ORIGINAL RESEARCH ARTICLE
Long-term oncological outcomes of pelvic lymph node dissection during radical prostatectomy
Rikke Groth Olsena,b,c  , William Birk Richa,b, Klaus Brassoa,b,d , Andreas Rødera,b,d , Lars Kongeb,c , Flemming Bjerrumc,e and Hein Vincent Stroomberga,f
, William Birk Richa,b, Klaus Brassoa,b,d , Andreas Rødera,b,d , Lars Kongeb,c , Flemming Bjerrumc,e and Hein Vincent Stroomberga,f
aCopenhagen Prostate Cancer Center, Department of Urology, Copenhagen University Hospital – Rigshospitalet, Copenhagen, Denmark; bFaculty of Health and Medical Sciences, University of Copenhagen, Denmark; cCopenhagen Academy for Medical Education and Simulation (CAMES), Copenhagen University Hospital, Rigshospitalet, Denmark; dDepartment of Urology, Copenhagen University Hospital, Rigshospitalet, Denmark; eDepartment of Gastrointestinal and Hepatic Diseases, Amager and Hvidovre Hospital, Hvidovre, Denmark; fSection of Biostatistics, Department of Public Health, University of Copenhagen, Copenhagen, Denmark
ABSTRACT
Purpose: Lymph node dissection during radical prostatectomy (RP) remains under debate due to an unclear impact on oncological outcomes. Here, we investigate long-term oncological events after RP +/- pelvic lymph node dissection (PLND).
Methods: All patients who had an RP from 2006 to 2021 (N=15,515) in the Danish Prostate Registry were included. Cumulative incidence of biochemical failure (BF), subsequent treatment, and prostate cancer-specific death by the Aalen Johansen estimator from the time of RP were compared for men without lymph nodes removed (pNx), without positive lymph nodes (pN0), and with lymph node invasion (pN1). Area under the curve (AUC) of the receiver operating characteristic was used to determine the added value of PLND for outcome discrimination.
Results: The 15-year incidences of BF were pNx = 22% (95% confidence interval [95CI]: 20–23), pN0 = 37% (95CI: 35–39), and pN1 = 70% (95CI: 65–76). Fifteen-year incidences of subsequent treatment were 19% (95CI: 18–20), 31% (95CI: 29–33), and 84% (95CI: 79–89) for men with pNx, pN0, and pN1. Fifteen-year risk of prostate cancer-specific death was 2.1% (95CI: 1.6–2.6), 5.5% (95CI: 4.6–6.5), and 25% (95CI: 18–32) for men with pNx, pN0, and pN1. The AUC for the 10-year BF increased from 74% (95CI: 72–77) to 76% (95CI: 73–78) with the addition of pN0/pN1 in the model. The main limitation was the inability to differentiate the number of malignant nodes removed.
Conclusion: Men with positive lymph nodes after PLND faced a high risk of BF, subsequent treatment, and prostate cancer-specific death. As the addition of PLND did not substantially improve the discriminative ability, the added benefit of PLND is likely limited. The side effects of PLND should be considered in relation to its possible advantages.
KEYWORDS: Urology; radical prostatectomy; prostate cancer; lymph node dissection; patient outcome; DanProst
Citation: Scandinavian Journal of Urology 2026, VOL. 61, 1–6. https://doi.org/10.2340/sju.v60.45236.
Copyright: © 2026 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 14 January 2025; Accepted: 25 August 2025; Published: 7 January 2026
CONTACT: Rikke Groth Olsen rikke.groth.olsen.01@regionh.dk Copenhagen Prostate Cancer Center, Ole Malløes Vej 24, 2200 Copenhagen N, Denmark
Supplemental data for this article can be accessed online at https://doi.org/10.2340/sju.v61.45236
Competing interests and funding: The authors have no conflicts of interest to report related to the presented manuscript.
No project-specific funding was obtained.
