ORIGINAL RESEARCH ARTICLE
Association between human papillomavirus status and the accuracy of [18F]-FDG PET/CT for detecting inguinal metastasis in penile cancer
Ida Marie Nordangera,b  , Torjan Magne Haslerudc,d, Alfred Honoréa,b , Tor Kristian Thorkelsena , Patrick Juliebø-Jonesa,b , Daniela Elena Costeab,e , Ellen Bergete , Christian Beislanda,b and Christian Arvei Moena,b
, Torjan Magne Haslerudc,d, Alfred Honoréa,b , Tor Kristian Thorkelsena , Patrick Juliebø-Jonesa,b , Daniela Elena Costeab,e , Ellen Bergete , Christian Beislanda,b and Christian Arvei Moena,b
aDepartment of Urology, Haukeland University Hospital, Bergen, Norway; bDepartment. of Clinical Medicine, University of Bergen, Bergen, Norway; cDepartment of Radiology, NM/PET-Centre, Haukeland University Hospital, Bergen, Norway; dDepartment of Radiology, NM/PET-Centre, Stavanger University Hospital, Stavanger, Norway; eDepartment of Pathology, Haukeland University Hospital, Bergen, Norway
ABSTRACT
Objectives: [18F]-FDG positron emission tomography combined with computed tomography (PET/CT) allows the non-invasive assessment of inguinal lymph node (ILN) status in penile squamous cell carcinoma (PSCC). The aim of this study was to assess if the diagnostic accuracy of PET/CT was influenced by the human papillomavirus (HPV) status of the tumor.
Methods: This retrospective study included 81 treatment-naïve patients with PSCC who underwent surgery between 2010 and 2024 and had a PET/CT before ILN surgery. Inguinal results were compared with histopathology (n = 72) or follow-up findings (n = 9), stratified by HPV status.
Results: HPV DNA was detected in tumor tissue from 41 (51%) patients. The sensitivity and specificity of PET/CT to detect an ILN metastasis were 83% (69%–93%) and 68% (58%–76%), with no significant differences when stratified by HPV status (both P > 0.8). In multivariable logistic regression, after adjustment for the clinical nodal stage, the timing of PET/CT (before or after penile surgery), number of FDG-positive ILNs, the maximum standardized uptake value (SUVmax) of the ILNs and HPV status, SUVmax remained associated with ILN metastasis (OR 1.18, 95% CI: (1.05–1.38), P = 0.023). There was, however, no significant interaction between HPV status and SUVmax (P = 0.57).
Conclusions: The diagnostic accuracy of [18F]-FDG PET/CT regarding preoperative detection of ILN metastasis was not associated with the HPV status in penile cancer. These findings indicate that HPV status does not need to be considered when interpreting the inguinal findings of preoperative PET/CT scans.
KEYWORDS: diagnostic accuracy; 18F-FDG PET/CT; human papillomavirus; lymph node metastasis; penile cancer; staging
Citation: Scandinavian Journal of Urology 2025, VOL. 60, 229–234. https://doi.org/10.2340/sju.v60.45027.
Copyright: © 2025 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 7 May 2025; Accepted: 23 October 2025; Published: 16 December 2025
CONTACT: Ida Marie Nordanger ida.marie.nordanger@helse-bergen.no Department of Urology, Haukeland University Hospital, Bergen 5021, Norway
Supplemental data for this article can be accessed online at https://doi.org/10.2340/sju.v60.45027
Introduction
Penile squamous cell carcinoma (PSCC) is known to develop from either infection with human papillomavirus (HPV) or from chronic inflammation [1]. Thus, PSCC is classified as HPV-related or non-HPV-related by the World Health Organization (WHO) [2].
The prognosis of PSCC is mainly dependent on whether inguinal lymph node (ILN) metastases are present at the time of treatment [1, 3, 4]. Surgical staging to determine possible inguinal node-positive disease, however, carries a high level of morbidity [5, 6]. An accurate non-invasive examination for detection of inguinal metastases would therefore be of great value in the diagnostic work-up and treatment of penile cancer.
