macroscopic haematuria. All study data were retrospectively collected through a review of medical records conducted by experienced physicians, who were blinded to the subsequent analysis and patient group allocation. The irritative symptoms examined in this study were initially evaluated by a physician and documented in the patient’s medical record. Details regarding tumour characteristics, such as the number of tumours, size, tumour grade and tumour-node-metastasis (TNM) classification, were documented for women diagnosed with urological malignancy.
Descriptive statistics were used to summarise the study characteristics and outcomes. Continuous variables were compared using the Mann–Whitney test, whereas categorical data were analysed using the chi-square test. Continuous data were presented as medians with interquartile ranges (IQRs). Univariable and multivariable Cox proportional hazards analyses were performed to evaluate time to events in relation to potential risk factors, including age, grouping into AHG versus non-AHG, radiotherapy and smoking status. For this analysis, the observation period started at the onset of macroscopic hematuria. It ended when a urological malignancy was identified, the patient died, follow-up was no longer possible, or the data were censored on September 30, 2024, whichever occurred first. The median follow-up time was calculated using the reverse Kaplan-Meier method. P-values < 0.05 were considered statistically significant. Statistical analysis was performed using SPSS version 29 (IBM Corp., Armonk, NY, USA).
Results
During the study period, 2,618 patients were evaluated for macroscopic haematuria according to SCP, including 1,084 women (41%), all of whom were included in this study (Figure 1). Patient data were retrospectively collected from electronic medical records, with a median follow-up period of 32 months (interquartile range, IQR, 25–38). This study included 677 women (63% from the NU-Hospital Group) and 402 women (37% from Halland Hospital). The median age was 67 years (IQR 58–76), with 652 women (60%) aged between 50 and 70 years.

Figure 1. Flow chart of patients included in the study.
Cystoscopy was performed in 1,070 women (99%), revealing normal findings in 675 women (63%), whilst benign lesions, such as cystitis-like changes, bladder stones, cystitis cystica or bladder diverticula, were observed in 340 women (32%). Urological malignancies were detected in 71 women (7%), including urinary bladder cancer in 53 women (5%), and both UTUC and kidney cancer in nine women each (1%).
Amongst women aged 50–70, urological malignancies were less common (4%, 27/652) compared with those over 70 (10%, 43/427). Muscle-invasive (T2+) bladder tumours were found in 22.5% of cases in the younger group and 29% in the older group (Table 1; Supplementary Tables 1 and 2). In the 50–70 age group, urological malignancies were found in only 1% (5/429) of AHG compared with 10% (21/223) in the non-AHG group (P < 0.001). Only five women (1%) in the AHG were diagnosed with urological malignancies, including two women of solitary urinary bladder cancer (TaG1–2 tumours < 3 cm) and three cases of kidney cancer, two with T2 tumours and one under active surveillance for a small renal mass. In contrast, urological malignancies were found in 22 women (10%) in the non-AHG (Table 3, Figure 2A).
