ORIGINAL RESEARCH ARTICLE
Testicular torsion Point-based Assessment and Imaging tool - identifying Need for Surgical exploration (TPAINS): a clinical algorithm for detecting testicular torsion
Nathalie Dahlgrena  , Gustav Sundströma, Charlotta Nilssonb and Magnus Wageniusc
, Gustav Sundströma, Charlotta Nilssonb and Magnus Wageniusc
aDepartment of Radiology, Department of Clinical Sciences, Helsingborg Hospital, Lund University, Helsingborg, Sweden; bDepartment of Pediatrics, Department of Clinical Sciences, Helsingborg Hospital, Lund University, Helsingborg, Sweden; cDepartment of Urology, Department of Clinical Sciences, Helsingborg Hospital, Lund University, Helsingborg, Sweden
ABSTRACT
Objective: Testicular torsion (TT) is a medical emergency, difficult to identify solely through clinical evaluation. This study aims to develop an assessment algorithm with a safe lower threshold for complementary ultrasound.
Material and methods: Males between 1 and 30 years of age assessed for suspected TT during the years 2019 – 2023 were retrospectively included. Clinical assessments were conducted by primarily nonurologists and ultrasounds by radiologists. An assessment algorithm named Testicular torsion Point-based Assessment and Imaging tool - identifying Need for Surgical exploration (TPAINS) was developed based on symptoms showing significant correlation with TT.
Results: Of the 417 patients included, 68 (16%) were surgically explored and 33 (8%) diagnosed with TT. Six symptoms showing a significant association with TT were combined for the development of the algorithm TPAINS. With a cut-off value of ≥2 points, TPAINS showed a sensitivity of 100% (confidence interval, CI: [90, 100]), specificity 54% (CI [49 – 59]), and an AUC-value of 0.89 (95% CI [84 – 94]).
Conclusions: This study concludes that symptom-based evaluation, together with a low threshold for ultrasound, is a promising approach for the detection of TT. The developed algorithm, TPAINS, includes an ultrasound assessment and focuses on safe lower thresholds for further clinical actions – hoping for a reduced rate of unnecessary surgical explorations.
KEYWORDS: Testicular torsion; TWIST score; ultrasound; spermatic cord torsion; assessment algorithm
Citation: Scandinavian Journal of Urology 2026, VOL. 61, 92–98. https://doi.org/10.2340/sju.v61.45578.
Copyright: © 2026 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 14 September 2025; Accepted: 3 February 2026; Published: 30 March 2026
CONTACT: Nathalie Dahlgren Na5354da-s@student.lu.se Helsingborgs Lasarett, Svartbrödragränden 3, 251 87 Helsingborg, Sweden
Competing interests and funding: The authors declare that there is no conflict of interest.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Introduction
One of the most acute scrotal conditions is torsion of the spermatic cord, also referred to as testicular torsion (TT) [1]. The incidence peaks during adolescence, affecting reportedly 3.8 – 24/100 000 males <29 years of age each year [2–4]. Early diagnosis and treatment are crucial to avoid testicular loss [5, 6]. However, symptoms associated with TT are common reasons for visits to the emergency department (ED). Epididymitis and torsion of the appendix testis are two examples of nonurgent scrotal conditions that can be difficult to symptomatically differentiate from TT. At the same time, abdominal pain has shown to be the main symptom of TT in some boys, unfortunately misleading clinicians and prolonging the time until correct diagnosis and treatment [7–10]. This makes it a diagnostic challenge in the ED, risking a high number of unnecessary urgent surgical explorations [11]. In 2013, the risk assessment tool ‘Testicular Workup for Ischemia and Suspected Torsion’ (TWIST) score was developed as a help for urologists assessing patients for detection of TT. The aim with TWIST score was reducing the number of unnecessary ultrasound assessments. It has three levels of suspicion based on five clinical findings, recommending Doppler ultrasonography (DUS) or urgent surgical exploration (SE) when scores are ≥3 [12]. Attempts to validate TWIST score when assessed by nonurologists have shown a lower accuracy [13]. Between 7 and 26% of patients with TT have in three different prospective studies scored as low risk. This means recommendation of no further in-hospital care. The same prospective studies lack necessary methodology regarding the ultrasound assessment. Information about which ultrasound findings indicate presence of TT are missing [14–16]. Previous studies on ultrasound alone report detection of spermatic cord rotation, not affected DUS signal, being reliable for detection of TT [17–20]. With a condition challenging to detect in the ED, nonurologists as primary assessors and access to scrotal ultrasound, there is a need for a new scoring algorithm to minimize the risk of patients being misdiagnosed. There is also a need for clear ultrasound guidelines, increasing the chances for fast and effective communication. This study aims to introduce an assessment algorithm that addresses these needs.
