ORIGINAL RESEARCH ARTICLE
Histopathological assessment practices in adult male circumcision and detection of lichen sclerosus: a retrospective single-centre study
Jenny Engmana  , Wilma Håkanssona , Nirina Anderssona , Johan Svenssonb , Elisabet Nylandera , Amir Sherifc and Maja af Klinteberga
, Wilma Håkanssona , Nirina Anderssona , Johan Svenssonb , Elisabet Nylandera , Amir Sherifc and Maja af Klinteberga
aDepartment of Public Health and Clinical Medicine, Dermatology and Venerology, Umeå University, Umeå, Sweden; bDepartment of Statistics, Umeå School of Business, Economics and Statistics, Umeå University, Umeå, Sweden; cDepartment of Diagnostics and Intervention, Urology and Andrology, Umeå University, Umeå, Sweden
Abstract
Objective: To investigate histopathological assessment practices following medical circumcision, analyse the prevalence of lichen sclerosus (LS) and assess the management of circumcised LS patients.
Material and methods: This retrospective study was conducted at Umeå University Hospital. A total of 416 patients aged ≥18 years who underwent medical circumcision between 2016 and 2023 were included. The variables investigated were the frequency of histopathological diagnosis of preputial tissue, pre- and post-surgery treatment, further management and the prevalence of LS.
Results: The mean (standard deviation [SD]) age of included patients was 47 (21) years. Before circumcision, 34% (141/416) of the study population had received treatment with potent or ultrapotent topical corticosteroids. A pre-operative diagnosis of LS was set in 4.8% (20/416) of the patients. Histopathological analysis of circumcised material was performed in 44% (183/416) of cases. Amongst these, LS was confirmed in 60% (110/183). Amongst the patients with histologically confirmed LS, 13% (14/110) received a recorded diagnosis of LS. A total of 15% (16/110) of the patients with LS were either referred to a dermatovenereologist and/or received treatment with an ultrapotent topical corticosteroid.
Conclusions: LS appears to be both underdiagnosed and not adequately treated in patients undergoing medical circumcision. Less than half of the circumcised specimens were analysed, which means a risk of missing LS and potential dysplastic changes. Most patients with LS did not receive adequate diagnosis and treatment after surgery. Failure to diagnose LS limits patient awareness, follow-up and appropriate care, factors that may contribute to disease progression and increased cancer risk.
KEYWORDS: Lichen sclerosus; circumcision; histopathology; treatment; diagnosis; prevalence; prepuce; phimosis
Citation: Scandinavian Journal of Urology 2026, VOL. 61, 156–162. https://doi.org/10.2340/sju.v61.45886.
Copyright: © 2026 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 22 January 2026; Accepted: 23 March 2026; Published: 27 April 2026
CONTACT: Jenny Engman jenny.engman@umu.se Umeå University Hospital, 901 85 Umeå
Supplemental data for this article can be accessed online at https://doi.org/10.2340/sju.v61.45886
Competing interests and funding: The authors declare no conflicts of interest.
Introduction
Lichen sclerosus (LS) is a chronic inflammatory scarring dermatosis that mainly affects the anogenital region [1]. The disease is believed to be both underdiagnosed and not adequately treated since early stages can be non-specific, asymptomatic or not recognised neither by healthcare professionals nor by patients. The exact prevalence and incidence are unknown. LS affects both sexes, although the disease is more common in females [2]. A recent Swedish study investigating the incidence of LS based on registered diagnoses in the National Patient Register found the incidence of male LS to be 47.2 per 100,000 persons/year [3].
Typical symptoms in male patients include soreness, sometimes pruritus, phimosis, dyspareunia and voiding difficulties. Clinical signs are white sclerotic plaques, fissures, atrophic skin and erosions. Penile LS often involves the glans and the prepuce [1, 4, 5]. LS is one of the most common causes of acquired phimosis in adults [6]. Other complications are urethral strictures and meatal stenosis [7]. Moreover, LS is associated with an increased risk of developing squamous cell carcinoma [8], with studies reporting a malignancy risk of 1.3–13.6% [8–11].
