ORIGINAL ARTICLE
Association between symptoms of acute cystitis and findings of bladder cancer in the Swedish standardized pathway for macroscopic haematuria
Rami Shkair, Magnus Wagenius, Mats Bläckberg and Gustaf Starlander
Department of Urology, Helsingborg Hospital, Helsingborg, Sweden
ABSTRACT
Standardized Care Pathway (SCP) for patients presenting with macroscopic haematuria was introduced in Sweden in 2015. In contrast to neighbouring countries, the Swedish model includes all patients with macroscopic haematuria above the age of 50, notwithstanding obvious causes. The aim of this study was to characterize the patients referred within the SCP and the presence of acute cystitis.
All patients admitted to two regional hospitals in 2023, under the terms of SCP macroscopic haematuria, were included. Patient data were collected retrospectively regarding age, sex, symptoms of cystitis and cause of haematuria.
The study included 782 patients. The median age was 70 years and half were women. In 89 cases, a urinary tract cancer was found (11%) and 74 (9%) had bladder cancer. The cancer-positive group was significantly older (median 75 years) and 76% were men. Half of patients (51%) had symptoms of acute cystitis on referral. This was significantly associated with the absence of bladder cancer, but only in the age groups 50–69, where no case was found among patients with symptoms of cystitis. In the age groups above, 22 cancer-positive patients (30% of all bladder cancer cases) had symptoms of cystitis.
The Swedish SCP macroscopic haematuria targets younger female patients unproportionally, in comparison to where cancer is likely found. Neither symptoms of cystitis, nor positive urine cultures exclude bladder cancer in elderly, but clearly in the age groups 50–69. If excluding the latter from the SCP, a 28% reduction of examined patients can be achieved with a negligible risk of missing cancer.
KEYWORDS: Bladder cancer; cystitis; macroscopic hematuria; standardized care; pathway
Citation: Scandinavian Journal of Urology 2025, VOL. 60, 238–243. https://doi.org/10.2340/sju.v60.45026.
Copyright: © 2025 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 14 April 2025; Accepted: 23 October 2025; Published: 18 December 2025
CONTACT: Gustaf Starlander gustaf_starlander@hotmail.com Department of Urology, Helsingborg Hospital, Charlotte Yléns gata 10, 251 87 Helsingborg, Sweden
Introduction
Each year around 3,200 cases of bladder cancer are diagnosed in Sweden, giving an incidence of about 30/100,000. It is three to four times more common in men and has a median onset age of 76 years. Worldwide it is the 10th most common cancer, with the highest incidence in southern Europe, causing approximately 200,000 deaths annually [1]. The mortality has not decreased over the recent decades [2], despite advances in treatment, and this has partly been attributed to delays in urological examination and treatment. Patients searching primary care for macroscopic haematuria has a positive predictive value of approximately 6%–11% for urinary tract cancer [3], which is among the highest of any symptom for cancer. Despite this, urinary tract cancer has among the longest time from symptom to treatment [3]. To overcome this obstacle Fast Track Pathways or Standardized Care Pathways (SCPs), for rapid examination and treatment of patients presenting with macroscopic haematuria, have been introduced in a number of countries, including the United Kingdom (UK) and the Nordic countries [4]. The inclusion criteria for SCP referral vary between countries, both regarding age and symptoms. The Swedish SCP for cancer in the urinary bladder and upper urothelial tract (commonly referred to as SCP macroscopic haematuria) was introduced in 2015. Initially all patients with macroscopic haematuria above the age of 40 were included, but the age limit was subsequently raised to 50. In contrast to the Danish and British SCP models, which exclude patients with ‘other obvious causes’ (including acute cystitis that has not been treated), the Swedish SCP has no such clause. This has caused criticism [5], due to a high number of patients being admitted for investigation with positive urine cultures [5, 6], arguably causing the Swedish SCP to be ineffective and still failing to prove clear clinical benefit for the patients. However, a positive urine culture does not exclude the possibility of concurrent bladder cancer [7], as the prevalence of bacteriuria increases with age [8].
The aim of this study was to describe the patients admitted for urological examination in the Swedish SCP macroscopic haematuria. Furthermore, we aim to evaluate the presence of symptoms of acute cystitis in this group and its association with a diagnosis of bladder cancer. Finally, we aim to see if the inclusion criteria for SCP macroscopic haematuria could be narrowed without causing an unacceptable risk of missing bladder cancer.