Study objective: A clinical assessment algorithm that detects all patients with TT while still keeping a lower threshold for further in-hospital assessments.
Materials and methods
This is a retrospective study of 417 patients in Helsingborg hospital, Sweden. Parts of this study population were previously analyzed regarding ultrasound as a diagnostic tool for TT [20]. Ethical approval was obtained by the Swedish Ethical Review Authority, ref 2023-07774-01. Data were analyzed anonymously.
Study sample
This study includes patients referred for ultrasound assessment or directly surgically explored due to suspected TT. Patients referred for acute scrotal ultrasound assessment between January 2019 and December 2023 were listed in the imaging program Sectra PACS IDS7. Inclusion criteria for the sample assessed with ultrasound were referral according to the current Helsingborg assessment algorithm for TT, 403 in total. Exclusion criteria were cases of nonurgent examinations, cryptorchidism, detorsion in the ED prior to the ultrasound assessment and cases where the ultrasound assessment of the spermatic cord for different reasons could not be completed (n = 14). This led to a remaining number of 389 patients. Through the operation registration program Orbit, patients surgically explored under the codes KFA00, KFA96, and KFA40 were extracted and matched to the study sample. A total of 40 patients matched as previously assessed with ultrasound according to the current algorithm. In addition, 28 patients had been surgically explored directly after the physical examination in the ED. No exclusions were made from the group of patients who were surgically explored without a preoperative ultrasound assessment. The upper age limit for inclusion was absent for these patients. This led to a final study sample of 417 patients. Patients in Sectra PACS were listed with a study number for anonymization during data collection and analyses. Patients directly surgically explored had their study number connected to their personal identification number saved according to current safety rules. The flow chart for exclusions is shown in Figure 1.
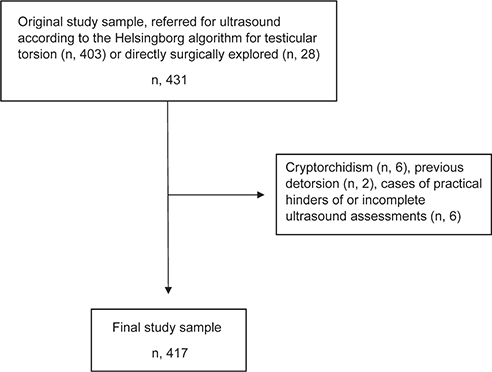
Figure 1. Flow chart for inclusion and exclusion criteria from the original study sample.
Definition of testicular torsion
TT is defined as ongoing TT, verified by surgical exploration (SE). Patients showing signs of recent detorsion were diagnosed with ITT, but in this study not analyzed as TT. The limit for concluding present signs of ongoing TT on ultrasound is spermatic cord rotation ≥180 degrees. These conclusions are based on the assessor’s own estimation and are not objectively measured.
The Helsingborg assessment algorithm for testicular torsion
The current Helsingborg TT algorithm involves an ultrasound assessment within 60 min for patients who are clinically assessed as ´low/ intermediate risk for TT´ Further criteria for urgent ultrasound are age 1–30 years and symptom duration <48 h. When TT is suspected, the recommendation is instead urgent SE without a preoperative ultrasound assessment. This risk assessment is conducted without the use of scoring systems. Patients with suspected TT are in the Helsingborg ED assessed by emergency doctors, general doctors, surgeons, and urologists.
TWIST score
In this study, TWIST score was used as a reference for comparison. This was due to previously published validations and a local experience that the TWIST score has been accepted as valid in ED settings.