The diagnosis of LS can be made clinically, although a punch biopsy at baseline is valuable and should always be performed, especially if the diagnosis is uncertain or dysplasia is suspected [7]. Providing patients with information about a correct diagnosis is essential for promoting disease awareness, highlighting potential risks and emphasising the significance of self-examination [7]. The gold standard treatment for LS is potent or ultrapotent topical corticosteroids, which are effective in early and intermediate stages of the disease [12]. If corticosteroids are insufficient or if there are difficulties applying topical treatment due to phimosis, circumcision may be required. Circumcision may be curative, but long-term studies are lacking [12]. In cases of acquired phimosis, it is recommended to analyse all circumcised tissue because histopathological diagnosis has higher accuracy and specificity than a clinical diagnosis [5, 12–14]. However, histopathology is not performed routinely [15]. Pre- and post-circumcision, it is recommended to treat LS patients with potent or ultrapotent topical corticosteroids, and the disease should be reviewed post-operatively [5, 12].
This retrospective study aimed to: (1) quantify histopathological submission frequency and detection of LS in circumcised specimens, (2) identify predictors of submission for histopathological analysis and (3) post-operative care of LS patients, including diagnosis, treatment and referral routines.
Materials and methods
Study design and population
This retrospective, single-centre study was based on data obtained from medical records at Umeå University Hospital. Inclusion criteria were male sex, 18 years of age or older and having undergone a medical circumcision, with a clinical indication at the Urology Department between 1st January 2016 and 31st December 2023. A total of 458 patients were circumcised during this period. Eleven patients were excluded due to, for example, unknown addresses without the possibility of receiving study information or medical charts marked as confidential. After receiving a letter with written information, 31 patients opted out, resulting in a total of 416 patients included in the study. The flowchart of participant inclusion is presented in Figure 1.
Figure 1. Flowchart of participant inclusion.
Data collection
Eligible patients were found using the procedure code for circumcision (KGV20). Data were collected according to a predefined list of variables, including age, pre- and post-operative diagnosis, medication, genital symptoms and their duration, topical treatment pre- and post-circumcision, previous surgical treatment, genital complaints in childhood, genital status, histopathological analysis and post-operative referral. The severity of phimosis was based on a grading system by Meuli et al. [16], with four categories (grades 1–4). In grade 1, the prepuce can be retracted fully, with a constrictive ring around the shaft; in grade 4, the prepuce cannot be retracted at all. When the exact grade was not documented, severity was estimated based on the description of genital status. Participants were stratified into groups to compare outcomes: phimosis was categorised as severe phimosis (grades 3–4) versus none or mild phimosis (grades 1–2). Additionally, circumcisions performed more recently, between 2020 and 2023, were compared with those conducted between 2016 and 2019, with the theory that histopathological analysis was used to a larger extent in more recent years. An age cut-off of 50 years was selected to compare outcomes in younger versus older participants. At the Urology Department, during the study period, there were no local established routines regarding the submission of histopathological analysis or post-operative care regarding LS.
Ethics
This study was ethically approved by the Swedish Ethical Review Authority (Dnr 2024-03331-01) and conducted according to the ethical principles of the Declaration of Helsinki. The included patients received written information about the study, including the option to opt out. All data were pseudonymised and presented at a group level.
Statistics
Descriptive analyses were used to summarise the data, and categorical variables were presented as absolute numbers (n) and relative frequencies (%). Student’s t-test was used to compare means. Associations between categorical variables were assessed using the Chi-square test. A significance level of 5% was used. Unadjusted and adjusted logistic regression analyses were performed to identify factors associated with histopathological analysis of the prepuce and clinical signs associated with an LS diagnosis histopathologically, expressed as odds ratio (OR) with a 95% confidence interval (CI). Included variables in the regression analysis were selected based on clinical relevance and previous literature. They comprised synechiae, atypical skin lesions, white lesions, red lesions, fissures, severe phimosis, more recent circumcision and age ≥ 50. There were no missing data for variables related to histopathological analysis, current pharmacological treatment or recorded clinical diagnoses. If documentation regarding findings from clinical examination or previous treatment was missing in the medical records, this was interpreted as absence of the finding or treatment, since such information is routinely recorded when present in clinical practice. For variables related to symptoms, documentation could be more variable, and results should therefore be interpreted as reported symptoms rather than definitive presence or absence. Data were analysed using IBM SPSS Statistics.