[18F]-fluoro-2-deoxy-D-glucose positron emission tomography combined with computed tomography ([18F] -FDG positron emission tomography combined with computed tomography (PET/CT), hereafter abbreviated to PET/CT) is an imaging modality that allows a non-invasive staging of regional lymph nodes [7]. Use of PET/CT for detecting inguinal metastases has, nevertheless, been limited by the reduced sensitivity and specificity reported in multiple studies [8–10]. None of these studies, however, have investigated if the sensitivity and specificity of PET/CT depend on the HPV status of the tumor. This is important to address, as HPV status is also a prognostic factor, with HPV positivity being associated with better cancer-specific survival in patients with PSCC [11]. To this end, the FDG-uptake in regional lymph nodes may be influenced by factors such as the degree of cancer-associated inflammation and the size and number of lymph node metastases, which might be different in HPV-positive compared to HPV-negative PSCC.
This study investigated if the diagnostic accuracy (sensitivity, specificity, positive predictive value [PPV] and negative predictive value [NPV]) of PET/CT to detect ILN metastasis in penile cancer was different for patients with HPV DNA positive compared to HPV DNA negative tumors.
Materials and methods
Following approval from the regional ethics committee (REK vest project no.291376), all treatment-naïve patients who underwent surgery for PSCC at Haukeland University Hospital between 2010 and 2024 were retrospectively identified. A total of 82 out of 132 patients had both a preoperative PET/CT scan as well as an established ILN status based on histopathological findings or long-term follow up (more than 5 years without inguinal metastasis). All but one of these patients accepted inclusion into this study, making the final study population 81 patients (Figure 1).
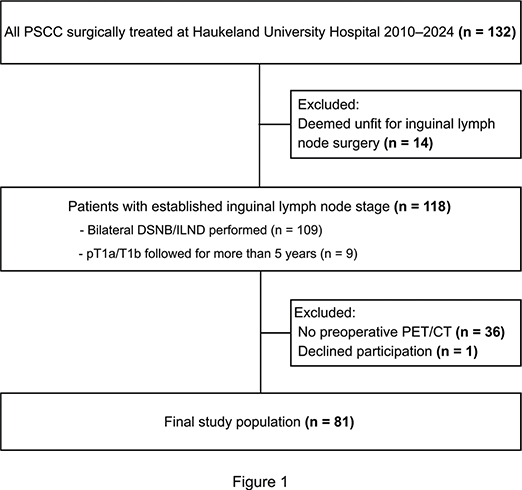
Figure 1. Flow diagram of the patient selection with inclusion and exclusion criteria. DSNB: Dynamic sentinel node biopsy; ILND: Inguinal lymph node dissection; PET/CT: positron emission tomography combined with computed tomography; PSCC: Penile squamous cell carcinoma.
For all patients, details regarding clinical variables and the type of treatment offered were noted from the medical records. Stored tissue blocks and slides had already been retrieved from the archives and analyzed as part of previous studies [12, 13]. Specifically, the histopathological slides were re-examined and the primary tumor restaged by an experienced genitourinary pathologist according to the current eighth Tumor, Node, Metastasis (TNM) classification system [14]. This restaging included assessment of tumor stage (pT), grade of differentiation (grade) and presence of lymphovascular infiltration (LVI).
Tumor tissue samples from the stored tissue blocks were also used for HPV DNA analysis, performed using a standard, commercially available assay on the same equipment routinely used in clinical practice. This included polymerase chain reaction (PCR) amplification of virus DNA, detection of virus DNA in agarose gel and Sanger sequencing of HPV-positive samples to identify specific HPV types. The GP5+/GP6+ primer system (Applied Biosystems, Waltham, Massachusetts, USA) for the detection of the HPV L1 gene was used [12]. To ensure assay validity, internal controls were included in all analyses. For each tissue sample, two separate aliquots were tested alongside a known positive HPV16 control, a negative ‘section control’ (DNA from an HPV-negative sample to rule out contamination during sectioning of tissue blocks) and a water control (to exclude contamination during PCR setup).