Data collection
Following data were collected from the patients’ medical journals (Melior, Cerner Corporation): age, symptom duration until referral of ultrasound (or medical journal record of decision of SE for the group not preceding a preoperative ultrasound), incidence of scrotal trauma, incidence of previous similar episodes (patients describing previous transient episodes), pain character (sudden onset, intermittent pain), abdominal pain, nausea/vomiting, signs of scrotal inflammation, absence of cremasteric reflex, ascendance or horizontally positioned testicle, testicular induration, diagnosis, and treatment if surgically explored. Absent information on duration was registered as missing data and excluded from statistical analysis. Absent information on symptoms was registered as ‘no symptom of’. An exception from this was made regarding symptoms included in the TWIST score. For increased reliability, absent information regarding TWIST score symptoms was registered as missing values. These patients were therefore excluded from score analysis. Patients with a concluded clear reduction of the cremasteric reflex on the affected side were registered as ‘absent cremasteric reflex’. Patients with a concluded probable slight reduction were registered as unaffected. The reflex did not count as absent if it was reported bilaterally as nondetectable. The ultrasound of patients diagnosed with TT was blindly reassessed by a senior uroradiologist. The same radiologist and a senior urologist also verified all exclusions from the study sample and registration of final assessments. Patients where SE concluded potential signs of recent spontaneous cord detorsion were registered as intermittent testicular torsion (ITT) but analyzed as no TT as ongoing TT could not be surgically verified.
Ultrasound specifics
Ultrasound assessments for TT in Helsingborg are carried out by a radiologist with a minimum of 12 months of training. Assessment is conducted using a 15–18 MHz linear transducer (GE HealthCare Logiq E10). Patients are assessed in a supine position. It includes assessment in both longitudinal and transverse planes and control of the unaffected side. The spermatic cord is visualized in its full length using gray scale ultrasound. Comparison of Doppler signal is accomplished with a side- by-side transversal image.
Statistical analyses
Statistical analyses were conducted using IBM SPSS version 28.0.1.0. Multiple logistic regression was used for association analysis between each symptom and TT. Analyzed symptoms were sudden severe scrotal pain, intermittent pain character, previous transient episodes, scrotal trauma, abdominal pain, nausea/vomiting, signs of scrotal inflammation/edema, ascendance of testis or horizontal lie, absent cremasteric reflex, and testicular induration. Adjustments for predictors were made by combining all symptoms in the regression analysis. Results were presented as adjusted odds ratios (OR) with 95% confidence interval (CI), p < 0.05 for statistical significance. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated with the one-sample proportion test. The same test was used for the calculation of CI for sensitivity and specificity. After analyzing sensitivity and specificity for TPAINS, a Receiver Operating Characteristic (ROC) curve was calculated for measuring the area under the curve (AUC).
Development of the scoring algorithm
Among the analyzed symptoms showing statistically significant association with TT, combinations of symptoms were analyzed. Due to sample size, this was accomplished without statistical tests. Combinations of symptoms were tested by calculating a score for each patient in the final study sample. Different combinations and weighted scores were tested with the goal of finding a combination including all patients with TT while still excluding as many patients without TT as possible. Furthermore, a ‘one point per symptom’ system was the aim for a user-friendly and memorable algorithm.
Results
Out of the 417 patients included for final analyses, 68 (16%) were surgically explored and 33 (8%) diagnosed with TT. The median age in patients diagnosed with TT was 16 years (Table 1). None of the 349 patients assessed with ultrasound solely had later revisits (within 1 year) registered in their medical journal indicating signs of missed TT. Of the 10 analyzed symptoms presented in Table 2, eight showed a significant association with TT.
Score system
Testicular torsion Point-based Assessment and Imaging tool – identifying Need for Surgical exploration (TPAINS)
Six symptoms were included in the newly developed scoring system, named TPAINS, see Figure 2. These were: (1) Sudden scrotal pain onset. (2) Abdominal pain. (3) Nausea/vomiting. (4) Previous transient episodes. (5) Scrotal inflammation. (6) Ascendance of testis and/or horizontal lie. Analyses showed TPAINS, with a cut-off value of ≥2 points, to have a sensitivity of 100% (CI [90, 100]), specificity 54% (CI [49 – 59]), PPV 15%, and NPV 100%. The AUC for TPAINS showed 0.89 (95% CI [84 – 94]). A presentation of TPAINS analyses is shown in Table 3. Among the 11 patients who were not diagnosed with TT but showed surgical signs of ITT, 100% scored ≥2 on TPAINS.