Introduction
Pelvic lymph node dissection (PLND) during radical prostatectomy (RP) was initially performed as a staging procedure limited to the obturator fossa, with the node-positive disease being considered an adverse pathological finding [1]. This indicated the need for androgen deprivation therapy, as demonstrated in the Messing trial in 1999 [2]. The trial was criticised for its limited dissection, low accrual, and power, which could lead to undertreatment due to the limited PLND. In contrast, adjuvant therapy would be an overtreatment when PLND alone would lead to a cure. Later studies showed that extended PLND could find more patients with positive lymph nodes, albeit with the risk of more complications [1, 3, 4]. As a result, extended PLND has become the standard for PLND. However, the benefit of extended PLND in terms of oncological outcomes has been harder to show, and the literature lacks evidence of the long-term outcomes of PLND beyond biochemical failure (BF) [1, 5, 6]. Here, we use nationwide prospectively maintained registries to describe the long-term risk of BF, secondary therapies, and disease-specific mortality following RP with or without PLND. The aim is to discuss the long-term oncological outcomes of PLND in RP.
Patients and methods
We extracted data from the prospectively maintained Danish Prostate Registry (DanProst) on all men who underwent RP from January 1, 2006 to December 31, 2021, without any other prostate cancer-related treatment up to 31 days after surgery [7]. All Danish patients who underwent RP within the study period are included in the registry, and the registry has shown excellent completeness and veracity [8, 9]. The period was chosen to adhere to updated ISUP guidelines, and national guidelines recommending that extended PLND be performed in patients with a higher risk of lymph node involvement [10, 11]. Patients had PLND if they met the criteria based on available nomograms. PLND was performed according to the standard at the time of surgery [6, 12–14]. RP was performed either through open surgery or robot-assisted surgery, with the first robot-assisted procedure conducted in 2009. After 2009, the number of robot-assisted procedures grew rapidly, and by the late 2010s, nearly all procedures were performed using robotic assistance, with only a few exceptions. Data included the age at RP, preoperative prostate-specific antigen (PSA) level, and clinical and specimen tumour pathology [7, 10]. The risk of lymph node invasion was calculated using the Memorial Sloan Kettering Cancer Center (MSKCC) and Briganti 2012 nomograms [13, 15]. Information about nerve sparing surgery, comorbidities, and history of adjuvant treatments was extracted from the Danish National Registry of Patients [16]. The updated Charlson Comorbidity Index (CCI) at the time of RP was calculated based on the registered comorbidities up to 1 year before RP [17]. Postoperative follow-up included regular PSA measurements at the department performing the procedure and subsequent follow-up by GPs. The assessment of BF was based on PSA values extracted from the laboratory registry and assessed for all men with at least one PSA measurement registered within a year following RP and with no prior treatment for prostate cancer other than RP [18]. The laboratory registry has been stepwise-introduced per region since 2008. We determined BF as a PSA ≥ 0.2 ng/ml after a nadir of ≤ 0.1 ng/ml. Persistent PSA was included as BF at the time of the lowest measured PSA within the first year, as we intended to define men who were not cured. Salvage treatment was defined as any post-operative radiation or hormonal therapy administered, regardless of the underlying reason for treatment initiation (e.g. clinical decision-making or participation in clinical trials). Vitality status was extracted from the central person registry and cause of death from the Danish Registry of Causes of Death until December 31, 2022 [19]. The ICD-10 code of ‘C619’ was used to determine prostate cancer-specific death. All other causes of death were grouped as other causes of death.
Patients with pT0 and patients diagnosed with metastatic prostate cancer and patients with lymph node metastasis on conventional imaging were excluded to ensure homogeneity of the cohort, to include only patients undergoing PLND where nodal status was determined pathologically. Patients from Greenland and the Faroe Islands and individuals who emigrated were excluded because of a lack of data regarding follow-up after the RP. Hormonal therapy was defined as the administration of androgen deprivation therapy, Bicalutamide, or any novel hormonal therapy. To minimise the impact of concurrent clinical trial enrolment, patients receiving radiation therapy within 6 months following surgery were excluded.