During the study period, all patients with PSCC were eligible for a preoperative PET/CT. In practice, some patients underwent a conventional CT at their local hospital to reduce travel distance, or when limited PET/CT availability could have delayed timely surgery (Figure 1). Patients undergoing PET/CT were scanned using Siemens Biograph Vision. The procedure was performed with a whole-body PET from the skull to the mid-thigh and a co-registered contrast enhanced diagnostic CT. After 6 h of fasting, patients were injected intravenously with 3 MBq/kg of fluorodeoxyglucose ([18F] FDG). The PET/CT scan was performed 60 min after contrast injection. A focal lesion with increased uptake of FDG was reported with a maximal standard uptake value (SUVmax). A lymph node was typically considered to contain metastatic tissue (positive node) on PET/CT if it demonstrated a SUVmax above 6–7 (approximately twice the SUVmax of normal liver tissue) in combination with suspicious morphological features, including a rounded shape, enlarged lymph node, absence of a visible nodal hilus and/or an asymmetric appearance compared with other visible inguinal nodes. The final assessment, however, was based on an integrated evaluation of these features rather than a single criterion. The PET/CT reports were retrospectively registered independently by two authors (IMN and CAM) to confirm the data accuracy. In a small number of cases with ambiguous findings, the researchers held consensus discussions to reach a final interpretation.
For each groin, the PET/CT findings were compared against the ILN status. Throughout the study period, patients fit for surgery having clinically node-negative (cN0) groins were scheduled for diagnostic sentinel node biopsy (DSNB) while clinically node-positive (cN+) groins were scheduled for DSNB and/or inguinal lymph node dissection (ILND). The only exceptions to this rule were four patients with T1a disease, which is classified by the EAU guidelines as a low-risk tumor where the risk of metastasis is too low to justify surgical staging [4]. These patients did therefore not undergo DSNB/ILND but were followed by active surveillance. An additional five patients with T1b disease who had negative preoperative PET/CT scans and had been followed for more than 5 years without regional lymph node pathology detected, were also included. PET/CT results for the pelvic area were also registered, but only those PET/CT findings that could be coupled to histopathology from pelvic lymph node dissection (PLND) were compared.
Statistical analysis
Categorical variables were described with frequencies and percentages, and quantitative variables with median and interquartile range (IQR). The Fisher’s exact test was used to compare the accuracy of the inguinal PET/CT findings when stratified by HPV status.
An exploratory uni- and multivariable logistic regression was performed to investigate the potential of PET/CT variables (number of FDG-positive inguinal nodes, SUVmax) to determine if a patient had lymph node metastasis, adjusted for by the HPV status and the clinical inguinal node status (cN stage). Since these variables could be influenced by the timing of the PET/CT (before or after penile surgery), this variable was also included in the model. To further investigate if the HPV status modified the predictive value of the SUVmax, an additional model including an interaction term between HPV status and SUVmax was also investigated [15].
For SUVmax alone, the Youden’s index was calculated to investigate which value optimized the tradeoff between sensitivity and specificity of the PET/CT results regarding ILN metastasis.
For all analyses, a p value less than 0.05 was considered statistically significant. Statistical analyses were performed using software R version 4.3.3 [16].
Results
HPV types and cohort characteristics
HPV DNA was present in cancer tissue from 41 (51%) of the 81 patients. The types detected are shown in Supplementary Table 1. Multiple HPV types in tumor tissue did not occur, and all types detected are classified as high-risk (hrHPV).
The median age of all patients was 69 years (IQR 57–74), and clinically node-positive inguinal groins were present in 48% of cases (Table 1). Additional variables regarding age group distribution, the presence of phimosis/balanitis, types of penile, inguinal and pelvic surgeries as well as follow-up time after surgery can be found in Supplementary Table 2.