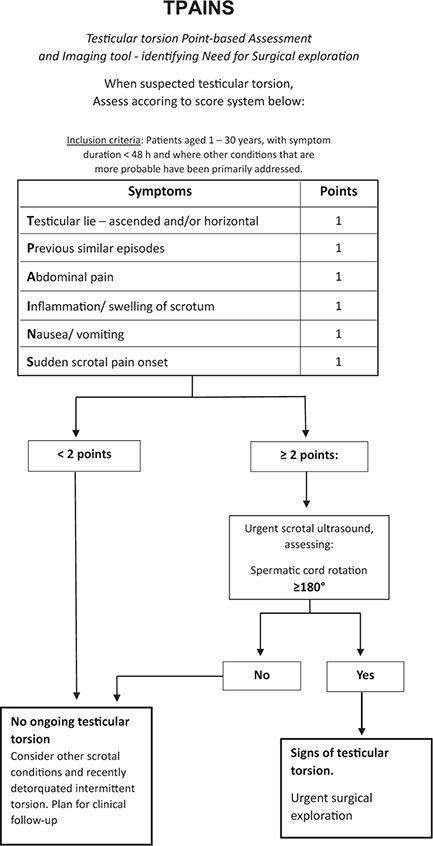
Figure 2. The proposed algorithm Testicular torsion Point-based Assessment and Imaging tool - identifying Need for Surgical exploration (TPAINS). With ≥2 points as a cut-off for needing an ultrasound, the TPAINS symptom score shows a sensitivity of 100% (confidence interval (CI) 90 – 100) and specificity of 54% (CI 49 – 59).
TWIST score
Three of the patients diagnosed with TT (15 of the total study sample) were excluded from TWIST score analyses due to missing symptom values. TWIST score analyses, therefore, included 402 patients in total. Of the 33 patients diagnosed with TT, eight (24%) were not detected by the TWIST score. Sensitivity and specificity for the TWIST score were 72% (CI [54, 85]) and 79% (CI [74, 83]), respectively, with PPV 22% and NPV 97%.
Discussion
This retrospective study analyzed symptoms in patients assessed in the Helsingborg ED with suspicion of TT. Eight of the 10 analyzed symptoms showed significant associations with TT. Six of them were finally, after combining symptoms to find a safe lower threshold for complementary ultrasound, included in the development of the algorithm TPAINS (Figure 2). TPAINS consists of an initial assessment of testicular lie, previous similar/transient episodes, abdominal pain, signs of scrotal inflammation, nausea/vomiting, sudden scrotal pain onset and recommends an ultrasound assessment of the spermatic cord when scores are ≥2. Another cut-off value is then 180 degrees of cord rotation for urgent SE, based on previously published data in which all patients with TT were detected based on spermatic cord rotation [20]. With an initial cut-off value of ≥2, TPAINS detected all 33 patients with TT. TWIST score failed to detect 24% of these patients. Signs of recent spontaneous detorsion were seen in 11 patients. Difficulties in estimating the amount of time passed as detorsion made these 11 patients not analyzed as having TT. However, every one of these patients were detected as scores ≥2 on TPAINS. They were also either detected as ≥180 degrees cord rotation on ultrasound or showed similar signs of recent torsion status.
Not all symptoms showing significant correlation with TT were included in TPAINS. Initially, a score was given for each of the eight symptoms with significant association, also with weighted scores. This inevitably gave a wide inclusion for ultrasound but showed to include the vast majority of patients with other scrotal disorders. When instead raising the threshold, patients with TT were missed. Two of the symptoms with significant association, trauma and testicular induration, were in the final score setting excluded. Among the patients with TT, only one presented after scrotal trauma. Previous studies show that patients with scrotal trauma more often have other testicular injuries, such as hematoma/tissue rupture, making these patients already recommended for acute scrotal ultrasound [21, 22]. Testicular induration was seen to co-vary with several other significantly associated symptoms. However, these data show the diversity of symptoms these patients can present with.