Statistical analysis
A multivariable logistic regression is fitted to define the association between pre-operative characteristics and pN1 in our cohort, with pNx and pN0 defined as no event. The Aalen Johansen estimator for competing risk estimates the cumulative incidence of BF with subsequent treatment and death as competing risks, salvage treatment (salvage radiation or hormonal therapy) with death as a competing risk, and prostate cancer-specific death with other causes of death as a competing risk, all reported by Gray’s test. The pathological lymph node category (pNx, pN0, pN1) was stratified for all cumulative incidences. The observation period was from the time of RP to prostate cancer-specific death, other cause of death, or censoring (31-12-2022). Three multivariable cause-specific Cox (CSC) models were fitted including preoperative variables (age at RP, last PSA before RP, clinical T-category, Gleason grade group [GG] of last biopsy set before RP, percentage positive biopsies, calculated as the number of positive biopsies by the total number of biopsies, and CCI), perioperative variables (preoperative characteristics and pathological GG, and surgical margins), and perioperative variables + lymph node category for 10-year risk of BF and 15-year risk of prostate cancer-specific death. The performance of the three CSC models is assessed by calibration plot, the area under the curve (AUC) of the receiver operating characteristic (ROC), Brier scores, and decision curve analysis. Brier score is a measure of accuracy. It specifically is the mean sum between the predicted and observed risk. The lower the score, the better the accuracy. All statistical analyses were performed using R version 4.1.2 (R Development Core Team, Vienna, Austria) running on RStudio version 2022.07.01 (© 2009–2022 by Rstudio, Inc).
Results
A total of 15,515 men were treated with RPs between 2006 and 2021 (Figure 1). PLND was performed in 7,087 patients, with 1,010 patients having pN1 disease (Supplementary Figure 1). Generally, patients with pN1 and pN0 exhibited a more advanced stage of prostate cancer, elevated PSA levels, and a higher frequency of positive surgical margins compared to pNx (Table 1). Gleason score, PSA, tumour category, and percentage positive biopsies were associated with pN1 disease (Supplementary Table 1).
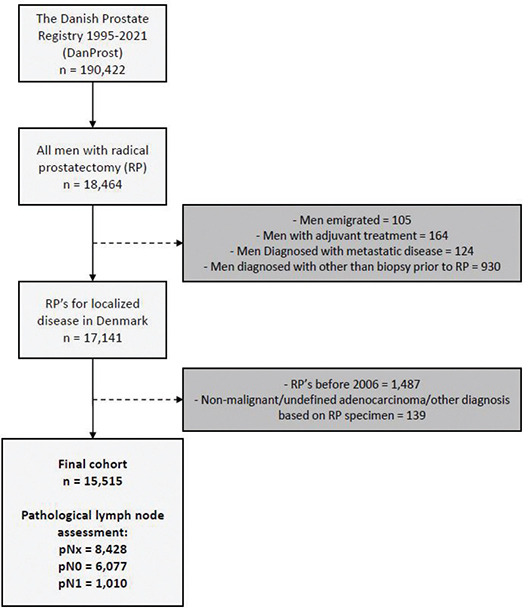
Figure 1. Flowchart illustration of the formation of the cohort.
The median time to censoring (follow-up) was 8.8 years (interquartile range [IQR]: 5.3–13) with 1,201 patients followed for more than 15 years. There were 11,416 men with PSA levels available, with a median of 7 PSA measurements (IQR: 4–10) taken for BF assessment. The overall 15-year cumulative incidence of BF, salvage therapy (radiation or hormonal therapy), and prostate cancer-specific death were 31% (95% confidence interval [95%CI]: 30–32), 27% (95%CI: 26–28), and 4.5% (95%CI: 3.9–5.0). The incidence of BF was not affected by the year of RP (Supplementary Figure 2). The 15-year cumulative incidence of BF was 22% (95%CI: 20–23), 37% (95%CI: 35–39), and 70% (95%CI: 65–76) for pNx, pN0, and pN1 (p < 0.001) (Figure 2A + Supplementary Table 2). Cumulative incidence of salvage radiation 15 years post-surgery was 13% (95%CI: 12–14), 20% (95%CI: 18–21), and 25% (95%CI: 20–29), for pNx, pN0, and pN1 (p < 0.001), and cumulative incidence of hormonal therapy 15 years post-surgery was 5.4% (95%CI: 4.6–6.3), 11% (95%CI: 10–13), and 60% (95%CI: 54–65), for pNx, pN0, and pN1 (p < 0.001) (Figure 2B/C + Supplementary Table 2). The cumulative incidence of prostate cancer-specific death 15 years post-surgery was 2.1% (95%CI: 1.6–2.6), 5.5% (95%CI: 4.6–6.5), and 25% (95%CI: 18–32), for pNx, pN0, and pN1 (p < 0.001) (Figure 2D + Supplementary Table 2).