| Variable name | 50–70 years | > 70 years | All | |
| No. patients | % of the row | 652 (60) | 427 (40) | 1079 |
| Age (years) | Median (IQR) | 60 (55–65) | 77 (74–82) | 66 (58–76) |
| Hospital | NU-Hospital Group | 405 (62) | 272 (64) | 677 (63) |
| Hallands Hospital | 247 (38) | 155 (37) | 402 (37) | |
| Smoking* | Never smoker | 323 (50) | 264 (63) | 587 (55) |
| Current or former smoker | 319 (50) | 153 (37) | 472 (45) | |
| Time of smoking (for both former and current smokers) | Median (IQR) years | 20 (10–30) | 22 (10–40) | 20 (10–30) |
| Radiotherapy | Yes | 17 (3) | 15 (4) | 32 (3) |
| Irritative cystitis-like symptoms | Yes | 498 (76) | 254 (60) | 752 (70) |
| Fever | Yes | 24 (4) | 14 (3) | 38 (4) |
| Urine dipstick | Yes | 472 (73) | 285 (70) | 757 (72) |
| Urine dipstick results | Positive for leukocytes | 357 (76) | 214 (75) | 570 (76) |
| Positive for nitrite | 84 (18) | 73 (26) | 157 (21) | |
| Positive urine dipstick** | 370 (57) | 231 (54) | 601 (56) | |
| Urine culture | Yes | 286 (44) | 191 (47) | 476 (46) |
| Urine culture results | Positive | 123 (45) | 87 (48) | 210 (46) |
| Positive laboratory results*** | 395 (61) | 260 (61) | 655 (61) | |
| Symptoms groups | AHG | 429 (66) | 196 (46) | 625 (58) |
| Non-AHG | 223 (34) | 231 (54) | 454 (42) | |
| Cystoscopy results | Not done**** | 3 (1) | 6 (1) | 9 (1) |
| Normal findings | 427 (67) | 238 (56) | 675 (63) | |
| Other benign findings | 191 (29) | 149 (35) | 340 (31) | |
| Papillomatous lesions | 21 (3) | 34 (8) | 55 (5) | |
| Investigation results***** | No uro-malignancy | 625 (96) | 383 (90) | 1008 (93) |
| Urinary bladder cancer | 22 (3) | 31 (7) | 53 (5) | |
| UTUC | 2 (0.5) | 7 (1.5) | 9 (1) | |
| Kidney cancer | 3 (0.5) | 6 (1.5) | 9 (1) | |
| Tumour stage of urinary bladder cancer | TaG1–2 | 12 (55) | 13 (42) | 25 (47) |
| TaG3 – Cis – T1 | 5 (22.5) | 9 (29) | 14 (26.5) | |
| T2+ | 5 (22.5) | 9 (29) | 14 (26.5) | |
| Tumour stage of UTUC | TaG1–2 | 1 (50) | 1 (14) | 2 (22) |
| TaG3 – Cis – T1 | 1 (50) | 1 (14) | 2 (22) | |
| T2+ | 0 (0) | 5 (72) | 5 (56) | |
| Tumour stage of kidney cancer | T1–2 | 2 (67) | 2 (33) | 4 (45) |
| T3+ | 0 (0) | 2 (33) | 2 (22) | |
| Not biopsied****** | 1 (33) | 2 (33) | 3 (33) | |
| Number of urinary bladder cancer lesions | Solitary | 16 (73) | 23 (74) | 39 (74) |
| Tumour size of (cm) | ≤ 3 cm | 17 (77) | 22 (71) | 39 (74) |
| The table represents the number of patients (% of the row) if not otherwise indicated. (AHG: acute haemorrhagic cystitis group, IQR: interquartile range, non-AHG: non-acute haemorrhagic cystitis group, Cis: carcinoma in situ, TNM: tumour, node, metastasis, UTUC: upper tracts urothelial carcinoma). *Patients with missing results n = 20 **Either positive leukocytes or nitrite in urine dipstick, or both ***Either positive urine dipstick or urine culture ****Computed tomography urography was done in these cases *****After both cystoscopy and computed tomography urography in almost all patients ******Under active surveillance |
||||
| Variable name | AHG | Non-AHG | p-value | |
| No. patients | % of the row | 429 (66) | 223 (34) | |
| Age (years) | Median (IQR) | 59 (54–64) | 60 (56–65) | 0.006 |
| Smoking* | Never smoker | 224 (53) | 99 (45) | 0.052 |
| Current or former smoker | 198 (47) | 121 (55) | ||
| Radiotherapy | Yes | 7 (2) | 10 (5) | 0.030 |
| Cystoscopy results | Not done | 3 (0.5) | 0 (0) | < 0.001 |
| Normal findings | 280 (65) | 157 (70) | ||
| Other benign findings | 144 (34) | 47 (21) | ||
| Papillomatous lesions | 2 (0.5) | 19 (9) | ||
| Investigation results** | No uro-malignancy | 424 (99) | 201 (90) | < 0.001 |