| Characteristic | Overall N = 811 | HPV negative N = 401 | HPV positive N = 411 |
| Age at surgery | 69 (57, 74) | 68 (55, 74) | 71 (61, 74) |
| cN-stage | |||
| cN0 | 42 (52%) | 20 (50%) | 22 (54%) |
| cN+ | 39 (48%) | 20 (50%) | 19 (46%) |
| Timing of PET/CT | |||
| Before penile surgery | 61 (75%) | 31 (78%) | 30 (73%) |
| After penile surgery | 20 (25%) | 9 (23%) | 11 (27%) |
| Highest inguinal SUVmax | 4.0 (0.0, 8.0) | 3.0 (0.0, 7.1) | 5.7 (0.0, 10.0) |
| PET/CT inguinal result | |||
| Negative | 30 (37%) | 17 (43%) | 13 (32%) |
| Positive | 51 (63%) | 23 (58%) | 28 (68%) |
| Nodal status | |||
| pN0 | 51 (63%) | 28 (70%) | 23 (56%) |
| pN+ | 30 (37%) | 12 (30%) | 18 (44%) |
| cN-stage: clinical node stage; HPV: Human papillomavirus; PET/CT: positron emission tomography combined with computed tomography; pT: Pathological T-stage; SUVmax: maximal standard uptake value; 1Median (IQR); n (%). | |||
PET/CT findings and histopathology stratified by HPV status
In 75% of cases, the PET/CT was performed before penile surgery and in 25% after removal of the primary tumor (Table 1). Moreover, for the patients who underwent invasive inguinal staging, the median time from PET/CT to inguinal surgery was 0 (0–1) months. The median SUVmax was 4.0 (0.0–8.0) and ILN metastasis was suspected in approximately 63% of the PET/CT examinations. A breakdown of the findings per inguinal groin and pelvic region can be found in Supplementary Table 3.
Pathological inguinal node-positive disease was found in 30 (37%) patients (Table 1). Details regarding the distribution of pT stages, grade, LVI, pN stages and number of metastatic nodes, stratified by HPV status, can be found in Supplementary Table 4.
Diagnostic accuracy of PET/CT
For all groins combined, PET/CT showed a sensitivity of 83% (69%–93%), specificity of 68% (58%–76%), PPV of 47% (36%–59%) and NPV of 92% (84%–97%) (Error! Hyperlink reference not valid.). There were no significant differences when stratified by HPV status (all P > 0.2). Data on the number of PET/CT examinations with agreement/disagreement against histopathology/follow-up for each inguinal and pelvic area can be found in Supplementary Tables 5 and 6, respectively.
Detection of metastatic tissue in an ILN after a negative preoperative PET/CT (false negative examination) occurred in seven groins. For these cases, the size of the metastatic tissue ranged from 1.1 to 13 mm.
Predictors of inguinal lymph node metastasis based on PET/CT findings and HPV status
In multivariable regression, after adjusting for HPV status, cN stage and other PET/CT variables, SUVmax remained associated with an ILN metastasis (OR 1.18, 95% confidence interval (1.05, 1.38), P = 0.023) (Table 3). There was, however, no significant interaction between HPV status and SUVmax (P = 0.57). When investigated, the optimal value for correct classification of cases was a SUVmax value of 6.1. This resulted in an accuracy (proportion of correct classified cases) of 86%.
| Characteristic | Overall | HPV negative | HPV positive | p-value1 |
| All patients | ||||
| No. pts/groins | 81/162 | 40/80 | 41/82 | |
| Sensitivity | 83 (69–93) | 82 (56–95) | 84 (63–95) | 1 |
| Specificity | 68 (58–76) | 67 (54–78) | 68 (55–80) | 0.85 |
| PPV | 47 (36–59) | 40 (24–58) | 54 (37–70) | 0.25 |
| NPV | 92 (84–97) | 93 (81–97) | 91 (77–97) | 0.71 |
| HPV: Human papillomavirus; NPV: Negative predictive value; PPV: Positive predictive value. 1Fisher’s exact test. Values are given as percentages with corresponding 95% confidence intervals. | ||||
Discussion
The main finding of the current study is that the diagnostic accuracy of [18F]-FDG PET/CT was not influenced by HPV status regarding the detection of ILN metastasis in penile cancer.
There are two major issues that affect the diagnostic accuracy of PET/CT. First, micrometastatic disease may not be detected, resulting in a false negative examination and thus a lower sensitivity. Second, FDG-positive nodes due to inflammation may be mistaken for metastatic activity, resulting in a false positive examination and thus a lower specificity.