Results
The mean (standard deviation [SD]) age was 47 (21) years. The majority reported genital symptoms lasting more than 1 year (Table 1). The most frequently reported symptoms were negative impact on sexual life (62%, 257/416), dyspareunia (60%, 250/416) and genital soreness/pain (59%, 244/416), as listed in Table 1. The vast majority had phimosis (97%, 405/416). Other common clinical signs are presented in Table 1.
| Characteristics | Specimens submitted for histopathological analysis | |||
| Yes n (%) |
No n (%) |
Total n (%) |
||
| Age ≥ 50 | 110 (60) | 75 (32) | 185 (45) | |
| Circumcision between 2020 and 2023 | 117 (64) | 122 (52) | 239 (58) | |
| Reported duration of symptoms | ≤ 1 year | 32 (19) | 29 (15) | 61 (17) |
| 1–10 years | 85 (52) | 94 (48) | 179 (49) | |
| ≥ 10 years | 27 (16) | 20 (10) | 47 (13) | |
| Always/since childhood | 21 (13) | 54 (27) | 75 (21) | |
| Missing | 18 | 36 | 54 | |
| Symptoms reported | Negative effect on sex life | 102 (56) | 155 (67) | 257 (62) |
| Dyspareunia | 100 (55) | 150 (64) | 250 (60) | |
| Genital soreness/pain | 114 (62) | 130 (56) | 244 (59) | |
| Erectile dysfunction | 22 (12) | 24 (10) | 46 (11) | |
| Itch | 12 (6.6) | 11 (4.7) | 23 (5.5) | |
| Urinary problems | 14 (7.7) | 10 (4.3) | 24 (5.8) | |
| Bleeding | 8 (4.4) | 10 (4.3) | 18 (4.3) | |
| Clinical signs | Phimosis | 174 (95) | 231 (99) | 405 (97) |
| Fissures | 89 (49) | 88 (38) | 177 (43) | |
| White lesions | 98 (54) | 61 (26) | 159 (38) | |
| Red lesions | 55 (30) | 43 (19) | 98 (24) | |
| Synechiae | 26 (14) | 22 (9.4) | 48 (12) | |
| Atypical skin lesions* | 19 (10) | 6 (2.6) | 25 (6.0) | |
| Severe phimosis** | 97 (53) | 88 (38) | 185 (45) | |
| Current medication | Anti-hypertensive | 92 (50) | 73 (31) | 165 (40) |
| Hypolipidemic | 65 (36) | 48 (21) | 113 (27) | |
| Antidiabetics | 44 (24) | 38 (16) | 82 (20) | |
| Psychopharmaceuticals | 42 (23) | 63 (27) | 105 (25) | |
| Anticoagulants | 38 (21) | 37 (16) | 75 (18) | |
| Inhalations | 20 (11) | 33 (14) | 53 (13) | |
| Thyroid hormone supplement | 9 (5) | 4 (1.7) | 13 (3.1) | |
| Previous topical treatment of genital symptoms in adulthood | Any previous topical corticosteroid treatment*** | 79 (43) | 94 (40) | 173 (42) |
| Mild or moderate topical corticosteroid | 16 (8.7) | 21 (9.0) | 37 (8.9) | |
| Potent or ultrapotent topical corticosteroid | 64 (35) | 77 (33) | 141 (34) | |
| Unknown topical corticosteroid | 2 (1.1) | 3 (1.3) | 5 (1.2) | |
| Previous surgical treatment of genital symptoms in adulthood | Any surgical treatment | 19 (10) | 32 (14) | 51 (12) |
| Frenuloplasty | 6 (3.3) | 15 (6.4) | 21 (5.0) | |
| Dosal slit | 6 (3.3) | 9 (3.9) | 15 (3.6) | |
| Circumcision | 5 (2.7) | 3 (1.3) | 8 (1.9) | |
| Adhesiotomy | 0 (0) | 2 (0.86) | 2 (0.48) | |
| Manual repositioning | 1 (0.55) | 2 (0.86) | 3 (0.72) | |
| Other**** | 5 (2.7) | 3 (1.3) | 8 (1.9) | |
| Patients circumcised at Umeå University hospital during the years 2016–2023 (divided in: submitted for histopathological analysis (yes) n = 183, not submitted (no) n = 233 and total n = 416). Note: patients could have more than one treatment. *Atypical skin lesion, including ulcers. **Severe phimosis, grade 3 or 4, according to Meuli [16]. ***Any previous topical corticosteroid treatment including combination with antifungal. ****Other: including the nesbit procedure, urethral dilatation, glansectomy, penile abscess drainage and unspecified preputioplasty. |
||||
Pre-operative topical corticosteroid treatment for genital symptoms was prescribed to 42% (173/416), with potent or ultrapotent topical corticosteroids most frequently used (34%, 141/416) (Table 1). Amongst those with previous surgical treatment (12%, 51/416), frenuloplasty was the most common procedure (5.0%, 21/416) used (Table 1).