| Urinary bladder cancer | 2 (0.5) | 20 (9) | ||
| UTUC | 0 (0) | 2 (1) | ||
| Kidney cancer | 3 (0.5) | 0 (0) | ||
| Tumour stage of urinary bladder cancer | TaG1–2 | 2 (100) | 10 (50) | 0.400 |
| TaG3 – Cis – T1 | 0 (0) | 5 (25) | ||
| T2+ | 0 (0) | 5 (25) | ||
| Tumour stage of UTUC | TaG1–2 | 0 (0) | 1 (50) | *** |
| TaG3 – Cis – T1 | 0 (0) | 1 (50) | ||
| Tumour stage of kidney cancer | T1–2 | 2 (67) | 0 (0) | *** |
| Not biopsied**** | 1 (1) | 0 (0) | ||
| Number of urinary bladder cancer lesions | Solitary | 2 (100) | 14 (70) | 0.364 |
| Tumour size (cm) | ≤ 3 cm | 2 (100) | 15 (75) | 0.421 |
| Table represents number of patients (% of the row) if not otherwise indicated (AHG: acute haemorrhagic cystitis group, IQR: interquartile range, non-AHG: non-acute haemorrhagic cystitis group, Cis: carcinoma in situ, TNM: tumour, node, metastasis, UTUC: upper tracts urothelial carcinoma). *Patients with missing results n = 10 **After both cystoscopy and computed tomography urography ***Not applicable ****Under active surveillance |
||||
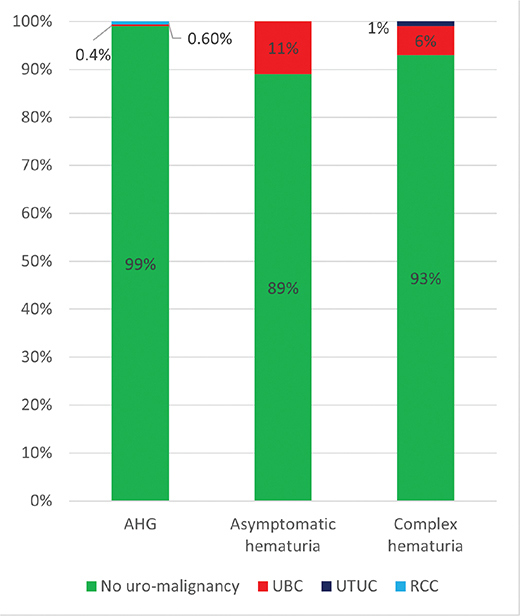
Figure 2. (A) The distribution of urological malignancies amongst women aged 50–70 years with macroscopic haematuria across the study groups, including those with acute haemorrhagic cystitis symptoms (AHG), and those in the non-AHG (non-acute haemorrhagic cystitis symptoms) subgroups with asymptomatic haematuria and those with complex haematuria.
The asymptomatic haematuria group had the highest cumulative cancer incidence, with 17 women (11%) aged 50–70 years diagnosed with urological malignancies versus 32 women (18%) aged > 70 years. Finally, amongst women with complex haematuria, urological malignancies were diagnosed in five women (7%) in the younger age group and seven women (12%) in the older age group (Supplementary Tables 1 and 2).
The age-stratified cumulative cancer incidence of urological malignancies across the study groups indicates that age is a significant risk factor, with older women facing a higher risk of developing urological malignancies. In AHG, the cumulative cancer incidence was very low amongst younger women, with a slight increase observed in those aged 80 and above. In contrast, non-AHG demonstrated a clear trend of progressively increasing risk of developing urological malignancies with advancing age (Figure 2B).

Figure 2. (B) Age-stratified cumulative cancer incidence of urological malignancies in all women in the study with macroscopic haematuria across the study’s groups including those with acute haemorrhagic cystitis symptoms (AHG), those in the non-AHG (non-acute haemorrhagic cystitis symptoms) subgroups with asymptomatic haematuria and those with complex haematuria.
The Cox regression analysis of all patients in the study (including those under and over 70 years) revealed that age was significantly associated with risk of developing urological cancers, with each additional year increasing the hazard by 5% in the univariable model (hazard ratio [HR]: 1.05, 95% confidence interval [CI]: 1.03–1.07, P < 0.001) and by 3% in the multivariable model (HR: 1.03, 95% CI: 1.01–1.06, P = 0.006). Belonging to the non-AHG was strongly associated with an elevated risk compared with the AHG, with an HR of 8.59 (95% CI: 4.39–16.76, P < 0.001) in the univariable model and 7.19 (95% CI: 3.64–14.21, P < 0.001) in the multivariable model. Smoking was a significant predictor in the multivariable model (HR: 1.69, 95% CI: 1.02–2.79, P = 0.040), indicating increased risk amongst current or former smokers (Table 4).