Regarding sensitivity, as many as 20%–25% of cN0 groins may contain occult metastases where the size of tumor deposits is too small to be palpated [4]. To this end, several studies have shown poor diagnostic accuracy of PET/CT, especially in the case of cN0 groins [17, 18]. Moreover, it has previously been shown that PET/CT cannot reliably detect inguinal metastases from PSCC that are less than about 10 mm in size [19]. Therefore, PET/CT has not been recommended as part of a standard preoperative diagnostic work-up in cN0 PSCC [7, 8]. The findings of the current study are in agreement with these conclusions. Furthermore, the added value of this study is the finding that these recommendations do not need to be modified based on the HPV status of the penile tumor.
Regarding specificity, reactive lymph nodes due to inflammation are common in PSCC, and can be present in up to 40% of cN+ groins [20]. Moreover, the timing of the PET/CT has also been called into question. If performed after penile surgery, the postoperative inflammation could result in an increased number of false positive examinations [21]. In this study, there was no indication that timing of the PET/CT (before or after penile surgery) impacted the diagnostic accuracy regarding the detection of an ILN metastasis.
Increasing SUVmax, however, was associated with a patient having an ILN metastasis, with a value around 6 found to most accurately classify cases. This is in keeping with another study that found a SUVmax of 6.5 to best predict cancer-specific survival [22]. In a study by Jakobsen et al. [9], however, the accuracy of PET/CT was investigated at different SUVmax values from 2 to 6. While a SUVmax value of 6 yielded the best sensitivity, the specificity was better when using a lower SUVmax cutoff value. Therefore, caution should be exerted in placing too much emphasis on a specific SUVmax value alone. The SUVmax value, however, was not modified by the HPV status of the tumor and the same interpretation of the results can therefore be used across all cases.
Few studies report results regarding the diagnostic accuracy of PET/CT for diagnosing pelvic metastasis [21]. However, a retrospective study by Ottenhof et al. found that PET/CT did have a high diagnostic value for pelvic staging in patients with high-risk penile cancer [23]. While the study did not include data on HPV, false negative PET/CT scans were in general rarely reported. This is in contrast to the findings of the current study, where almost 1 in 4 of the included pelvic scans were false negative, but these results are limited by the few cases reported. As such, this study cannot assess the diagnostic value of PET/CT for pelvic lymph nodes.
Traditionally, PLND has been an open procedure associated with a high risk of complications. Older, more frail patients have therefore often received other oncological treatments instead. Currently, however, PLND can be performed robotically with less associated morbidity. Histopathology from pelvic specimens is therefore more readily available today. The value of PET/CT to non-invasively diagnose pelvic metastasis should therefore be examined further in future studies.
Whether HPV status affects the number of metastatic ILNs in PSCC has not been fully resolved. In a study by Bandini et al., patients with HPV positive PSCC did have a lower ILN metastasis density compared to patients with HPV negative disease [24]. Other studies, however, have not found a difference in the distribution of node-positive disease when stratified by HPV status [25–27]. This should therefore also be further examined in future studies, including results for the pelvic area.
The major limitations of this study are its retrospective design and relatively small cohort size. As this was a retrospective exploratory study, no formal a priori power analysis was conducted to justify the sample size. Instead, the cohort size was determined by the available patient data. The findings should therefore be interpreted with caution, and future studies with larger sample sizes are warranted to confirm these results. The study is, however, strengthened by the completeness of the clinical and histopathological data and that the groups were balanced regarding HPV status.
All PET/CT examinations were performed according to contemporary clinical standards. As the study period spans a relatively long timeframe, it is possible that factors such as a learning curve in the early years and hardware upgrades over time may have influenced the results.
The researchers who interpreted the PET/CT reports were not blinded to clinical or histopathological outcomes, which represents a potential source of bias. However, PET/CT readings were completed independently, and only later were the results compared with histopathology. No changes were made to the PET/CT data based on this comparison.