The most common clinical diagnosis documented before circumcision was phimosis (92%, 383/416), followed by LS (4.8%, 20/416). Other diagnoses before circumcision are listed in Table 2. Genital symptoms in childhood were reported by 29% (121/416).
| Clinical diagnosis before circumcision | n (%) |
| Phimosis | 383 (92) |
| Lichen sclerosus | 20 (4.8) |
| Frenulum breve | 8 (1.9) |
| Paraphimosis | 5 (1.2) |
| Tumour of clinical unknown nature | 4 (0.96) |
| Penile cancer/suspected penile cancer | 4 (0.96) |
| Penile intraepithelial neoplasia | 3 (0.72) |
| Atypical skin lesion | 2 (0.48) |
| Balanitis | 2 (0.48) |
| Cancer in the urinary tract | 2 (0.48) |
| Surplus of prepuce | 2 (0.48) |
| Plasma cell balanitis | 2 (0.48) |
| Meatal stenosis | 1 (0.24) |
| Prostate cancer | 1 (0.24) |
| Adhesion of prepuce | 1 (0.24) |
| Histopathological diagnosis after circumcision | n (%) |
| Lichen sclerosus | 110 (60) |
| Non-specified inflammation and fibrosis | 46 (25) |
| PeIN | 10 (5.5) |
| Penile cancer | 4 (2.2) |
| Normal/non-atypical | 4 (2.2) |
| Lichen planus | 4 (2.2) |
| Non-specified lichenoid inflammation | 3 (1.6) |
| Other* | 5 (2.7) |
| Note: patients and specimens could have more than one diagnosis. *Other: includes condyloma and benign sebaceous gland hyperplasia. | |
Histopathological analysis was performed on 44% (183/416) of all circumcised prepuces. The most common histopathological diagnosis was LS (60%, 110/183), Table 2. Of these, 86% (95/110) did not have a documented clinical LS diagnosis prior to circumcision. Other histopathological diagnoses are listed in Table 2.
Factors associated with histopathological analysis of the prepuce were investigated using unadjusted and adjusted logistic regression analysis (Figure 2). White lesions, atypical skin lesions (including ulcers), fissures, age ≥ 50 years, severe phimosis (grades 3–4) and circumcision performed in more recent years (2020–2023) were factors significantly associated with histopathological analysis. Factors with the highest impact were atypical skin lesions (OR: 5.16, 95% CI: 1.87–14.26), white lesions (OR: 2.97, 95% CI: 1.89–4.66) and age ≥ 50 years (OR: 2.83, 95% CI: 1.77–4.52) (see Figure 2 and Supplementary Table S1). A second adjusted and unadjusted logistic regression model investigated associations between clinical signs and a histopathologically confirmed LS diagnosis (Table 3). The presence of white lesions was a significant factor associated with a histopathological LS diagnosis in the unadjusted and adjusted logistic regression analysis. Fissures and severe phimosis were clinical signs associated with a histopathological LS diagnosis in the unadjusted analysis. Atypical skin lesions and red lesions were signs associated with a decreased risk of receiving a histopathological LS diagnosis.
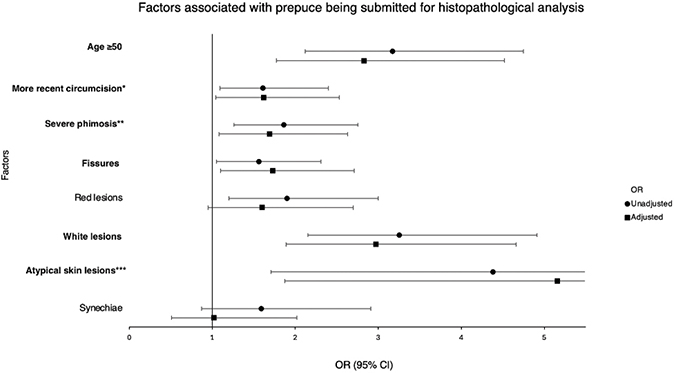
Figure 2. Factors associated with the submission of circumcised prepuce for histopathological analysis. Results from unadjusted and adjusted logistic regression presented as odds ratios (OR) with 95% confidence interval (CI).