Materials and methods
Helsingborg Hospital and Ängelholm Hospital are situated in southern Sweden and comprise the region of Northwestern Scania, with a population of approximately 320,000 inhabitants. According to the Swedish National Quality Register for Bladder and Urinary Tract Cancer (SNRUBC), 115 patients were diagnosed with bladder cancer in this region in 2023.
This study was designed as a retrospective observational study, by manually reviewing patient charts. All patients referred to the Department of Urology at the hospitals of Helsingborg and Ängelholm, for investigation under the terms of SCP macroscopic haematuria in 2023, were included.
At the time of the study, the Swedish SCP macroscopic haematuria included all patients above the age of 50 with macroscopic haematuria, or visible tumour on radiology or cystoscopy due to other investigations. Only patients unfit for examination were excluded.
Patient data regarding age and sex were noted. The time between referral and first examination by a urologist was noted, and a timeframe within 7 days was regarded as compliant with the terms of the SCP.
All referral notes from referring physicians were examined. The patient was regarded as having an acute cystitis when referred, if the referring physician described any of the following symptoms: a burning sensation while urinating (dysuria), an urge to urinate or an increased urinary frequency. If the symptoms were said to have lasted 3 weeks or longer it was not considered to be acute cystitis. If no timeframe was mentioned, it was assumed that the symptoms were acute. Acute cystitis was also defined as the referring physician explicitly diagnosing the patient as having an acute cystitis. Symptoms obtained by the urologist were not taken into consideration. The results from urine cultures were noted, as well as if the referring physician had prescribed an antibiotic treatment.
Cause of haematuria was noted from the patient chart at the Department of Urology, following cystoscopy and computed tomography of the urinary tract. If a cancer was diagnosed, type and grade was noted from the histopathological analysis.
The study was approved by the Swedish Ethical Review Authority (No. 2025-00380-01) and patient consent was waived by the ethics committee.
Statistical analysis
Data were summarized by descriptive statistics. Analysis was performed using SPSS. Numerical data were assessed by using the Shapiro–Wilk test to define if it followed a normal distribution. Univariate analyses were performed with the Mann–Whitney U test for comparison of unevenly distributed continuous variables, while categorical data were assessed by the Chi-squared test. Multivariate logistic regression was used for odds ratio (OR) and confidence intervals (CI) of variables comparing bladder cancer positive and bladder cancer negative patients. A p < 0.05 was regarded as statistically significant. No formal power calculation was performed before planning the analyses. Missing data were handled by leaving the corresponding fields blank and excluding them from statistical calculations.
Results
A total of 1,180 patients were referred to the Department of Urology at the Hospitals of Helsingborg and Ängelholm during 2023, under the conditions of SCP macroscopic haematuria. A total of 398 patients were excluded leaving 782 patients to remain in the study. Reasons for exclusion were as follows: 147 were duplicated referrals, 62 patients had incomplete information with essential information missing, 35 had no macroscopic haematuria, 32 patients declined participation in examination and 122 patients were referred without meeting the formal SCP criteria or had already been diagnosed with a cancer when referred for treatment. A summary of the results with baseline characteristics of the patients referred and diagnosis of bladder cancer by risk factors examined, is provided in Table 1.
| Bladder cancer versus No bladder cancer | |||||||||
| Univariate analysisa | Multivariate analysis | ||||||||
| Variable | Referred patients | Bladder cancer | No Bladder cancer | Risk ratio | 95% Confidence interval | Odds ratio | 95% confidence interval | ||
| Total (n) | 782 | 74 | 708 | ||||||
| Men (n) | 404 | 59 | 345 | ||||||
| Women (n) | 378 | 15 | 363 | ||||||
| Sex (% men) | 52 | 80 | 49 | Women 1 (Ref) | Men 3.68 | 2.13–6.37 | Women 1 (Ref) | Men 2.97 | 1.60–5.49 |
| Age (median years) | 70 | 75 | 69 | Difference in years | 6 | 3–9 | 50 years 1 (Ref) | Above 50 years 1.03b | 1.01–1.06 |
| Men (median years) | 73 | 75 | 73 | 2 | -2–6 | ||||
| Women (median years) | 65 | 75 | 65 | 10 | 7–20 | ||||
| Cystitis+ (n) | 402 | 22 | 380 | No Cystitis 1 (Ref) | Cystitis 0.40 | 0.25–0.64 | No Cystitis 1 (Ref) | Cystitis 0.54 | 0.31–0.93 |
| Men (n) | 141 | 15 | 126 | 0.64 | 0.38–1.09 | ||||
| Women (n) | 261 | 7 | 254 | 0.38 | 0.15–0.96 | ||||
| aMedian difference and Bootstrap confidence interval for age bAge as a continous variable |
|||||||||
Age and sex of the referred group
The median age of the 782 patients was 70 years with an interquartile range (IQR) 59–77. The patient population was evenly distributed between women and men, with 378 (48%) women and 404 (52%) men. The women had a median age of 65 years (IQR 57–75), and men were older (p < 0.01) 73 (IQR 63–79). The age distribution of men and women is depicted in Figure 1. Notably 58% of women referred were under the age of 70 and women between 50 and 69 made up 28% of the entire group referred for examination.