| Variable name | Nr. | HR Univariable (95%CI) | Nr. | HR Multivariable (95%CI) | |
| Age* | 1 079 | 1.05 (1.03–1.07) | 1 059 | 1.03 (1.01–1.06) | |
| Symptoms groups | AHG | 625 | 1 (ref) | 615 | 1 (ref) |
| Non-AHG | 454 | 8.59 (4.39–16.76) | 444 | 7.19 (3.64–14.21) | |
| Smoking** | Never smoker | 587 | 1 (ref) | 587 | 1 (ref) |
| Current or former smoker | 472 | 1.29 (0.79–2.08) | 472 | 1.69 (1.02–2.79) | |
| Radiotherapy*** | No | 1 047 | 1 (ref) | 1 027 | 1 (ref) |
| Yes | 32 | 0.04 (0.00–20.63) | 32 | 0.0 (0.0–0.0) | |
| (AHG: acute hemorrhagic cystitis group, CI: confidence interval, HR: hazard ratio, and non-AHG: non-acute hemorrhagic cystitis group, Nr. the number of patients at risk) HRs were calculated using Cox proportional hazards regression models. For age, HR reflects the change per one-year increase. (Ref) indicates the reference category in categorical comparisons. *Age is a continuous variable **20 missed values |
|||||
Discussion
This retrospective study included 1,084 women evaluated for macroscopic haematuria, amongst whom urological malignancies were identified in 71 cases (7%), with urinary bladder cancer being the most common (53/71, 75%). Notably, amongst younger women, the AHG exhibited a significantly lower cumulative cancer incidence (n = 5, 1%) than the non-AHG (n = 22, 10%), P < 0.001. These findings suggest that foregoing further investigation according to the SCP protocol may be a reasonable approach for women in the AHG. This strategy could spare 40% of women who undergo cystoscopy and computed tomography urography for macroscopic haematuria (429/1,079), representing 16% of the total study cohort (429/2,618), from undergoing these invasive procedures. By tailoring investigations for these women, healthcare systems can reduce the burden of unnecessary invasive procedures, thereby minimising patient discomfort, procedural complications and financial costs.
Three women with kidney cancer were identified in the AHG, raising the question of whether these tumours were the actual cause of macroscopic haematuria or if the bleeding originated from haemorrhagic cystitis, with the kidney tumours being incidental findings. Although early cancer detection can be beneficial, it raises concerns about overdiagnosis [21]. Notably, one-third of these women had a small kidney mass that required neither biopsy nor intervention. These findings underscore the need for a more nuanced approach to evaluate macroscopic haematuria, striking a balance between early detection and the risk of overdiagnosis.
Our findings are consistent with those of Malmström et al. [6], who showed that abandoning testing for asymptomatic microscopic haematuria did not adversely affect urinary bladder cancer outcomes in Sweden. Both their study and ours emphasise that reducing unnecessary urological investigations – whether for asymptomatic microscopic haematuria or isolated acute haemorrhagic cystitis – can alleviate patient burden and lower healthcare costs without compromising cancer detection or survival. This supports a more targeted approach to haematuria evaluation, emphasising the need for further large-scale prospective studies to optimise clinical guidelines.
A clinical presentation involving complex haematuria and/or a history of recurrent UTIs was associated with a higher risk of urothelial malignancies, aligning with the findings of Liedberg et al. [14]. They investigated the relationship between UTIs and delayed urinary bladder cancer diagnosis in a large cohort of 29,921 patients with urinary bladder cancer and 149,467 matched references. They showed a higher risk of muscle-invasive or metastatic urinary bladder cancer in relation to at least one prescription of prediagnostic antibiotics indicated for UTI treatment, 1.42 (95% CI 1.27–1.58). Moreover, the risk increased with the number of UTI treatments, suggesting a possible delay in diagnosis. However, some clinical/laboratory details, such as irritative urinary symptoms, urine testing results and other relevant signs accompanying macroscopic haematuria, were not included in the analysis, prompting further investigation. Additionally, UTI treatments within 90 days before urinary bladder cancer diagnosis were excluded, which could have affected the results by overlooking potentially relevant prediagnostic confounders. Our study helps bridge this critical clinical gap just before urinary bladder cancer diagnosis by offering valuable insights into this prediagnostic period, emphasising the importance of a more refined approach to assessing UTIs in the context of macroscopic haematuria.