The relatively small study sample increases the risk of overestimating symptom association and AUC and might explain the wide CIs seen in Table 2. The AUC represents the calculated probability value for TPAINS to distinguish TT from other conditions. Analyzing patients diagnosed with recent detorsion/ITT as TT might have affected this value. A larger study sample of patients with TT could have generated a higher statistical power, allowing for reliable analyses on different symptom combinations. This score-based algorithm is exploratory: prospective validations are needed.
Abdominal pain has been shown in several studies to be present in a significant number of patients with TT [9, 10]. This might contribute to a difficulty in knowing when further clinical actions for TT are needed. In addition, this study indicates that the cremasteric reflex can be difficult to detect. It was also shown to be absent in a significant number of patients without TT. Guo et al. [23] have previously concluded assessment of the cremasteric reflex to be unreliable. In this study, a significantly reduced cremasteric reflex on the affected side was registered as absent. This might have contributed to falsely high TWIST scores.
The Helsingborg ED does not primarily have urologists addressing patients presenting with acute scrotum. The original study from Barbosa et al. [12] developed the TWIST score as a tool for urologists, focused on reducing the number of unnecessary ultrasound assessments. Out of the 51 patients diagnosed with TT in their study sample, 15 (29%) needed orchiectomy, and the mean symptom duration was 25 h. They discussed the possibility that the chances to detect typical scrotal symptoms might increase later in the torsion process. This can indicate that patients who seek emergency care early have a higher risk of being misdiagnosed and/or have a prolonged time until SE. A reliable scoring system needs to be applicable in all stages of time after torsion onset, especially in the first 6 h when chances of orchiopexy are the highest. This study does not present exact durations due to the risk of registration bias in retrospective data but has grouped them into time blocks for estimation. Results show that patients with TT can seek the ED at any time within 48 h although it was more common in this study to present with a symptom duration <6 h. The number of patients requiring orchiectomy was in this study sample comparably low (12%).
Prospective studies have been conducted in attempts to validate TWIST score when assessed by nonurologists. In three of these, between 7 and 26% of patients with TT scored as low risk/<3 points [14–16]. In our study sample, this number was 24%. A systematic review by Choudhury et al. [13] in 2022 concluded TWIST score being useful mainly as a guide for the clinician. In clinical practice, a low-risk score that cannot be trusted might not be helpful enough. An ultrasound will then become the safest way to detect TT without surgically exploring every patient where the clinician has a slight suspicion.
Assessing the spermatic cord with ultrasound for the detection of cord rotation has, in multiple studies, been shown to be a reliable method to detect TT [18, 24, 25]. Patients with TT in this study sample were all detected using 180 degrees as a lower limit of cord rotation. Access to fast ultrasound assessments has previously not shown to negatively impact surgical outcome in patients with TT. Instead, it has been shown to lower the number of negative SEs [11]. This study supports these conclusions. It can be argued that ultrasound then should be used more widely to avoid both negative SEs and the risk of missing cases of TT. However, a TPAINS score <2 was, in this study sample, shown to be a safe sign that ultrasound could be avoided. The radiologists in Helsingborg hospital prioritize ultrasound referrals for TT above other planned assessments for achieving a short preoperative waiting time. This is an important aspect as low-risk ultrasound assessments might contribute to inadequate use of resources. However, ultrasound is safe and does not come with the same potential stress or risk of complications that urgent SE does [26, 27]. Future validations on TPAINS might show whether a cut-off for direct urgent SE without a preoperative ultrasound is possible to include. This might increase its generalizability, as access to urgent ultrasound varies between hospitals.
Seeing as the study sample was restricted to include patients already suspected of having TT, the results might be biased by selection difficulties. A wider inclusion of patients in the ED, with lower degrees of suspicion, would possibly have affected the outcome to be more representative for all levels of suspicion. Regardless, these data give an indication of what symptoms are relevant in initial assessment. It also illustrates the wide range of symptoms and complexity that this condition represents.