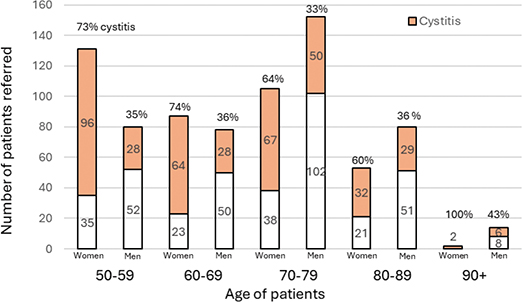
Figure 1. Number of patients referred within the Swedish Standardized Care Pathway macroscopic hematuria, Northwestern Scania 2023. Distribution by sex, age group and presence of cystitis.
Cause of haematuria
The timeframe set by the SCP was fulfilled in 96% of the time, with patients examined by a urologist within 7 days from referral. A total of 89 cases of urinary tract cancer were found, corresponding to 11% of the entire study group. Bladder cancer was the dominant diagnosis, with 74 cases, accounting for 83% of cancer cases and 9% of the entire study group. Other types of cancer, such as kidney cancer, renal pelvic cancer and ureteral cancer, were considerably less common. Kidney cancer was the second most common cancer diagnosis with a total of seven cases (<1% of the study group). The cancer-positive group was older (p < 0.01) than the whole group of examined patients, with a median age of 75 (IQR 66–82). Age was independently significant in multivariable analysis with an OR of 1.03 (CI 1.01–1.06 p< 0.01), with years above 50 as a continuous variable.
Cancer cases were more common among men than women (p < 0.01). Of the 89 diagnosed cases, 68 (76%) were found in men and 21 (24%) in women. The difference remained for bladder cancer alone, where 59 of the 74 cases (80%) were found in men and 15 cases in women (20%). The OR for bladder cancer was 2.97 (CI 1.60–5.49, p < 0.01) for men, in multivariate analysis and independently significant. Distribution of bladder cancer by age group and sex is depicted in Figure 2. The final histopathological findings are shown in Figure 3, with 12% being muscle invasive cancer, 15 % carcinoma in situ, 22% T1 and 51% Ta.

Figure 2. Number of patients diagnosed with bladder cancer within the Swedish Standardized Care Pathway macroscopic hematuria, Northwestern Scania 2023. Distribution by sex, age group and presence of cystitis.

Figure 3. Histopathological distribution of bladder cancer within the Swedish Standardized Care Pathway macroscopic hematuria, Northwestern Scania 2023.
Benign causes of haematuria are listed in Table 2. In 40% of the examined group, no clear source of haematuria could be diagnosed by the urologist. In 35% of the cases, visible cystitis could be seen.
Symptoms of acute cystitis on referral
Figure 1 also shows the distribution of patients with acute cystitis at referral for SCP macroscopic haematuria. Of the 782 patients in the study, 402 patients (51%) had acute cystitis according to the referral note. There was a difference (p < 0.01) between men and women with 261 women (69% of women) and 141 men (35% of men) presenting with symptoms of acute cystitis. The largest group with acute cystitis was women in the age group 50–59 years, with a total of 96 patients (25% of women).