Significantly associated factors are in bold. *More recent circumcision (2020–2023). **Severe phimosis, grade 3 and 4, according to Meuli [16]. ***Atypical skin lesions, including ulcers.
| Clinical signs | Unadjusted | Adjusted | ||
| OR (95% CI) | Sig. | OR (95% CI) | Sig. | |
| Synechiae | 1.59 (0.65–3.88) | 0.305 | 1.40 (0.47–4.18) | 0.544 |
| Atypical skin lesions* | 0.27 (0.10–0.74) | 0.007 | 0.24 (0.07–0.79) | 0.020 |
| White lesions | 5.18 (2.72–9.86) | < 0.001 | 4.90 (2.42–9.92) | < 0.001 |
| Red lesions | 0.27 (0.14–0.52) | < 0.001 | 0.27 (0.13–0.60) | 0.001 |
| Fissures | 2.00 (1.09–3.66) | 0.023 | 1.60 (0.79–3.21) | 0.189 |
| Severe phimosis** | 2.03 (1.11–3.71) | 0.020 | 1.85 (0.92–3.71) | 0.085 |
| Age ≥ 50 | 1.31 (0.72–2.40) | 0.375 | 1.82 (0.86–2.87) | 0.120 |
| Significantly associated factors with receiving a histopathological lichen sclerosus diagnosis are in bold. *Atypical skin lesions, including ulcers. **Severe phimosis, grade 3 and 4, according to Meuli [16]. | ||||
In patients with phimosis, a higher mean phimosis severity score was observed amongst prepuces submitted for histopathological analysis (2.7 vs. 2.2, p = 0.001). The mean age of patients was higher (54 vs. 42 years, p < 0.001) amongst those who had their prepuce submitted. Patients with a clinical LS diagnosis prior to circumcision were more likely to have their excised tissue submitted for histopathological analysis compared to individuals without an LS diagnosis (75% vs. 42%, p = 0.004). The proportion of specimens analysed histopathologically was significantly higher in 2020–2023 (49%) than in 2016–2019 (39%) (p = 0.018).
Amongst the 110 patients who received a histopathological diagnosis of LS, 13% (14/110) had a documented LS diagnosis in their medical records post-circumcision. Of these, 9.1% (10/110) received treatment with an ultrapotent topical corticosteroid (no other topical treatment was prescribed), and 11% (12/110) obtained referral to a dermatovenereologist (6 persons were both treated with ultrapotent topical corticosteroids and referred to the Department of Dermatology and Venereology post-operatively). In total, 15% (16/110) of the patients with LS were either referred to a dermatovenereologist and/or received treatment with an ultrapotent topical corticosteroid.
Discussion
This retrospective study of patients undergoing medical circumcision demonstrates that the majority, 56%, did not have their prepuce submitted for histopathological analysis. Amongst the analysed prepuces, the most common diagnosis was LS (60%). Most patients with a histopathological LS diagnosis neither had a documented diagnosis in their medical records nor received appropriate treatment or follow-up after circumcision.
The European guidelines on LS recommend submitting all circumcised materials for histopathological analysis to confirm the diagnosis and exclude neoplastic changes [5, 12]. In the present study, only 4.8% had an LS diagnosis before circumcision, whereas 60% of the prepuces analysed were histopathologically diagnosed as LS. Amongst all circumcised men, 110 cases of LS were identified. As histopathological examination was performed selectively, this proportion should not be interpreted as an unbiased prevalence estimate. The true prevalence of LS in the cohort cannot be determined and is probably underestimated. These results highlight the importance of submitting all medically circumcised prepuces for histopathological evaluation to avoid missing an LS diagnosis and, in extension, dysplastic changes. It is important to provide patients with information about the disease and treatment, the increased risk of developing penile squamous cell carcinoma and urethral strictures, as well as instructions on self-examination [8, 17].
Histopathological diagnosis has a higher specificity than clinical diagnosis in detecting LS in circumcised patients [14, 18, 19]. Our findings are consistent with those of previous studies. A previous Swedish study showed that the vast majority had the clinical diagnosis ‘phimosis’, whereas after histopathological analysis, 59% had an LS diagnosis [14]. Even when the phimotic prepuce is carefully examined by a dermatovenereologist or a urologist before circumcision, histopathology has a higher diagnostic accuracy in diagnosing LS [18]. These findings highlight the importance of routinely submitting excised specimens for histopathological examination [12, 14, 20].