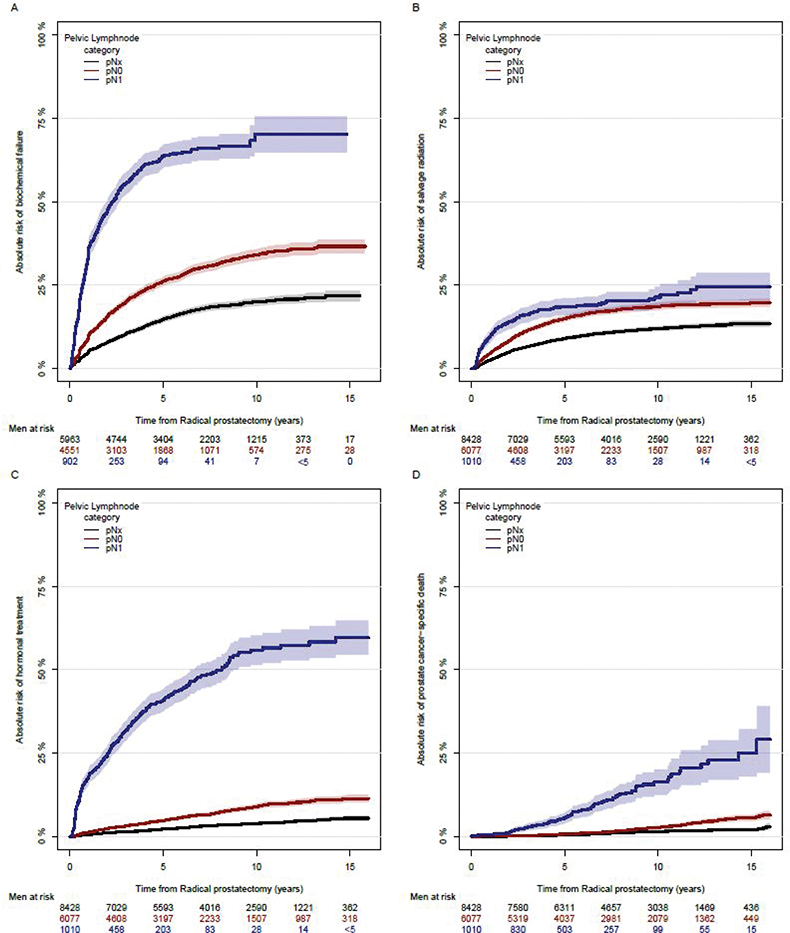
Figure 2. Univariable model of the absolute risk of biochemical failure (A), subsequent therapy (B+C), and prostate cancer-specific death (D) after curatively intended radical prostatectomy with pelvic lymph node dissection (pN0 and pN1) or without pelvic lymph node dissection (pNx) at any given point with a 15-year follow-up.
In men who underwent PLND, pN1 was associated with BF (hazard ratio: 2.2, 95%CI: 2.2–2.8) and prostate cancer-specific death (hazard ratio: 2.6, 95%CI: 1.83–3.7; Supplementary Table 3) compared to pN0 when adjusted for other perioperative variables. The AUCs of the 10-year BF for the perioperative and perioperative + lymph node category were 74% (95%CI: 72–77) and 76% (95%CI: 73–78), and the Brier scores were 20.1% (95%CI: 19.3–21.0) and 19.7% (95%CI: 18.8–20.5). The AUCs of the 15-year risk of prostate cancer death were 80% (95%CI: 76–84) and 80% (95%CI: 75–84) for the perioperative and perioperative + lymph node category, and the Brier scores were 6.2% (95%CI: 5.3–7.2) and 6.0% (95%CI:5.1–7.0). The addition of lymph nodes marginally increased the unweighted decision curve for BF and prostate cancer-specific death prediction (Supplementary Figure 3+4). We performed a sensitivity analysis for the prediction of BF that included only patients who underwent RP in 2014 or later to ensure comparable follow-up times. The model’s predictive performance remained similar, with AUCs not markedly different from those observed in the full cohort (Supplementary Table 4).