Association between acute cystitis and bladder cancer
Among patients presenting with acute cystitis on referral, 22 of 402 patients (5%) had bladder cancer on urological examination. Thus, acute cystitis was associated (p < 0.01) with absence of bladder cancer, in the whole patient group on univariate analysis. However, this was only true for the age groups under 70. In the age groups 50–69, no case of bladder cancer was found among patients who presented with acute cystitis. Conversely, in the age groups above, 22 patients (30% of all patients with bladder cancer and 40% if only including patients 70 years and older) had bladder cancer and symptoms of acute cystitis (depicted in Figure 2). Seven were women (47% of women with bladder cancer) and 15 were men (26% of men with bladder cancer). Notably, four of these patients also had positive urine cultures of clinically significant bacteria, and 11 of 22 had been prescribed antibiotics by the referring physician. Four had muscle-invasive cancer. The OR for bladder cancer was 0.54 (CI 0.31–0.93, p = 0.03) in the whole group with acute cystitis on multivariate analysis, thus independently significant.
Having a positive urine culture was also associated (p < 0.01) with absence of bladder cancer. Only six patients (8%) with bladder cancer had a positive urine culture. However, 30% of patients were never cultured.
Discussion
In this retrospective observational study of 782 patients referred through the Swedish SCP macroscopic haematuria, 48% were women with a median age of 65 years. Among patients diagnosed with bladder cancer 80% were men and the median age at diagnosis was 75 years. This distribution is likely attributable to the fact that 69% of women had symptoms of acute cystitis – a criterion that would likely have excluded them from SCP referral in neighbouring countries. Among patients younger than 70 years, with concomitant symptoms of acute cystitis, the risk of bladder cancer was negligible. Conversely, in patients aged 70 years and older, 40% of those diagnosed with bladder cancer reported symptoms consistent with acute cystitis at referral.
The strength of this study lies in the fact that to our knowledge the population in Northwestern Scania is representative for a Swedish and Northern European population. We believe that compliance with the guidelines of the SCP macroscopic haematuria is rigorous among primary care physicians and that the referred group represent most patients who searched primary care for macroscopic haematuria within this region, in the age groups above 50, in 2023. The main limitation of this study is that it is retrospective. Symptoms of acute cystitis had to be interpreted retrospectively and apart from cases where the referring physicians explicitly diagnosed acute cystitis, it is unclear whether the primary care physicians interpreted the symptoms in the same way. Consequently, symptoms may have been both over- and under-interpreted as indicative of acute cystitis.
Furthermore, there are no standardized diagnostic criteria for acute cystitis. Symptoms such as dysuria, urgency and frequency are commonly used in studies [9–11], but sometimes acute cystitis is merely regarded as a clinical diagnosis. Additionally, known risk factors such as smoking, previous cancer treatment, environmental exposure and heredity are not mandatory information in the SCP. Due to limited information available, we chose not to include these variables, that could have provided further depth to the analysis.
Of 115 patients diagnosed in 2023, in Northwestern Scania, 74 patients (64%) with bladder cancer could be included in this study. This could cause the study to be underpowered, but we assume the included patients to be representative for patients within the SCP.
SCPs promote less individualized decisions and tend to resemble screening of patient groups with a certain symptom. As such, it is important that the included group of patients, to a certain extent, matches the group where a disease is likely found. Otherwise, SCPs will consume health care resources and possibly cause discomfort, or even harm, to a group of patients with little or no benefit. The inclusion criteria in the Swedish SCP macroscopic haematuria cause urologists to examine a group of patients that is younger and skewed towards women, in comparison to where urinary tract cancer is likely found. In this study, 28% of patients referred were women under 70 years of age, which is in line with a previous evaluation from a nearby region [6]. In this cohort, only one patient (<1%) was diagnosed with bladder cancer, which is lower than the expected frequency (according to SNRUBC, 7% of bladder cancer cases in Sweden are diagnosed in women younger than 70 years). Six additional women under the age of 70 had been diagnosed with bladder cancer outside the SCP or were excluded from this study, thereby accounting for this statistical discrepancy. If all seven patients had been diagnosed within the SCP, the proportion of referred women under 70 years diagnosed with bladder cancer would have been 3%.
Even though the time limit within the SCP was met in 96%, in this region, it is likely that resources drawn to examining a group of patients with low likelihood of cancer, contribute to the failure to meet the time frame and adherence to the SCP in other instances [6, 12, 13]. Furthermore, it can draw resources from examining other diagnoses, especially benign urological conditions.
In this study 11% of the examined group had a urinary tract cancer, which is slightly lower than other studies from SCPs in Sweden [6] and Denmark [14]. A study from Sweden [15] from before the SCP was introduced, showed that 24% of all patients examined by urologists for macroscopic haematuria had a urinary tract cancer, reaching 32% in asymptomatic patients. This was likely a group of patients selected by primary care physicians, and numbers in our study have been diluted by patients that primary care physicians would not choose to refer, if not prompted by the SCP. The distribution of cancer between sexes was in line with previous studies [13] as well as the scarce findings of cancers other than bladder cancer [6].