SUVmax of the penile tumor was not studied, since about one in four of the PET/CT scans were performed after removal of the penile tumor. This study has only addressed the diagnostic accuracy of a preoperative PET/CT in treatment-naïve patients. The role of HPV status in the use of PET/CT for evaluation after neoadjuvant treatment or for follow-up of PSCC patients after initial treatment should therefore be examined further in future studies.
Conclusions
The diagnostic accuracy of [18F]-FDG PET/CT for preoperative detection of ILN metastasis was not associated to the HPV status of the tumor. The findings indicate that interpretations of preoperative PET/CT scans regarding the detection of inguinal metastasis do not need to be modified based on the HPV status of the penile tumor.
Grants/acknowledgements
Financial support related to the HPV analyses performed on archival tissue was obtained from the Norwegian Institute of Urology. There are no conflicts of interest to declare, and the above-mentioned institution played no part in the development or the approval of this manuscript.
References
- [1] Thomas A, Necchi A, Muneer A, et al. Penile cancer. Nat Rev Dis Primers. 2021;7:11. https://doi.org/10.1038/s41572-021-00246-5
- [2] Cubilla AL, Velazquez EF, Amin MB, et al. The World Health Organisation 2016 classification of penile carcinomas: a review and update from the International Society of Urological Pathology expert-driven recommendations. Histopathology. 2018;72:893–904. https://doi.org/10.1111/his.13429
- [3] Sachdeva A, McGuinness L, Zapala L, et al. Management of lymph node-positive penile cancer: a systematic review. Eur Urol. 2024;85:257–73. https://doi.org/10.1016/j.eururo.2023.04.018
- [4] Brouwer OR, Albersen M, Parnham A, et al. European Association of Urology–American Society of Clinical Oncology Collaborative Guideline on Penile Cancer: 2023 Update. Eur Urol. 2023;83:548–60. https://doi.org/10.1016/j.eururo.2023.02.027
- [5] Gopman JM, Djajadiningrat RS, Baumgarten AS, et al. Predicting postoperative complications of inguinal lymph node dissection for penile cancer in an international multicentre cohort. BJU Int. 2015;116:196–201. https://doi.org/10.1111/bju.13009
- [6] Wever L, de Vries HM, Dell’Oglio P, et al. Incidence and risk factor analysis of complications after sentinel node biopsy for penile cancer. BJU Int. 2022;130:486–95. https://doi.org/10.1111/bju.15725
- [7] Ottenhof SR, Vegt E. The role of PET/CT imaging in penile cancer. Transl Androl Urol. 2017;6:833–8. https://doi.org/10.21037/tau.2017.04.36
- [8] Sadeghi R, Gholami H, Zakavi SR, et al. Accuracy of 18F-FDG PET/CT for diagnosing inguinal lymph node involvement in penile squamous cell carcinoma: systematic review and meta-analysis of the literature. Clin Nucl Med. 2012;37:436–41. https://doi.org/10.1097/RLU.0b013e318238f6ea
- [9] Jakobsen JK, Frahm Nielsen T, Ipsen P, et al. DaPeCa-7: comparative assessment of fluorodeoxyglucose positron emission tomography/computed tomography (CT) and conventional diagnostic CT in diagnosis of lymph node metastases, distant metastases and incidental findings in patients with invasive penile cancer. BJU Int. 2021;127:254–62. https://doi.org/10.1111/bju.15206
- [10] Lee SW, Kim SJ. Diagnostic performance of 18F-FDG PET/CT for lymph node staging in penile cancer. Clin Nucl Med. 2022;47:402–8. https://doi.org/10.1097/RLU.0000000000004081
- [11] Vandermaesen K, Elst L, Defraigne C, et al. The prognostic role of HPV status in penile squamous cell carcinoma: a systematic review and meta-analysis. Int J Impot Res. 2025;37:782–93. https://doi.org/10.1038/s41443-025-01145-z
- [12] Moen CA, Falkenthal TE, Thorkelsen TK, et al. Penile cancers attributed to human papillomavirus are associated with improved survival for node-positive patients. Findings from a Norwegian Cohort Study Spanning 50 years. Eur Urol Oncol. 2024;7:778–85. https://doi.org/10.1016/j.euo.2023.10.013
- [13] Nordanger IM, Beisland C, Thorkelsen TK, et al. The prognostic value of human papillomavirus status in penile cancer: outcomes from a Norwegian cohort study. Clin Genitourin Cancer. 2024;22:102127. https://doi.org/10.1016/j.clgc.2024.102127
- [14] Brierley J, Gospodarowicz MK, Wittekind C. TNM classification of malignant tumours. Chichester, UK: Wiley; 2017.