Our results are also consistent with a previous report, showing that the predictive value of macroscopic haematuria was below 1% in patients aged 75 years or younger with concomitant bacteriuria, prompting the authors to advise against further urological evaluation in these cases [17]. Vasdev et al. [22] had evaluated 1,740 patients at a one-stop fast-track haematuria clinic in 2003–2006, including 673 women. Amongst 330 patients with a positive urine culture and a subsequent negative one after treatment, only three patients (1%) were found to have urological malignancies, which align with our results. However, this study concluded that the presence of a UTI does not reduce the likelihood of urologic malignancy. This conclusion may be influenced by the inclusion of a heterogeneous group comprising both men and women, as well as patients with both microscopic and macroscopic haematuria. Additionally, 14% of their cohort consisted of individuals under 40 years.
Vasdev et al. used urine culture as a key factor to differentiate between groups. In a subgroup of 161 patients who initially had a negative urine culture but later tested positive at the urology visit, 32 cases (20%) of urological malignancies were identified. They suggested that UTI should not be ruled out in further urological evaluation. However, it remains unclear whether these 20% were men or women, which is important because men have a higher risk of developing urological malignancies [18, 23, 24]. Furthermore, although these patients may not have had a bacterial infection during the haematuria episode, they were still categorised as having a positive urine culture, which may have impacted the study’s conclusions. In contrast, our study distinguished between patients with short-term irritative cystitis-like symptoms (AHG) and those with asymptomatic macroscopic haematuria, consistently demonstrating a significant difference in cancer detection rates (P < 0.001).
A well-founded and important concern that arises from previous reports is that women tend to present with more advanced tumours and have higher cancer-specific mortality, which may be linked to referral delays and inadequate adherence to diagnostic guidelines. Research indicates that women are more likely than men to require three or more consultations before being referred, possibly as a result of their symptoms being misinterpreted as uncomplicated haemorrhagic cystitis, not requiring further investigation [25, 26]. Additionally, different age groups are often treated similarly, with older women treated similarly to younger women, and those with chronic recurrent or persistent irritative symptoms grouped with those experiencing a single episode of acute haemorrhagic cystitis. In contrast, our study specifically distinguished between these two latter groups, demonstrating a clear difference in cumulative cancer incidence. One potential risk of excluding younger women with acute UTIs from the SCP is the increased likelihood that those with complicated UTIs may not be referred. Therefore, we strongly highlight the critical importance of referring women with complex or asymptomatic haematuria to the SCP, as the association with cancer in these groups is significantly higher than that in other groups.
An interesting finding was reported by Nilbert et al. [18], who compared patients with positive laboratory results (either a positive urine dipstick or urine culture) to those with negative laboratory results. They found that 20 out of 317 (6%) of women with positive laboratory results had urological malignancies, compared with 69 of 367 (19%) amongst those with negative laboratory results. Interestingly, applying the same approach to our study (regardless of the presence of symptoms) yields comparable figures: urological malignancies were found in 34 out of 655 women (5%) with positive laboratory results, compared with 37 out of 424 women (9%) with negative laboratory results.
However, Nilbert et al. did not categorise their study cohort based on symptom presentation; instead, they grouped all patients with positive laboratory results into a single category. In our study, we differentiated between acute irritative symptoms (AHG) and chronic or recurrent symptoms or even asymptomatic haematuria (non-AHG). We observed that women aged 50–70 with acute irritative symptoms (regardless of laboratory results) had only a 1% risk of cancer. In addition, the presence of chronic, recurrent, irritative symptoms, sometimes accompanied by fever or silent macroscopic haematuria, was a stronger predictor of cancer detection compared with isolated positive laboratory results alone.