Another weakness in this study was that all patients were not surgically explored for a final diagnosis. However, no patients who were sent home without or after an ultrasound assessment had visits to the ED associated with TT/scrotal conditions registered in their medical journals for the following year. With the support of previous studies showing ultrasound to be a reliable preoperative tool and this study presenting a scoring tool with a relatively low threshold for ultrasound, it might not be ethically justifiable to conduct urgent SE on every boy or young man assessed by the algorithm.
This study introduces a scoring system that aims to be a practical assessment tool also for nonurologists. To enhance its usability in the high-pressure ED environment, TPAINS was designed as a mnemonic for the initial physical assessment. An aim for zero missed TTs and the finding of a reliable lower threshold for a complementary ultrasound were prioritized in the development of TPAINS. TPAINS suggest a low threshold system, both for symptom and ultrasound assessment, to minimize the risk of missing torsions. This means accepting ultrasound as a necessary part of the assessment chain.
Acknowledgments
We thank Axel Ström, statistician from ‘Clinical Studies Sweden, Forum South’, for statistical assistance.
References
[1] Leone N, Morlacco A, D’Elia C, et al. A retrospective multicentric analysis on testicular torsion: is there still something to learn? Scand J Urol. 2021;55(5): 408–411. https://doi.org/10.1080/21681805.2021.1889026
[2] Zhao LC, Lautz TB, Meeks JJ, et al. Pediatric testicular torsion epidemiology using a national database: incidence, risk of orchiectomy and possible measures toward improving the quality of care. J Urol. 2011;186(5): 2009–2013. https://doi.org/10.1016/j.juro.2011.07.024
[3] Sugrue DD, O’Connor E, Davis N. Testicular torsion in Ireland: a 10-year analysis of incidence and risk of orchidectomy. Ir J Med Sci. 2022;191(5):2267–2274. https://doi.org/10.1007/s11845-021-02816-8
[4] Socialstyrelsen. Statistikområden, Testikeltorsion. Stockholm: Socialstyrelsen: 2024 [cited 2024 Mar 27]. Available from: https://sdb.socialstyrelsen.se/if_par/val.aspx
[5] Lian BS, Ong CC, Chiang LW, et al. Factors predicting testicular atrophy after testicular salvage following torsion. Eur J Pediatr Surg. 2016;26(1):17–21. https://doi.org/10.1055/s-0035-1566096
[6] Steeman A, Ngatchou W, Ramadan AS, et al. Impact of treatment delays on outcome of acute testicular torsion: a 15-year retrospective study. Acta Chir Belg. 2022;122(2):116–122. https://doi.org/10.1080/00015458.2021.1883391
[7] Sweet DE, Feldman MK, Remer EM. Imaging of the acute scrotum: keys to a rapid diagnosis of acute scrotal disorders. Abdom Radiol (NY). 2020;45(7):2063–2081. https://doi.org/10.1007/s00261-019-02333-4
[8] Gkalonaki I, Patoulias I, Anastasakis M, et al. The challenging diagnosis of acute scrotum: remaining difficulties and further insights. Folia Med Cracov. 2022; 62(3):91–100.