In contrast to previous studies on SCPs [5–7] that have focused on the presence of positive urine cultures, this study focuses on the presence of clinical symptoms of cystitis. Half of patients (51%) had symptoms of acute cystitis when referred and 35% had visible cystitis on cystoscopy. This was also largely skewed toward younger women with 73% of women under 70 having symptoms of acute cystitis. This group is likely excluded from examination in SCPs in other countries. To our knowledge, this is the first estimation of how many patients with macroscopic haematuria in the population have concurrent symptoms of acute cystitis.
Although both symptoms of acute cystitis and a positive urine culture were statistically significantly associated with absence of bladder cancer, 30% of all bladder cancer patients presented with haematuria and symptoms of acute cystitis. Some even had a positive urine culture. Notably, 11 of the 22 patients with symptoms of acute cystitis and bladder cancer had received antibiotic treatment from the primary care physician, indicating that they must have thought that the symptoms were due to a bacterial infection. The reason may be that bladder cancer can mimic the symptoms of cystitis. Furthermore, the elderly population is more likely to have both bacterial cystitis or bacteriuria, at the same time as bladder cancer [6, 7]. The elderly population also have a larger prevalence of lower urinary tract symptoms [16] and may have a harder time to communicate their problems, which could lead to an overestimation of acute cystitis in this age group by physicians. Hence, the exclusion criteria in the Danish and British SCPs of urinary tract infections as ‘other obvious causes’, may not be as obvious as it first seems and could cause a diagnostic delay. Women being initially misdiagnosed with cystitis may contribute to their later-stage presentation of bladder cancer and the subsequently poorer prognosis observed compared with men [17].
Nevertheless, in the age groups under 70, no patient had symptoms of acute cystitis and bladder cancer. This group consisted of 216 patients (28% of the examined group). If the Swedish SCP macroscopic haematuria excluded patients under 70 with symptoms of acute cystitis, almost one third of patients could be spared a urological and radiological examination, with a negligible (0% in this study) risk of missing urological cancer. If excluding this suggested group, in this study, the median age of the examined group would have been 72 years (IQR 13) and 61% would have been men.
In the Danish and British SCPs, microscopic haematuria is included, representing 1.5%–3% of all positive findings of urinary tract cancers [14]. This incidence has been considered too low [18] and has been excluded in the Swedish SCP, without adverse outcomes for patients [19]. Furthermore 1.4% of bladder cancer is found in the age group under 40 [20] and 2% in the age group between 40 and 49 [6], but these incidences have also been considered too low to motivate inclusion in the Swedish SCP. Thus, there are already limitations in the Swedish SCP, balancing the calculated risk of missing cancers with the resources spent on finding them.
In conclusion, the criteria of the Swedish SCP macroscopic haematuria of today skew the examined group toward younger patients consisting of more women, than where urinary tract cancer is likely found. This is largely attributed to not excluding patients with suspected urinary tract infections. However, neither symptoms of acute cystitis, nor a positive urine culture, ruled out the possibility of urinary tract cancer in the age groups 70 years and above. But, in the age groups under 70, this was clearly the case. Thus, treating patients under the age of 70 with symptoms of acute cystitis before referral is considered, would lead to a substantial reduction in the number of patients examined with a minimal risk of missing cancer. This could be taken into consideration when updating the SCP both in Sweden and neighbouring countries. Prospective studies including more risk factors would add further knowledge.