Multicollinearity was assessed as part of the review process and found not to influence the conclusions (Supplementary Table 5).
The AUCs of the 10-year BF stratified by the Briganti nomogram and MSKCC nomogram were 73% (95%CI: 70–75) for both and the Brier scores were 21.2% (95%CI: 20.5–22.0) and 21.1% (95%CI: 20.4–21.9). The AUCs of the 15-year prostate cancer-specific death stratified by the Briganti nomogram and MSKCC nomogram were 79% (95%CI: 74–85) and 82% (95%CI: 77–86), and the Brier scores were 6.9% (95%CI: 5.6–8.1) and 6.8% (95%CI: 5.5–8.1).
Discussion
Lymph node spread is a distinct disease entity that induces several alterations in the tumour immunity that facilitate further metastatic spread [20]. This raises the question of whether lymph node-positive disease can be cured if removed and/or if detection should be established to guide adjuvant interventions. Finding lymph node spread on imaging has historically been challenging because of the low sensitivity of conventional radiological procedures, such as computed tomography (CT) scans, making surgical lymphadenectomy an important tool to detect lymph node disease. Lymph node dissection in cancer surgery remains under debate due to an unclear impact on oncological outcomes, not only in prostate cancer but also in other cancers, most notably in cystectomy for muscle-invasive bladder cancer, where the lymph node template is similar to the template in RP [21, 22]. Cystectomy with extended lymphadenectomy increased positive lymph node yield without improving overall survival, as demonstrated in SWOG S1011 [23]. Our data show that most men with removed positive lymph nodes are likely to experience biochemical and clinical progression and that they have a high risk of prostate cancer-specific death. Despite our study design preventing us from quantifying the true magnitude of the effect of PLND, given the large proportion of men with pN1 undergoing subsequent treatment, the potential for cure appears limited. Therefore, the benefit of removing pN1 will primarily lie in delaying the need for further treatment. Our data confirm previous retrospective modelling studies that have found a particularly high risk of prostate cancer-specific death in patients with surgical pathological confirmed lymph node metastasis (pN1) compared to lymph node-negative (pN0) patients [24]. There are currently two randomised trials that show no benefit in terms of biochemical-free survival of extended compared to limited PLND [6, 14]. One of the two randomised trials recently published secondary outcomes showing a protective effect of extended PLND on metastasis development, but showed similar results of metastasis-free survival rate at 10 years between limited PLND and extended PLND (85%, 95% CI 81–89% vs. 88%, 95%CI 84–1%) [25]. Until these trials have published results on long-term oncological outcomes, the uncertainty of the benefit of performing PLND regarding the harms associated with the extended procedure remains.
If PLND is only to be performed for staging, the increased risk of lymphocele, deep venous thrombosis, and a higher 90-day mortality rate compared to no PLND must be considered [1]. Furthermore, extended PLND has a higher complication rate, longer operative time, higher risk of bleeding, and longer length of hospital stays than the limited PLND [3, 6]. We investigated the added value of PLND staging post-PLND decision. In post-PLND decision models with perioperative clinical variables, the lymph node category did not contribute substantially to distinguishing between patients at risk of recurrence and disease-specific death, questioning the usefulness of PLND in staging. This is especially evident as PSMA-PET and MRI are non-invasive alternatives for lymph node staging [26]. However, omitting PLND will raise questions about how disease recurrence is managed and may increase the proportion of men with persistent PSA following RP, where the evidence for disease management is currently low. Therefore, PLND will likely remain important in staging patients for selection in future trials until better imaging has been proven sufficient. Several studies have been performed and are in the pipeline to investigate the treatment options for men with persistent PSA following RP, such as the RADICALS-RT, RADICALS-HD, SPORTT, PRIMORDIUM, and ARASTEP [27–29]. These trials have investigated the use and treatment timing of radiotherapy, ADT, and androgen receptor pathway inhibitors (ARPI) in terms of metastasis-free survival. The development of targeted treatments for persistent and recurrent disease may eventually outperform PLND in long-term effectiveness, leading to a decreased use of PLND.
