RESEARCH LETTER
Application of the International Bladder Cancer Group prediction model for recurrence-free survival on a national cohort of primary intermediate risk non-muscle invasive bladder cancer
Denis Mesinovica,b, Johannes Bobjera,b, Oskar Hagberga, Firas Aljaberyc, Truls Gårdmarkd,e, Staffan Jahnsonc, Tomas Jerlströmf, Henrik Kjölhedeg,h, Per-Uno Malmströmi, Viveka Ströckg,h, Karin Söderkvistj, Anders Ullénk,l, Lars Holmbergi,m, Christel Häggströmn and Fredrik Liedberga,b
aDepartment of Translational Medicine, Lund University, Malmö, Sweden; bDepartment of Urology Skåne University Hospital, Malmö, Sweden; cDepartment of Clinical and Experimental Medicine, Division of Urology, Linköping University, Linköping, Sweden; dDepartment of Urology, Danderyd Hospital, Stockholm, Sweden; eDepartment of Molecular Medicine and Surgery, Karolinska Institute, Stockholm, Sweden; fDepartment of Urology, School of Medical Sciences, Faculty of Medicine and Health, Örebro University, Örebro, Sweden; gDepartment of Urology, Sahlgrenska University Hospital, Gothenburg, Sweden; hInstitute of Clinical Sciences, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden; iDepartment of Surgical Sciences, University of Uppsala, Uppsala, Sweden; jOncology, Department of Diagnostics and Intervention, Umeå University, Umeå, Sweden; kDepartment of Pelvic Cancer, Genitourinary Oncology and Urology Unit, Theme Cancer, Karolinska University Hospital, Stockholm, Sweden; lDepartment of Oncology and Pathology, Karolinska Institute, Stockholm, Sweden; mSchool of Cancer and Pharmaceutical Sciences, King’s College London, London, United Kingdom; nNorthern Register Centre, Oncology, Department of Diagnostics and Intervention, Umeå University, Umeå, Sweden
ABSTRACT
The International Bladder Cancer Group (IBCG) has proposed a prognostic model for intermediate risk (IR) non-muscle invasive bladder cancer (NMIBC) for clinical decision-making. We applied the IBCG IR model in a population-based Swedish setting in patients with primary IR NMIBC diagnosed 2013–2014 in BladderBaSe 2.0. Patients were stratified into low-risk (unifocal and tumour size < 3 cm) and intermediate-risk (multiple and/or tumour size ≥ 3 cm) for estimation of 1- and 3-year recurrence-free survival (RFS). Among 710 patients with IR NMIBC, 329 (46%) and 381 (54%) were categorized as low- and intermediate-risk, respectively. Probabilities of disease recurrence or death at 1 and 3 years in low-risk patients were 19% (95% confidence interval [CI]: 15–23) and 41% (95% CI: 35–46), versus 27% (95% CI: 22–31) and 45% (95% CI: 40–50) in the intermediate-risk group. In a sensitivity analysis including only patients receiving serial adjuvant instillations (n = 152) the corresponding probabilities at 1 and 3 years were 19% (95% CI: 10–28) and 33% (95% CI: 22–43) versus 15% (95% CI: 7–23) and 31% (95% CI: 20–41), respectively. Thus, no clinically meaningful difference in recurrence-free survival was observed between International Bladder Cancer Group low- and intermediate-risk groups in this population-based primary non-muscle invasive bladder cancer setting.
KEYWORDS: Intermediate risk; non-muscle invasive bladder cancer; risk stratification
Citation: Scandinavian Journal of Urology 2026, VOL. 127, 127–130. https://doi.org/10.2340/sju.v61.45712.
Copyright: © 2026 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 23 November 2025; Accepted: 16 February 2026; Published: 17 April 2026
CONTACT: Denis Mesinovic denis.mesinovic@med.lu.se Department of Translational Medicine, Lund University, Jan Waldenströms gata 35, 205 02 Malmö, Sweden
Supplemental data for this article can be accessed online at https://doi.org/10.2340/sju.v61.45712
Competing interests and funding: The authors report no conflicts of interest.
This work was supported by the Swedish Cancer Society (grant numbers CAN 22 2021 and CAN 2023/2807), Swedish Research Council (2021‐00859), a regional agreement between Umeå University and Region Västerbotten (ALF), Skåne University Hospital Research Funds, the Swedish Society of Medicine, the Cancer Research Fund at Malmö General Hospital, Sjöberg Foundation, Maud and Birger Gustavsson Research Foundation, the Hjelm Family Foundation for Medical Research, Anna-Lisa and Sven-Eric Lundgren Research Foundation, Gösta Jönsson Research Foundation, the Foundation of Urological Research (Ove and Carin Carlsson Bladder Cancer Donation) and Hillevi Fries Research Foundation.