Our findings are consistent with the growing body of evidence supporting the more selective use of invasive investigations in patients with haematuria. Tan et al. introduced the Haematuria Cancer Risk Score (HCRS) in combination with renal bladder ultrasound (RBUS) as a risk stratification tool, demonstrating that up to 25%–34% of patients could safely avoid cystoscopy whilst maintaining high sensitivity for cancer detection (97%) [27]. Similarly, our results suggest that women aged 50–70 years with isolated acute haemorrhagic cystitis have a significantly lower risk of urological malignancies and may not require routine cystoscopy or computed tomography urography, supporting the feasibility of a more tailored diagnostic approach.
Cox regression analysis of the entire cohort further reinforces the stratified cancer risk observed in different patient subgroups. Most notably, women in the non-AHG had a markedly elevated cancer risk, with a more than seven-fold increase compared with the AHG, even after adjustment for confounders (HR: 7.19; P < 0.001). Additionally, smoking emerged as a significant independent risk factor in the multivariable model, further supporting its role in urological carcinogenesis. These findings underscore the clinical utility of symptom-based categorisation and known risk factors in guiding the diagnosis of haematuria.
However, relying solely on laboratory tests may not always be a successful approach, as asymptomatic bacteriuria is present in more than 50% of women above the age of 80 [28], complicating cancer risk assessment in those with macroscopic haematuria and concurrent bacteriuria. However, considering symptoms alongside laboratory results provides a more transparent framework and better guidance. Short-term irritative symptoms might not automatically prompt further investigation. In contrast, chronic, recurrent urinary symptoms or febrile UTIs with haemorrhagic cystitis in women should warrant a prompt SCP evaluation, including cystoscopy and computed tomography urography.
A closer examination of biomarkers is essential to streamline the diagnostic process further, as their clinical and practical significance continues to evolve [29]. GeneXpert BC has a sensitivity of 0.94 (95% CI: 0.90–0.97) and an NPV of 0.99 (95% CI: 0.98–0.99). The use of this biomarker could potentially eliminate the need for cystoscopy and computed tomography urography in 44% of patients presenting with macroscopic haematuria [30]. Incorporating such tools into routine clinical practice is crucial for enhancing efficiency and improving patient outcomes. However, further research should investigate the clinical application of biomarkers to optimise the efficiency of macroscopic haematuria evaluations.
One of the strengths of this study was the inclusion of a large cohort of women aged 50 and older, allowing for a comprehensive analysis of the association between macroscopic haematuria and urological malignancies across a diverse range of clinical presentations. Moreover, data collection from two separate centres enhances the generalisability of the findings. Furthermore, this study provides new insights into the risk of uro-malignancy across different clinical subgroups by stratifying patients based on their symptom presentation.
However, our study has limitations. The retrospective nature of the study limits the ability to establish causality. It may introduce selection bias, as it only includes those who sought medical attention and had documented cases of macroscopic haematuria. Sweden’s quality registers remain valuable for monitoring care patterns and outcomes, supporting further research, such as on women with acute cystitis [31]. Additionally, variations in the completeness and quality of medical records could have impacted our findings. Moreover, only 72% of patients underwent urinalysis, and 46% had urine cultures performed, which may have affected the accurate classification of UTI-related cases. Standardising these tests would strengthen the study’s conclusions.
In conclusion, women aged 50–70 years with isolated acute haemorrhagic cystitis had a minimal risk of urological malignancies (1%), supporting the possibility of excluding them from SCP. Implementing this adjustment could spare 40% of women with macroscopic haematuria due to haemorrhagic cystitis from undergoing invasive procedures. However, it remains essential to provide a careful follow-up for women with persistent, complicated or recurrent symptoms to ensure early detection of potential malignancies. Larger prospective studies are still needed to confirm our findings and develop risk-adapted strategies for managing macroscopic haematuria in women.
Acknowledgements
The authors thank research assistant Anna Duverin and the staff in the urology departments at NU-Hospital Group and Halland Hospital for their technical support. The authors also thank statisticians Koen Simons and Viktor Tasselius for their valuable assistance with the statistical analyses.
Ethical approval
All authors declared that the research was conducted according to the principles of the World Medical Association Declaration of Helsinki ‘Ethical Principles for Medical Research Involving Human Subjects’. This study was approved by the Swedish Ethical Review Authority (File Nos. 2019-05582 and 2024-03846-01).