This study was limited by the inability to differentiate the number of malignant nodes removed, as this was not reported consistently in the registries. As a result, we excluded this variable to reduce the risk of reporting bias. PLND has been performed differently over time, and likely differences may have occurred based on local tradition and surgical experience; however, data have not demonstrated any significant impact of the extent of PLND on oncological outcome [6, 14]. Previous research has shown that two or fewer malignant lymph nodes had markedly better cancer-specific survival at 15-year follow-up compared with more than two malignant lymph nodes [30]. Thus, adding the number of lymph nodes may refine the prostate cancer-specific death predictions at 15 years, considering the marginal difference between the three models. Furthermore, the decision to perform PLND reflects the clinical practice within Denmark; consequently, comparing the long-term outcomes between pN1/pN0 and pNx reflects the selection for PLND in men with higher-risk disease, as shown by the clinical characteristics associated with pN1 disease. Thus, we reemphasise that our prediction models should be interpreted in the light of a current post-PLND treatment decision. Moreover, a proportion of patients in our cohort participated in clinical trials (e.g. RADICALS), which may have influenced treatment timing or decisions, particularly regarding early treatment for some patients. However, excluding these patients would have introduced selection bias and reduced the generalisability of our findings, as clinical trial participation is an inherent part of clinical practice. Strengths of our study include the large sample size and long follow-up compared to the duration and number of patients in the clinical trials conducted [1]. Finally, information on whether biopsies were performed following MR and the use of PSMA-PET in the diagnostic workup was not retrievable in the registers. However, PSMA-PET has not been used routinely in Denmark in the period studied, and although MRI-guided biopsies have been demonstrated to perform differently from standard transrectal biopsies, this change will unlikely influence results as MRI-guided biopsies will have been equally distributed among men regardless of whether PLND has been performed. A major strength is the longitudinal assessment of BF, salvage treatment, and death in the same cohort.
Conclusion
Men with positive lymph nodes after PLND face a high risk of BF, salvage treatment, and prostate cancer-specific death. Since adding the result of the PLND to the prediction model does not significantly enhance the discriminative ability, its role in staging warrants further examination. Given the associated harms, future randomised controlled trials should explore whether high-risk patients could avoid PLND or require more intensive treatment.
Data sharing statement
The data supporting these findings can be requested from the relevant Danish registers. However, access to the data may be subject to ethical and legal restrictions, and study-specific ethical permissions are required.
Author contribution statement
RGO: Concept and design, Analysis and interpretation of data, Drafting of the manuscript.
WBR: Concept and design, Analysis and interpretation of data, Drafting of the manuscript.
KB: Concept and design, Analysis and interpretation of data, critical revision of the manuscript for important intellectual content, Supervision.
AR: Concept and design, Analysis and interpretation of data, critical revision of the manuscript for important intellectual content, Supervision.
LK: Concept and design, critical revision of the manuscript for important intellectual content.
FB: Concept and design, critical revision of the manuscript for important intellectual content.
HVS: Concept and design, Acquisition of data, Analysis and interpretation of data, Statistical Analysis, Supervision.