Introduction
Due to heterogeneity within the intermediate risk (IR) group in non-muscle invasive bladder cancer (NMIBC), the International Bladder Cancer Group (IBCG) has proposed a three-group stratification model for IR patients based on the following five risk factors for recurrence-free survival (RFS): tumour size ≥ 3 cm, tumour multiplicity, early recurrence (< 1 year), frequent recurrences (> one per year), and failure of previous intravesical treatment. The risk categories are grouped as low (no risk factors), intermediate (one or two risk factors) and high (three or more risk factors) IR NMIBC [1]. Thus, in primary NMIBC only tumour size and multiplicity are possible factors. Validation of the IBCG IR prognostic model in nine academic referral centers with 677 patients treated with transurethral resection (TURB) and serial adjuvant instillations showed clinically relevant differences in RFS [2], supporting a stratified approach for clinical decisions regarding follow-up and adjuvant therapies [3, 4]. We applied the IBCG IR prognostic model in a population-based setting with primary IR NMIBC.
Patients and methods
All 3,938 patients diagnosed with NMIBC 2013–2014 in the Swedish National Register for Urinary Bladder Cancer (SNRUBC) with information about tumour grade (according to WHO 1999) [5] in the research database BladderBaSe 2.0 were considered for inclusion. These inclusion years were selected as information on tumour size and tumour multiplicity was not registered prior to 2013. The SNRUBC also consists of data on primary management and a 5-year follow-up form assessing recurrence and progression at 5 years. In addition to the data from SNRUBC, information from the Patient Register, the Causes of Death register and additional healthcare and demographic registers until forms BladderBaSe 2.0 [6]. Excluding patients with primary carcinoma in situ (CIS), metastases, inadequate information about follow-up and primary treatment with cystectomy or radiotherapy, 2,407 patients with information about tumour size and number of tumours were categorized according to the European Association of Urology (EAU) 2021 prognostic model [7], of which 710 were IR when excluding 71 grade 3 (WHO 1999) tumours according to the IBCG criteria [3] (Supplementary figure 1 and Supplementary table 1). Patients were followed from date of diagnosis to date of recurrence according to the 5-year follow-up form in the SNRUBC, or death, or censored after 5 years from date of diagnosis at the timepoint of completion of the 5-year follow-up form. Categorical variables were reported as numbers and proportions. Age was reported as medians with interquartile ranges (IQR). We defined a composite event as the combination of recurrence and death to harmonize methodology with Soria et al. [2] and estimated the probability of not having the event, that is, RFS by Kaplan-Meier curves and compared differences by log-rank test. We performed a sensitivity analysis with recurrence and death related to bladder cancer as event, where patients were censored at date of death unrelated to bladder cancer (Supplementary figure 2). Probabilities of RFS were explored in sensitivity analyses including patients receiving (n = 152) (Supplementary figure 3 and Supplementary table 2) and not receiving adjuvant serial instillations (n = 558) (Supplementary table 3 and Supplementary figure 4). For all statistical analyses the R statistical package version 4.1.1 was used.
The Research Ethics Board at Uppsala University, Sweden approved this study (year of approval and diary number: 2015‐277, 2019‐03574, 2020‐05123, and 2022‐01747‐02).
Results
In 710 patients with primary IR NMIBC, 152 (21%) patients were treated with adjuvant serial instillations. Additional patient and treatment characteristics are shown in Table 1. According to the IBCG model, 329 (46%) and 381 (54%) patients were low-IR and intermediate-IR risk (patients with primary NMIBC cannot be categorized as high-IR). During median 4.2 (IQR: 1.1–5.0) years of follow-up, 128 low-risk IR and 139 intermediate-risk IR patients experienced recurrence and 18 low-risk IR and 21 intermediate-risk IR patients died. The difference in RFS was not statistically significant (p = 0.2) (Figure 1). Probabilities of recurrence or death at 1 and 3 years after diagnosis were 19% (95% Confidence Interval [CI]: 15–23) and 41% (95% CI: 35–46) in low-risk IR, versus 27% (95% CI: 22–31) and 45% (95% CI: 40–50) in patients with intermediate-risk IR. Using recurrence and death related to bladder cancer as event, no statistically significant differences were observed between low and intermediate IR primary NMIBC (Supplementary figure 2).