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author upon reasonable request.
References
- [1] Shapley M, Mansell G, Jordan, JL, et al. Positive predictive values of >/=5% in primary care for cancer: systematic review. Br J Gen Pract. 2010;60(578):e366–e377. https://doi.org/10.3399/bjgp10X515412
- [2] Abuhasanein S, Chaves V, Mohsen AM, et al. Diagnostic value of repeated comprehensive investigation with CT urography and cystoscopy for recurrent macroscopic haematuria. BJUI Compass. 2024;5(2):253–260. https://doi.org/10.1002/bco2.300
- [3] Liedberg F, Gerdtham U, Gralén K, et al. Fast-track access to urologic care for patients with macroscopic haematuria is efficient and cost-effective: results from a prospective intervention study. Br J Cancer. 2016;115(7):770–775. https://doi.org/10.1038/bjc.2016.265
- [4] Abuhasanein S, Jahnson S, Aljabery F, et al. Standardized care pathways for patients with suspected urinary bladder cancer: the Swedish experience. Scand J Urol. 2022;56(3):227–232. https://doi.org/10.1080/21681805.2022.2058605
- [5] Malmstrom PU, Skaaheim Haug E, Bostrom PJ, et al. Progress towards a Nordic standard for the investigation of hematuria: 2019. Scand J Urol. 2019;53(1):1–6. https://doi.org/10.1080/21681805.2018.1555187
- [6] Malmström PU, Truls G. Abandoning testing for asymptomatic microscopic haematuria in Sweden – a long-term follow-up. Scand J Urol. 2023;58:109–114. https://doi.org/10.2340/sju.v58.11142
- [7] Waisbrod S, Natsos A, Wettstein MS, et al. Assessment of diagnostic yield of cystoscopy and computed tomographic urography for urinary tract cancers in patients evaluated for microhematuria: a systematic review and meta-analysis. JAMA Network Open. 2021;4(5):e218409. https://doi.org/10.1001/jamanetworkopen.2021.8409
- [8] Tsapaki V, Rehani M, Saini S. Radiation safety in abdominal computed tomography. Semin Ultrasound CT MR. 2010;31(1):29–38. https://doi.org/10.1053/j.sult.2009.09.004
- [9] Georgieva MV, Wheeler SB, Erim D, et al. Comparison of the harms, advantages, and costs associated with alternative guidelines for the evaluation of hematuria. JAMA Intern Med. 2019;179(10):1352–1362. https://doi.org/10.1001/jamainternmed.2019.2280
- [10] Halpern JA, Chughtai B, Ghomrawi H. Cost-effectiveness of common diagnostic approaches for evaluation of asymptomatic microscopic hematuria. JAMA Intern Med. 2017;177(6):800–807. https://doi.org/10.1001/jamainternmed.2017.0739
- [11] Galtung KF, Lauritzen PM, Sandbaek G, et al. Computed tomography for visible haematuria – a single nephrographic phase is sufficient for detecting renal cell carcinoma. Scand J Urol. 2024;59:10–18. https://doi.org/10.2340/sju.v59.18467
- [12] Abuhasanein S, Edenbrandt L, Enqvist O, et al. A novel model of artificial intelligence based automated image analysis of CT urography to identify bladder cancer in patients investigated for macroscopic hematuria. Scand J Urol. 2024;59:90–97. https://doi.org/10.2340/sju.v59.39930
- [13] Kranz J, Bartoletti R, Bruyère F, et al. European Association of urology guidelines on urological infections: summary of the 2024 guidelines. Eur Urol. 2024;86(1):27–41. https://doi.org/10.1016/j.eururo.2024.03.035
- [14] Liedberg F, Gårdmark T, Hagberg O, et al. Treatment related to urinary tract infections is associated with delayed diagnosis of urinary bladder cancer: a nationwide population-based study. Eur Urol Oncol. 2025;8(1):119–125. https://doi.org/10.1016/j.euo.2024.07.008
- [15] D’Amico MJ, Foss H, Uhr A, et al. Hemorrhagic cystitis: a review of the literature and treatment options. Can J Urol. 2022;29(5):11276–11283.