- [15] Amy Berrington de G, Cox DR. Interpretation of interaction: a review. Ann Appl Stat. 2007;1:371–85. https://doi.org/10.1214/07-AOAS124
- [16] R Core Team_. R: A language and environment for statistical computing [Internet]. Austria: R Foundation for Statistical Computing V; 2024. Available from: https://www.R-project.org/ [Cited date October 17, 2025]
- [17] Leijte JA, Graafland NM, Valdes Olmos RA, et al. Prospective evaluation of hybrid 18F-fluorodeoxyglucose positron emission tomography/computed tomography in staging clinically node-negative patients with penile carcinoma. BJU Int. 2009;104:640–4. https://doi.org/10.1111/j.1464-410X.2009.08450.x
- [18] Souillac I, Rigaud J, Ansquer C, et al. Prospective evaluation of (18)F- fluorodeoxyglucose positron emission tomography-computerized tomography to assess inguinal lymph node status in invasive squamous cell carcinoma of the penis. J Urol. 2012;187:493–7. https://doi.org/10.1016/j.juro.2011.10.033
- [19] Schlenker B, Scher B, Tiling R, et al. Detection of inguinal lymph node involvement in penile squamous cell carcinoma by 18F-fluorodeoxyglucose PET/CT: a prospective single- center study. Urol Oncol. 2012;30:55–9. https://doi.org/10.1016/j.juro.2011.10.033
- [20] Hughes B, Leijte J, Shabbir M, et al. Non-invasive and minimally invasive staging of regional lymph nodes in penile cancer. World J Urol. 2009;27:197–203. https://doi.org/10.1007/s00345-008-0288-6
- [21] Mirvald C, Garaz R, Sinescu I, et al. Current role of PET CT in staging and management of penile cancers. J. Clin. Med. 2024, 13(16), 4879. https://doi.org/10.20944/preprints202407.0356.v1
- [22] Salazar A, Junior EP, Salles PGO, et al. (18)F-FDG PET/CT as a prognostic factor in penile cancer. Eur J Nucl Med Mol Imaging. 2019;46:855–63. https://doi.org/10.1007/s00259-018-4128-7
- [23] Ottenhof SR, Djajadiningrat RS, Versleijen MWJ, et al. F-18 fluorodeoxyglucose positron emission tomography with computed tomography has high diagnostic value for pelvic and distant staging in patients with high-risk penile carcinoma. Eur Urol Focus. 2022;8:98–104. https://doi.org/10.1016/j.euf.2021.02.012
- [24] Bandini M, Ross JS, Zhu Y, et al. Association between human papillomavirus infection and outcome of perioperative nodal radiotherapy for penile carcinoma. Eur Urol Oncol. 2021;4:802–10. https://doi.org/10.1016/j.euo.2020.10.011
- [25] Bezerra SM, Chaux A, Ball MW, et al. Human papillomavirus infection and immunohistochemical p16(INK4a) expression as predictors of outcome in penile squamous cell carcinomas. Hum Pathol. 2015;46:532–40. https://doi.org/10.1016/j.humpath.2014.12.004
- [26] Djajadiningrat RS, Jordanova ES, Kroon BK, et al. Human papillomavirus prevalence in invasive penile cancer and association with clinical outcome. J Urol. 2015;193:526–31. https://doi.org/10.1016/j.juro.2014.08.087
- [27] Hu J, Cui Y, Liu P, et al. Predictors of inguinal lymph node metastasis in penile cancer patients: a meta-analysis of retrospective studies. Cancer Manag Res. 2019;11:6425–41. https://doi.org/10.2147/CMAR.S206579