References
[1] Fossati N, Willemse PPM, Van den Broeck T, et al. The benefits and harms of different extents of lymph node dissection during radical prostatectomy for prostate cancer: a systematic review. Eur Urol. 2017;72:84–109. https://doi.org/10.1016/j.eururo.2016.12.003
[2] Messing E, Manola J, Sarosdy M, et al. Immediate hormonal therapy compared with observation after radical prostatectomy and pelvic lymphadenectomy in men with node-positive prostate cancer. N Engl J Med. 1999;341(24):246–247. https://doi.org/10.1056/NEJM199912093412401
[3] Briganti A, Chun FKH, Salonia A, et al. Complications and other surgical outcomes associated with extended pelvic lymphadenectomy in men with localized prostate cancer. Eur Urol. 2006;50(5):1006–1013. https://doi.org/10.1016/j.eururo.2006.08.015
[4] Bader P, Burkhard FC, Markwalder R, et al. Is a limited lymph node dissection an adequate staging procedure for prostate cancer? J Urol. 2002;168(2):514–518. https://doi.org/10.1016/S0022-5347(05)64670-8
[5] Swindle PW, Kattan MW, Scardino PT. Markers and meaning of primary treatment failure. Urol Clin North Am. 2003;30(2):377–401. https://doi.org/10.1016/S0094-0143(02)00176-3
[6] Lestingi JFP, Guglielmetti GB, Trinh QD, et al. Extended versus limited pelvic lymph node dissection during radical prostatectomy for intermediate- and high-risk prostate cancer: early oncological outcomes from a randomized phase 3 trial. Eur Urol. 2021;79(5):595–604. https://doi.org/10.1016/j.eururo.2020.11.040
[7] Stroomberg HV, Larsen SB, Lanthén GS, et al. Danish Prostate Registry (DanProst) – an updated version of the Danish Prostate Cancer Registry, Methodology , and Early Results. 2023. https://pubmed.ncbi.nlm.nih.gov/37702859/
[8] Stroomberg HV, Larsen SB, Kjær Nielsen T, et al. Outcomes of Biopsy Grade Group 1 prostate cancer diagnosis in the Danish population. Eur Urol Oncol. 2024 Aug;7(4):770-777 https://doi.org/10.1016/j.euo.2023.10.005
[9] Stroomberg HV, Friberg AS, Helgstrand JT, et al. The impact of positive surgical margins on salvage radiation or androgen deprivation therapy following radical prostatectomy – a nationwide study. Acta Oncol (Madr). 2021;60(5):620–626. https://doi.org/10.1080/0284186X.2021.1898047
[10] Epstein JI, Allsbrook WC, Amin MB, et al. The 2005 International Society of Urological Pathology (ISUP) consensus conference on gleason grading of prostatic carcinoma. Am J Surg Pathol. 2005;29(9):1228–1242. https://doi.org/10.1097/01.pas.0000173646.99337.b1
[11] Dansk Urologisk Cancer Gruppe. Danish Prostate Cancer Group DaProCa: annual report 2022. https://www.dmcg.dk/siteassets/arsberetninger-og-udgivelser/arsberetninger/2022/daproca-arsberetning-2022.pdf
[12] Briganti A, Chun FKH, Salonia A, et al. Validation of a nomogram predicting the probability of lymph node invasion among patients undergoing radical prostatectomy and an extended pelvic lymphadenectomy. Eur Urol. 2006 Jun;49(6):1019–1027. https://doi.org/10.1016/j.eururo.2006.01.043
[13] Briganti A, Larcher A, Abdollah F, et al. Updated nomogram predicting lymph node invasion in patients with prostate cancer undergoing extended pelvic lymph node dissection: the essential importance of percentage of positive cores. Eur Urol. 2012 Mar;61(3):480–487. https://doi.org/10.1016/j.eururo.2011.10.044
[14] Touijer KA, Sjoberg DD, Benfante N, et al. Limited versus extended pelvic lymph node dissection for prostate cancer: a randomized clinical trial. Eur Urol Oncol. 2021;4(4):532–539. https://doi.org/10.1016/j.euo.2021.03.006
[15] Memorial Sloan Kettering Cancer Center pre-radical prostatectomy [Internet]. Available from: https://www.mskcc.org/nomograms/prostate/pre-op
[16] Lynge E, Sandegaard JL, Rebolj M. The Danish national patient register. Scand J Public Health. 2011;39(7):30–33. https://doi.org/10.1177/1403494811401482