| Group | Low-IR n (%) | Intermediate-IR n (%) | Total n (%) | ||
| Number of patients | 329 | 381 | 710 | ||
| Median age [interquartile range] years | 71 [65–79] | 75 [69–81] | 73 [67–80] | ||
| Sex | |||||
| Female | 71 (10) | 100 (14) | 171 (24) | ||
| Male | 258 (36) | 281 (40) | 539 (76) | ||
| Tumour size | |||||
| <3 cm | 329 (46) | 193 (27) | 522 (74) | ||
| ≥3 cm | 0 (0) | 188 (26) | 188 (26) | ||
| Multiplicity | |||||
| Single | 329 (46) | 147 (21) | 476 (67) | ||
| Multiple | 0 (0) | 234 (33) | 234 (33) | ||
| Tumour stage | |||||
| Ta | 306 (43) | 378 (53) | 684 (96) | ||
| T1 | 23 (3) | 3 (0.4) | 26 (4) | ||
| Grade (WHO 1999) | |||||
| LMP | 0 (0) | 4 (0.6) | 4 (0.6) | ||
| G1 | 2 (0.3) | 146 (21) | 148 (21) | ||
| G2 | 327 (46) | 231 (33) | 558 (79) | ||
| Single postoperative instillation | 13 (2) | 25 (4) | 38 (6) | ||
| Adjuvant serial instillations* | 72 (10) | 80 (11) | 152 (21) | ||
| BCG | 34 (5) | 35 (5) | 69 (10) | ||
| Serial chemotherapy instillations | 38 (5) | 45 (6) | 83 (11) | ||
| WHO: World Health Organization; LMP: low malignant potential; BCG: Bacillus Calmette-Guérin. *One patient with missing information. | |||||
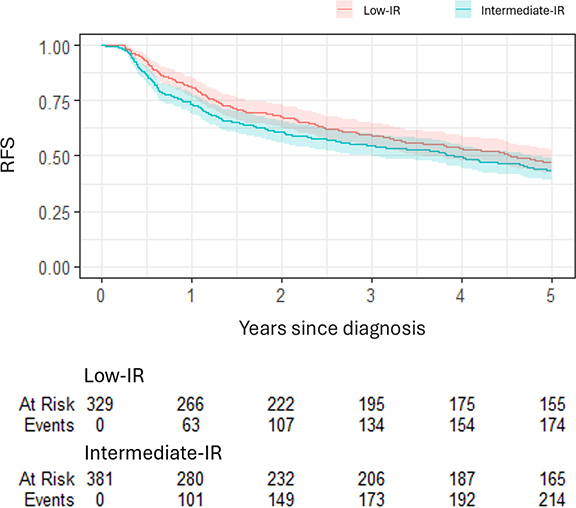
Figure 1. Recurrence-free survival (RFS) for all 710 patients with primary intermediate risk (IR) non-muscle invasive bladder cancer stratified in low- and intermediate-IR (log-rank test p = 0.2). Event is defined as recurrence or death as a composite endpoint.
In a sensitivity analysis comprising only patients receiving serial adjuvant instillations (Supplementary table 2), corresponding probabilities of recurrence or death at 1 and 3 years were 19% (95% CI: 10–28) and 33% (95% CI: 22–43%) versus 15% (95% CI: 7–23) and 31% (95% CI: 20–41), respectively (Supplementary figure 3).
Discussion
The IBCG prognostic model for IR NMIBC predicted similar RFS in low- and intermediate-risk primary IR NMIBC at 3 years after diagnosis and in patients with serial adjuvant instillations.
The five risk factors for recurrence suggested by the IBCG were based on a collaborative review of randomized clinical trials, systematic reviews and meta-analyses [1]. The current study population with primary IR NMIBC is likely more homogenous than patients in the previous validation study [2] and represents a real-life setting including patients from a variety of hospitals nation-wide. Regarding grade, this study applied the WHO 1999 grading system, as opposed to WHO 1973 or 2004/2022 systems used in previous studies [1, 2]. As the different grading systems have shown different recurrence-predictive capabilities, that is, the four-tier combination of WHO 1973 and 2004/2022 (a proxy for WHO1999) predicted recurrence [8], whereas WHO 1973 grading system did not [9]. Likely, the more precise definition of grade 2 by the WHO 1999 system compared to WHO 1973, suggests that IR tumours in this setting could be a more homogenous group, further contributing to similar RFS in the low- and intermediate-risk IR categories in this study.
Excluding patients with missing data on tumour size and tumour multiplicity could have influenced the generalizability of our results if these excluded patients inherently had a higher propensity to recur. Yet, we did not detect any large differences in patient characteristics among those with missing data and the main study population (Supplementary table 1). Another limitation is the low proportion of patients treated with serial adjuvant chemotherapy instillations, due to paucity of such practice in several hospitals in Sweden during the years of 2013 and 2014. Still, as the results did not change in the sensitivity analysis including only patients receiving adjuvant serial instillations, it is unlikely that this feature influenced the internal validity of the study. As a consequence of similar RFS in low- and intermediate-risk primary IR NMIBC, no formal assessment of calibration and discrimination of the IBCG prognostic model was undertaken.