The prevalence of LS in histopathologically analysed circumcised prepuce was similar in our study compared to previous studies, ranging between 55% and 68% [14, 18, 21]. LS is considered an underdiagnosed disease, with an unknown true prevalence [2]. An important factor can be the lack of histopathological analysis following circumcision, and another can be insufficient documentation of the diagnosis in the medical records. The lack of documentation can affect the credibility of estimated incidence in registry-based studies based on documented diagnoses in medical records. This is supported by our finding that only 13% of histologically verified LS cases were coded in the medical records post-operatively, suggesting substantial underreporting in registry-based data.
It is crucial to receive a correct LS diagnosis since the disease is associated with a substantially increased risk of penile squamous cell carcinoma, reported to be up to 16-fold higher compared to unaffected men, and the risk increases over time [11]. It is important to be informed about self-examination for cellular changes and detection of inflammatory activity that can be treated [7, 12]. In addition to malignant transformation and active inflammation, LS may lead to progressive scarring and complex urethral strictures, underscoring the importance of early and accurate diagnosis to enable appropriate treatment and prevent long-term complications [7].
In addition to being underdiagnosed, LS is also believed to be undertreated [22]. According to our data, only 34% of the patients included had received treatment with potent or ultrapotent topical corticosteroids prior to circumcision, which is the gold standard treatment of LS. Topical treatment of LS can be effective in early and intermediate stages, whilst delayed treatment may lead to irreversibly altered genital anatomy [12]. The effectiveness of medical topical treatment in male LS varies between 50% and 60% in different studies [9, 23]. Correct medical treatment can also reduce the risk for malignant transformation and scarring [9, 24]. Knowing this, we emphasise that it is of great importance for patients with LS to receive correct medical treatment prior to circumcision, with the possibility of preventing surgery. However, males with LS have a delay in seeking medical care by up to 1.6 years [4], which risks worsening genital symptoms and reducing treatment efficacy.
The effectiveness of circumcision in treating LS varies between studies, with different endpoints, ranging between 36 and 100% [12, 23, 25, 26]; however, long-term studies are lacking [12]. The use of potent or ultrapotent topical corticosteroids is recommended both pre- and post-circumcision in patients with LS, starting 4 weeks prior to surgery and for at least 4–12 weeks post-operatively and longer based on individual assessment [12, 24]. According to our data, only 15% of patients with a histopathological LS diagnosis were either continuously medically treated and/or referred to a dermatovenereologist for follow-up, indicating severe undertreatment relative to established guidelines recommendations. It is recommended to review LS activity post-circumcision, and disease activity should be treated to reduce the risk of malignant transformation [5, 24, 27].
To the best of our knowledge, there are no previous studies on the frequency of preputial specimen submission for histopathological examination in Sweden, nor on clinical features increasing the likelihood of histopathological analysis. White lesions, atypical skin lesions, fissures, severe phimosis, older age and circumcision performed more recently were factors that made urologists more prone to submit circumcised material for histopathological analysis. Atypical skin lesions, which included ulcers, could be a clinical sign of cellular changes such as suspected penile intraepithelial neoplasia (PeIN) [28]. The mean age of patients whose prepuce was analysed was higher, which may reflect increased suspicion of dysplasia in elderly [29]. Kristiansen et al. demonstrated that PeIN was discovered in 2% of circumcised patients with symptomatic prepuce without clinical suspicion [14]. White lesions and fissures might be submitted to confirm an LS diagnosis [18]. Also, patients with a previous LS diagnosis more often had their specimens histopathologically analysed. Prepuce material was analysed to a larger extent during more recent years (2020–2023), possibly reflecting increased clinician awareness or an increasing incidence of LS, as demonstrated by Hieta et al. [30]. In addition, a more severe phimosis was more likely to be submitted for analysis. One possible explanation could be that in cases of severe phimosis, the prepuce cannot be fully clinically examined.
In the adjusted logistic regression analysis, white lesions were the only clinical sign independently associated with histopathologically confirmed LS, whilst fissures and severe phimosis were also associated in the unadjusted model. However, given that LS may be present even in the absence of these findings, these results support a low threshold for histopathological examination of all medically circumcised prepuce to ensure accurate diagnosis and correct treatment.