[17] Quan H, Li B, Couris CM, et al. Updating and validating the charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol. 2011;173(6):676–682. https://doi.org/10.1093/aje/kwq433
[18] Arendt JFH, Hansen AT, Ladefoged SA, et al. Existing data sources in clinical epidemiology: laboratory information system databases in Denmark. Clin Epidemiol. 2020;12:469–475. https://doi.org/10.2147/CLEP.S245060
[19] Helweg-Larsen K. The Danish register of causes of death. Scand J Public Health. 2011;39(7):26–29. https://doi.org/10.1177/1403494811399958
[20] Reticker-Flynn NE, Zhang W, Belk JA, et al. Lymph node colonization induces tumor-immune tolerance to promote distant metastasis. Cell. 2022;185(11):1924. https://doi.org/10.1016/j.cell.2022.04.019
[21] Harter P, Sehouli J, Lorusso D, et al. A randomized trial of lymphadenectomy in patients with advanced ovarian neoplasms. N Engl J Med. 2019;380(9):822–832. https://doi.org/10.1056/NEJMoa1808424
[22] Gentilini OD, Botteri E, Sangalli C, et al. Sentinel lymph node biopsy vs no axillary surgery in patients with small breast cancer and negative results on ultrasonography of axillary lymph nodes: the SOUND randomized clinical trial. JAMA Oncol. 2023;9(11):1557–1564. Available from: https://jamanetwork.com/journals/jamaoncology/fullarticle/2809872
[23] Lerner SP, Tangen C, Svatek RS, et al. SWOG S1011: a phase III surgical trial to evaluate the benefit of a standard versus an extended lymphadenectomy performed at time of radical cystectomy for muscle invasive urothelial cancer. J Clin Oncol. 2023 Jun 1;41(16_suppl):4508. https://doi.org/10.1200/JCO.2023.41.16_suppl.4508
[24] Eggener SE, Scardino PT, Walsh PC, et al. Predicting 15-year prostate cancer specific mortality after radical prostatectomy. J Urol. 2011;185(3):15–27. https://doi.org/10.1016/j.juro.2010.10.057
[25] Touijer KA, Vertosick EA, Sjoberg DD, et al. Pelvic lymph node dissection in prostate cancer: update from a randomized clinical trial of limited versus extended dissection. Eur Urol. 2025 Feb 1;87(2): 253–260. https://doi.org/10.1016/j.eururo.2024.10.006
[26] Chow KM, So WZ, Lee HJ, et al. Head-to-head comparison of the diagnostic accuracy of prostate-specific membrane antigen positron emission tomography and conventional imaging modalities for initial staging of intermediate- to high-risk prostate cancer: a systematic review and meta-analysis. Eur Urol. 2023 Jul 1;84(1):36–48. https://doi.org/10.1016/j.eururo.2023.03.001
[27] Parker CC, Clarke NW, Cook AD, et al. Timing of radiotherapy after radical prostatectomy (RADICALS-RT): a randomised, controlled phase 3 trial. Lancet. 2020;396(10260):1413–1421. Available from: http://www.thelancet.com/article/S0140673620315531/fulltext
[28] Parker CC, Kynaston H, Cook AD, et al. Duration of androgen deprivation therapy with postoperative radiotherapy for prostate cancer: a comparison of long-course versus short-course androgen deprivation therapy in the RADICALS-HD randomised trial. Lancet. 2024 May 16 [cited 2024 May 29]. Available from: http://www.thelancet.com/article/S014067362400549X/fulltext
[29] Pollack A, Karrison TG, Balogh AG, et al. The addition of androgen deprivation therapy and pelvic lymph node treatment to prostate bed salvage radiotherapy (NRG Oncology/RTOG 0534 SPPORT): an international, multicentre, randomised phase 3 trial. Lancet. 2022;399(10338): 1886–1901. https://doi.org/10.1016/S0140-6736(21)01790-6
[30] Briganti A, Karnes JR, Da Pozzo LF, et al. Two positive nodes represent a significant cut-off value for cancer specific survival in patients with node positive prostate cancer. A new proposal based on a two-institution experience on 703 consecutive N+ patients treated with radical prostatectomy, E. Eur Urol. 2009;55(2):261–270. https://doi.org/10.1016/j.eururo.2008.09.043