- [16] McCue J. UTIs in at-risk patients: are they ‘complicated’? Infect Med. 1999;16(8):533–540.
- [17] Kulander O, Johansson J, Brudin L. [Low frequency of cancer in the urinary organs when macroscopic hematuria is associated with bacteriuria]. Lakartidningen. 2019;116(8):1–5. https://lakartidningen.se/klinik-och-vetenskap-1/artiklar-1/rapport/2019/02/lag-sannolikhet-for-cancer-i-urinorganen-vid-makroskopisk-hematuri-och-samtidig-bakteriuri/
- [18] Nilbert M, Bläckberg M, Ceberg J, et al. Diagnostic pathway efficacy for urinary tract cancer: population-based outcome of standardized evaluation for macroscopic haematuria. Scand J Urol. 2018;52(4):237–243. https://doi.org/10.1080/21681805.2018.1498124
- [19] Bonkat G, Bartoletti R, Bruyère F, et al. EAU guidelines on urological infections. EAU Guidelines Office, Arnhem, the Netherlands 2021.
- [20] Strama arbetsgrupp, F. Behandlingsrekommendationer för vanliga infektioner i öppenvård [Internet]. 2023. Available from: https://strama.se/behandlingsrekommendationer/ [cited December 2024]
- [21] Welch HG, Black WC. Overdiagnosis in cancer. J Natl Cancer Instit. 2010;102(9):605–613. https://doi.org/10.1093/jnci/djq099
- [22] Vasdev N, Thorpe AC. Should the presence of a culture-positive urinary tract infection exclude patients from rapid evaluation hematuria protocols? Urol Oncol. 2013;31(6):909–913. https://doi.org/10.1016/j.urolonc.2011.07.016
- [23] Jones R, Latinovic R, Charlton J, et al. Alarm symptoms in early diagnosis of cancer in primary care: cohort study using General Practice Research Database. BMJ. 2007;334(7602):1040. https://doi.org/10.1136/bmj.39171.637106.AE
- [24] Khadhouri S, Gallagher KM, MacKenzie KR, et al. The IDENTIFY study: the investigation and detection of urological neoplasia in patients referred with suspected urinary tract cancer – a multicentre observational study. BJU Int. 2021;128(4):440–450. https://doi.org/10.1111/bju.15483
- [25] Thorstenson A, Hagberg O, Ljungberg B, et al. Gender-related differences in urothelial carcinoma of the bladder: a population-based study from the Swedish National Registry of Urinary Bladder Cancer. Scand J Urol. 2016;50(4):292–297. https://doi.org/10.3109/21681805.2016.1158207
- [26] Lyratzopoulos G, Abel GA, McPhail S, et al. Gender inequalities in the promptness of diagnosis of bladder and renal cancer after symptomatic presentation: evidence from secondary analysis of an English primary care audit survey. BMJ Open. 2013;3(6):e002861. https://doi.org/10.1136/bmjopen-2013-002861
- [27] Tan WS, Ahmad A, Zhou Y, et al. Hematuria cancer risk score with ultrasound informs cystoscopy use in patients with hematuria. Eur Urol Oncol. 2025;8(1):87–93. https://doi.org/10.1016/j.euo.2024.05.005
- [28] Wagenlehner FM, Naber KG, Weidner W. Asymptomatic bacteriuria in elderly patients: significance and implications for treatment. Drugs Aging. 2005;22(10):801–807. https://doi.org/10.2165/00002512-200522100-00001
- [29] Flores Monar GV, Reynolds T, Gordon M, et al. Molecular markers for bladder cancer screening: an insight into bladder cancer and FDA-approved biomarkers. Int J Mol Sci. 2023;24(18):14374. https://doi.org/10.3390/ijms241814374
- [30] Abuhasanein S, Radmann J, Jahnson S, et al. Diagnostic performance of geneXpert BC as a triage test for patients presenting with macroscopic hematuria suspicious for urinary bladder cancer: a multicenter prospective case-control study. Eur Urol Open Sci. 2024;70:158–166. https://doi.org/10.1016/j.euros.2024.10.016
- [31] Stattin P. How to improve cancer care by use of guidelines and quality registers. Scand J Urol. 2024;59:190–192. https://doi.org/10.2340/sju.v59.42272