[9] Vasconcelos-Castro S, Soares-Oliveira M. Abdominal pain in teenagers: beware of testicular torsion. J Pediatr Surg. 2020;55(9):1933–1935. https://doi.org/10.1016/j.jpedsurg.2019.08.014
[10] Goetz J, Roewe R, Doolittle J, et al. A comparison of clinical outcomes of acute testicular torsion between prepubertal and postpubertal males. J Pediatr Urol. 2019;15(6):610–616. https://doi.org/10.1016/j.jpurol.2019.07.020
[11] Teurneau-Hermansson K, Zindovic I, Jakobsson J, et al. Doppler ultrasound improves diagnostic accuracy for testicular torsion. Scand J Urol. 2021;55(6):461–465. https://doi.org/10.1080/21681805.2021.1962404
[12] Barbosa JA, Tiseo BC, Barayan GA, et al. Development and initial validation of a scoring system to diagnose testicular torsion in children. J Urol. 2013;189(5):1859–1864. https://doi.org/10.1016/j.juro.2012.10.056
[13] Choudhury P, Saroya KK, Anand S, et al. Unjumbling the TWIST score for testicular torsion: systematic review and meta-analysis. Pediatr Surg Int. 2023;39(1):137. https://doi.org/10.1007/s00383-023-05401-5
[14] Frohlich LC, Paydar-Darian N, Cilento BG, Jr., et al. Prospective validation of clinical score for males presenting with an acute scrotum. Acad Emerg Med. 2017;24(12):1474–1482. https://doi.org/10.1111/acem.13295
[15] Sheth KR, Keays M, Grimsby GM, et al. Diagnosing testicular torsion before urological consultation and imaging: validation of the TWIST score. J Urol. 2016;195(6):1870–1876. https://doi.org/10.1016/j.juro.2016.01.101
[16] Lim X, Angus MI, Panchalingam V, et al. Revisiting testicular torsion scores in an Asian healthcare system. J Pediatr Urol. 2020;16(6):821 e1–821 e7. https://doi.org/10.1016/j.jpurol.2020.09.023
[17] McDowall J, Adam A, Gerber L, et al. The ultrasonographic ‘whirlpool sign’ in testicular torsion: valuable tool or waste of valuable time? A systematic review and meta-analysis. Emerg Radiol. 2018;25(3):281–292. https://doi.org/10.1007/s10140-018-1579-x
[18] Kalfa N, Veyrac C, Baud C, et al. Ultrasonography of the spermatic cord in children with testicular torsion: impact on the surgical strategy. J Urol. 2004; 172(4 Pt 2):1692–1695; discussion 1695. https://doi.org/10.1097/01.ju.0000138477.85710.69
[19] Vijayaraghavan SB. Sonographic differential diagnosis of acute scrotum: real-time whirlpool sign, a key sign of torsion. J Ultrasound Med. 2006;25(5):563–574. https://doi.org/10.7863/jum.2006.25.5.563
[20] Dahlgren N, Sundstrom G, Wagenius M, et al. A validation of ultrasound as a diagnostic tool for the detection of testicular torsion. Acta Radiol. 2025;66(8):878-884. https://doi.org/10.1177/02841851251331560
[21] Fenton LZ, Karakas SP, Baskin L, et al. Sonography of pediatric blunt scrotal trauma: what the pediatric urologist wants to know. Pediatr Radiol. 2016;46(7):1049–1058. https://doi.org/10.1007/s00247-016-3600-4
[22] Schilliro ML, Lonardo V, Iacobellis F, et al. Multiparametric ultrasound in acute scrotum: a comprehensive review with special emphasis on contrast-enhanced ultrasound. J Ultrasound. 2025;28(2):305–321. https://doi.org/10.1007/s40477-025-01017-8
[23] Guo X, Sun L, Lei W, et al. Management of testicular torsion <360 degrees in children: a single-center, retrospective study. J Int Med Res. 2020;48(4):300060519895861. https://doi.org/10.1177/0300060519895861
[24] Xu Z, Wu J, Ni S, et al. The diagnostic value of ultrasound in pediatric testicular torsion with preserved flow. Front Pediatr. 2022;10:1001958. https://doi.org/10.3389/fped.2022.1001958
[25] Waldert M, Klatte T, Schmidbauer J, et al. Color Doppler sonography reliably identifies testicular torsion in boys. Urology. 2010;75(5):1170–1174. https://doi.org/10.1016/j.urology.2009.07.1298
[26] Hart J, Pastore G, Jones M, et al. Chronic orchalgia after surgical exploration for acute scrotal pain in children. J Pediatr Urol. 2016;12(3):168 e1–168 e6. https://doi.org/10.1016/j.jpurol.2015.11.014
[27] Ali Benali N, Pradere B, Lannes F, et al. TORSAFUF – Surgical exploration for torsion of spermatic cord suspicion and risk factors for unnecessary surgery: results of a French nationwide retrospective study on 2940 patients. Prog Urol. 2022;32(2):92–100. https://doi.org/10.1016/j.purol.2021.10.011