References
- [1] Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. https://doi.org/10.3322/caac.21492
- [2] Malmström PU, Gårdmark T, Sherif A, Strock V, et al. Incidence, survival and mortality trends of bladder cancer in Sweden 1997–2016. Scand J Urol. 2019;53(4):193–9. https://doi.org/10.1080/21681805.2019.1632380
- [3] Shapley M, Mansell G, Jordan JL, et al. Positive predictive values of >/=5% in primary care for cancer: systematic review. Br J Gen Pract. 2010;60(578):e366–77. https://doi.org/10.3399/bjgp10X515412
- [4] Malmström PU, Skaaheim Haug E, Boström PJ, et al. Progress towards a Nordic standard for the investigation of hematuria: 2019. Scand J Urol. 2019;53(1):1–6. https://doi.org/10.1080/21681805.2018.1555187
- [5] Holmäng S, Hedelin H. Standardized care pathway for bladder cancer in Sweden. So far lots of pain but little gain. Scand J Urol. 2022;56(3):233–4. https://doi.org/10.1080/21681805.2022.2078876
- [6] Nilbert M, Bläckberg M, Ceberg J, et al. Diagnostic pathway efficacy for urinary tract cancer: population-based outcome of standardized evaluation for macroscopic haematuria. Scand J Urol. 2018;52(4):237–43. https://doi.org/10.1080/21681805.2018.1498124
- [7] Vasdev N, Thorpe AC. Should the presence of a culture positive urinary tract infection exclude patients from rapid evaluation hematuria protocols? Urol Oncol. 2013;31(6):909–13. https://doi.org/10.1016/j.urolonc.2011.07.016
- [8] Luu T, Albarillo FS. Asymptomatic bacteriuria: prevalence, diagnosis, management, and current antimicrobial stewardship implementations. Am J Med. 2022;135(8):e236–44. https://doi.org/10.1016/j.amjmed.2022.03.015
- [9] Bollestad M, Vik I, Grude N, et al. Bacteriology in uncomplicated urinary tract infections in Norwegian general practice from 2001–2015. BJGP Open. 2018;1(4):bjgpopen17X101145. https://doi.org/10.3399/bjgpopen17X101145
- [10] Hooton TM, Vecchio M, Iroz A, et al. Effect of increased daily water intake in premenopausal women with recurrent urinary tract infections: a randomized clinical trial. JAMA Intern Med. 2018;178(11):1509–15. https://doi.org/10.1001/jamainternmed.2018.4204
- [11] Vik I, Bollestad M, Grude N, et al. Ibuprofen versus pivmecillinam for uncomplicated urinary tract infection in women-A double-blind, randomized non-inferiority trial. PLoS Med. 2018;15(5):e1002569. https://doi.org/10.1371/journal.pmed.1002569
- [12] Abuhasanein S, Jahnson S, Kjölhede H. Shortened time to diagnosis for patients suspected of urinary bladder cancer managed in a standardized care pathway was associated with an improvement in tumour characteristics. BJUI Compass. 2024;5(2):261–8. https://doi.org/10.1002/bco2.301
- [13] Abuhasanein S, Jahnson S, Aljabery F, et al. Standardized care pathways for patients with suspected urinary bladder cancer: the Swedish experience. Scand J Urol. 2022;56(3):227–32. https://doi.org/10.1080/21681805.2022.2058605
- [14] Elmussareh M, Young M, Ordell Sundelin M, et al. Outcomes of haematuria referrals: two-year data from a single large university hospital in Denmark. Scand J Urol. 2017;51(4):282–9. https://doi.org/10.1080/21681805.2017.1310759
- [15] Boman H, Hedelin H, Holmäng S. The results of routine evaluation of adult patients with haematuria analysed according to referral form information with 2-year follow-up. Scand J Urol Nephrol. 2001;35(6):497–501. https://doi.org/10.1080/003655901753367613
- [16] Irwin DE, Milsom I, Hunskaar S, et al. Population-based survey of urinary incontinence, overactive bladder, and other lower urinary tract symptoms in five countries: results of the EPIC study. Eur Urol. 2006;50(6):1306–14; discussion 14–5. https://doi.org/10.1016/j.eururo.2006.09.019
- [17] Secher MS, Hyldgaard J, Jensen JB. The association between gender, stage and prognosis in bladder cancer patients undergoing radical cystectomy. Scand J Urol. 2023;57(1–6):10–4. https://doi.org/10.1080/21681805.2023.2166103
- [18] Malmström PU. Time to abandon testing for microscopic haematuria in adults? BMJ. 2003;326(7393):813–5. https://doi.org/10.1136/bmj.326.7393.813
- [19] Malmström PU, Truls G. Abandoning testing for asymptomatic microscopic haematuria in Sweden – a long-term follow-up. Scand J Urol. 2023;58:109–14. https://doi.org/10.2340/sju.v58.11142
- [20] Lara J, Brunson A, Keegan TH, et al. Determinants of survival for adolescents and young adults with urothelial bladder cancer: results from the California Cancer Registry. J Urol. 2016;196(5):1378–82. https://doi.org/10.1016/j.juro.2016.05.082