Thus, prediction of recurrence based on only clinical factors in the IBCG model in primary IR NMIBC seems inadequate when applied in a larger cohort outside referral centers. In line with this, in the large cohort where the EAU 2021 prognostic model for progression was constructed, a model for prediction of RFS could not be identified [10]. Factors not measured in the IBCG model that could affect RFS include how well the TURB surgery is performed and biological characteristics such as the tumour’s molecular subtype and grade. Furthermore, a recent publication shows promising results for an artificial intelligence-based model for progression including patients with IR NMIBC [11].
In conclusion, this study does not support the use of the International Bladder Cancer Group prognostic model to predict recurrence-free survival in patients with primary intermediate risk non-muscle invasive bladder cancer. The International Bladder Cancer Group model seems to lack information for clinical decision-making in terms of a stratified use of adjuvant instillations (serial chemotherapy or Bacillus Calmette-Guérin) or intensity of follow-up [3].
Acknowledgements
None.
References
[1] Tan WS, Steinberg G, Witjes JA, et al. Intermediate-risk non-muscle-invasive bladder cancer: updated consensus definition and management recommendations from the International Bladder Cancer Group. Eur Urol Oncol. 2022;5(5):505–516. https://doi.org/10.1016/j.euo.2022.05.005
[2] Soria F, Rosazza M, Livoti S, et al. Clinical validation of the intermediate-risk non-muscle-invasive bladder cancer scoring system and substratification model proposed by the International Bladder Cancer Group: a multicenter young academic urologists urothelial working group collaboration. Eur Urol Oncol. 2024;7(6):1497–1503. https://doi.org/10.1016/j.euo.2024.06.004
[3] Li R, Hensley PJ, Babjuk M, et al. Intermediate-risk Non-muscle-invasive Bladder Cancer: Recommendations for Definitions, Risk Stratification, Management Strategies, and Clinical Trial Design from the International Bladder Cancer Group. Eur Urol Oncol. 2025;8(6):1685-1695. https://doi.org/10.1016/j.euo.2025.08.003
[4] Zaurito P, Scilipoti P, Longoni M, et al. The value of maintenance therapy in intermediate-risk non-muscle-invasive bladder cancer. BJU Int. 2026;137(1):201-208. https://doi.org/10.1111/bju.16905
[5] Busch C, Algaba F. The WHO/ISUP 1998 and WHO 1999 systems for malignancy grading of bladder cancer. Scientific foundation and translation to one another and previous systems. Virchows Arch. 2002;441(2):105-108. https://doi.org/10.1007/s00428-002-0633-x
[6] Häggström C, Hagberg O, Gårdmark T, et al. Cohort profile: Bladder Cancer Data Base Sweden (BladderBaSe) 2.0. BMJ Open. 2022;12(12):e064898. https://doi.org/10.1136/bmjopen-2022-064898
[7] Sylvester RJ, Rodríguez O, Hernández V, et al. European Association of Urology (EAU) prognostic factor risk groups for Non-muscle-invasive Bladder Cancer (NMIBC) incorporating the WHO 2004/2016 and WHO 1973 classification systems for grade: an update from the EAU NMIBC guidelines panel. Eur Urol. 2021;79(4):480–488. https://doi.org/10.1016/j.eururo.2020.12.033
[8] Contieri R, Martini A, Beijert IJ, et al. Towards defining follow-up strategies for patients with primary intermediate-risk non-muscle-invasive bladder cancer. Eur Urol Oncol. 2025;8(4):977–985. https://doi.org/10.1016/j.euo.2025.04.010
[9] Jahnson S, Jancke G, Olsson H, Aljabery F. Bladder cancer grading using the four-tier combination of the World Health Organization (WHO) 1973 and WHO 2004 classifications. BJU Int. 2023;132(6):656–663. https://doi.org/10.1111/bju.16100
[10] van Rhijn BWG, Hentschel AE, Bründl J, et al. Prognostic value of the WHO1973 and WHO2004/2016 classification systems for grade in primary Ta/T1 non-muscle-invasive bladder cancer: a Multicenter European Association of Urology non-muscle-invasive bladder cancer guidelines panel study. Eur Urol Oncol. 2021;4(2):182–191. https://doi.org/10.1016/j.euo.2020.12.002
[11] Kwong JCC, Al-Daqqaq Z, Chelliahpillai Y, et al. Development and International Evaluation of an Artificial Intelligence-based Model (PROGRxN-BCa) Using the World Health Organization 2004/2022 Grading System to Predict Progression Risk and Improve Substratification for Non-muscle-invasive Bladder Cancer. Eur Urol. Published online October 7, 2025. https://doi.org/10.1016/j.eururo.2025.09.4145