The present study has both strengths and limitations. A significant strength of this study is a large population of 416 patients, with a variety of symptoms and ages. This study provides a comprehensive overview of real-world clinical practice over an 8-year period, at a single centre. However, it has some limitations as well. First, the study solely relies on data from a single centre and because of its retrospective design selection bias cannot be excluded. Second, the absence of documentation was interpreted as the absence of the finding and may lead to misclassification bias. However, in routine clinical practice, positive findings are usually documented, whereas the absence of findings is not consistently recorded. This assumption is likely valid for routinely recorded clinical findings, but it may be less reliable for patient history variables, which could be more variably documented. The true presence of the described symptoms is likely higher than the prevalence reported in the medical records. The grading of phimosis was rarely documented in the exact grade; instead, it was based on descriptions in the medical records, which may result in an observational bias. Although our study is only performed in a single centre, previous studies have similar results to ours, which increases the generalisability [14, 20]. A prospective study where all the prepuces are submitted for histopathological analysis and where the participants are followed post-circumcision would be useful to calculate the prevalence of LS amongst circumcised patients and the need for treatment and follow-up post-circumcision.
In conclusion, according to our study, the clinical diagnosis may substantially underestimate the actual prevalence of LS in males undergoing medical circumcision. Routine histopathological analysis of circumcised preputial tissue demonstrates higher diagnostic sensitivity and can drastically improve case detection. There is also a lack of documentation and follow-up regarding circumcised patients with LS. Failure to diagnose LS limits patient awareness and appropriate care, factors that contribute to disease progression and increased risk of dysplastic changes. Our findings highlight the importance of diagnosing LS, routinely submitting circumcised tissue for histopathological analysis and ensuring appropriate management when LS is identified.
Acknowledgements
The authors thank the patients who participated in the study.
Financial support was received from the Medical Faculty, Umeå University and ALF – a regional agreement between Umeå University and Västerbotten County Council (grant number Bas-ALF/VLL RV-1014239). None of the funders was involved in the study design, data collection, data analysis or manuscript preparation.
References
- [1] Powell JJ, Wojnarowska F. Lichen sclerosus. Lancet. 1999;353(9166): 1777–1783. https://doi.org/10.1016/S0140-6736(98)08228-2
- [2] De Luca DA, Papara C, Vorobyev A, et al. Lichen sclerosus: the 2023 update. Front Med (Lausanne). 2023;10:1106318. https://doi.org/10.3389/fmed.2023.1106318
- [3] Jerkovic Gulin S, Lundin F, Eriksson O, et al. Lichen sclerosus-incidence and comorbidity: a nationwide Swedish Register Study. J Clin Med. 2024;13(10):2761. https://doi.org/10.3390/jcm13102761
- [4] Kantere D, Löwhagen GB, Alvengren G, et al. The clinical spectrum of lichen sclerosus in male patients – a retrospective study. Acta Derm Venereol. 2014;94(5):542–546. https://doi.org/10.2340/00015555-1797
- [5] Lewis FM, Tatnall FM, Velangi SS, et al. British Association of Dermatologists guidelines for the management of lichen sclerosus, 2018. Br J Dermatol. 2018;178(4):839–853. https://doi.org/10.1111/bjd.16241
- [6] Bighetti S, Mancon S, Suardi N, et al. Evaluating lichen sclerosus in phimosis: insights from a multidisciplinary retrospective study. Australas J Dermatol. 2025;66(2):e39–e42. https://doi.org/10.1111/ajd.14417
- [7] Kirtschig G, Kinberger M, Kreuter A, et al. EuroGuiderm guideline on lichen sclerosus-introduction into lichen sclerosus. J Eur Acad Dermatol Venereol. 2024;38(10):1850–1873. https://doi.org/10.1111/jdv.20082
- [8] Fergus KB, Lee AW, Baradaran N, et al. Pathophysiology, clinical manifestations, and treatment of lichen sclerosus: a systematic review. Urology. 2020;135:11–19.
- [9] Kravvas G, Shim TN, Doiron PR, et al. The diagnosis and management of male genital lichen sclerosus: a retrospective review of 301 patients. J Eur Acad Dermatol Venereol. 2018;32(1):91–95. https://doi.org/10.1111/jdv.14488
- [10] Ranjan N, Singh SK. Malignant transformation of penile lichen sclerosus: exactly how common is it? Int J Dermatol. 2008;47(12): 1308–1309. https://doi.org/10.1111/j.1365-4632.2008.03866.x
- [11] Stærk MG, Kaderly Rasmussen EL, Hannibal CG, et al. Histologically verified penile lichen sclerosus-Incidence in Denmark over 26 years and long-term risk of penile and non-penile cancer. Int J Cancer. 2025;157(6):1086–1093. https://doi.org/10.1002/ijc.35454
- [12] Kirtschig G, Kinberger M, Kreuter A, et al. EuroGuiderm guideline on lichen sclerosus – treatment of lichen sclerosus. J Eur Acad Dermatol Venereol. 2024;38(10):1874–1909. https://doi.org/10.1111/jdv.20083
- [13] Li J, Deng C, Peng Q. Underestimation of genital lichen sclerosus incidence in boys with phimosis: results from a systematic review. Pediatr Surg Int. 2018;34(11):1245–1250. https://doi.org/10.1007/s00383-018-4357-7
- [14] Kristiansen S, Bjartling C, Svensson Å, et al. Penile intraepithelial neoplasia, penile cancer precursors and human papillomavirus prevalence in symptomatic preputium: a cross-sectional study of 351 circumcised men in Sweden. BJU Int. 2021;127(4):428–434. https://doi.org/10.1111/bju.15221
- [15] Bochove-Overgaauw DM, Gelders W, De Vylder AM. Routine biopsies in pediatric circumcision: (non) sense? J Pediatr Urol. 2009;5(3): 178–180. https://doi.org/10.1016/j.jpurol.2008.11.008
- [16] Meuli M, Briner J, Hanimann B, et al. Lichen sclerosus et atrophicus causing phimosis in boys: a prospective study with 5-year followup after complete circumcision. J Urol. 1994;152(3):987–989. https://doi.org/10.1016/S0022-5347(17)32638-1
- [17] Leeson C, Vigil H, Witherspoon L. Foreskin care: hygiene, importance of counselling, and management of common complications. Can Fam Physician. 2025;71(2):97–102. https://doi.org/10.46747/cfp.710297
- [18] Czajkowski M, Żawrocki A, Czajkowska K, et al. Lichen sclerosus and phimosis – discrepancies between clinical and pathological diagnosis and its consequences. Urology. 2021;148:274–279. https://doi.org/10.1016/j.urology.2020.11.027
- [19] Kato T, Mizuno K, Nishio H, et al. Can lichen sclerosus be diagnosed by preputial appearance or symptoms? Res Rep Urol. 2018;10:89–94. https://doi.org/10.2147/RRU.S173184
- [20] Kwok M, Shugg N, Siriwardana A, et al. Prevalence and sequelae of penile lichen sclerosus in males presenting for circumcision in regional Australia: a multicentre retrospective cohort study. Transl Androl Urol. 2022;11(6):780–785. https://doi.org/10.21037/tau-22-29
- [21] Mazzoni D, Pool L, Muir J. Pathologically oriented descriptive study of male genital circumcisions across medical and surgical specialties. Int J Dermatol. 2021;60(5):559–563. https://doi.org/10.1111/ijd.15359
- [22] Kirtschig G. Lichen sclerosus-presentation, diagnosis and management. Dtsch Arztebl Int. 2016;113(19):337–343. https://doi.org/10.3238/arztebl.2016.0337
- [23] Edmonds EV, Hunt S, Hawkins D, et al. Clinical parameters in male genital lichen sclerosus: a case series of 329 patients. J Eur Acad Dermatol Venereol. 2012;26(6):730–737. https://doi.org/10.1111/j.1468-3083.2011.04155.x
- [24] Lee A, Bradford J, Fischer G. Long-term management of adult vulvar lichen sclerosus: a prospective cohort study of 507 women. JAMA Dermatol. 2015;151(10):1061–1067. https://doi.org/10.1001/jamadermatol.2015.0643
- [25] Kulkarni S, Barbagli G, Kirpekar D, et al. Lichen sclerosus of the male genitalia and urethra: surgical options and results in a multicenter international experience with 215 patients. Eur Urol. 2009;55(4):945–954. https://doi.org/10.1016/j.eururo.2008.07.046
- [26] Kantere D, Alvergren G, Gillstedt M, et al. Clinical features, complications and autoimmunity in male lichen sclerosus. Acta Derm Venereol. 2017;97(3):365–369. https://doi.org/10.2340/00015555-2537
- [27] Charlton OA, Smith SD. Balanitis xerotica obliterans: a review of diagnosis and management. Int J Dermatol. 2019;58(7):777–781. https://doi.org/10.1111/ijd.14236
- [28] Engelsgjerd JS, Leslie SW, LaGrange CA. Penile cancer and penile intraepithelial neoplasia. Treasure Island, FL: StatPearls Publishing Copyright © 2025, StatPearls Publishing LLC.; 2025.
- [29] Thumma N, Pitla N, Gorantla V, et al. A comprehensive review of current knowledge on penile squamous cell carcinoma. Front Oncol. 2024;14:1375882. https://doi.org/10.3389/fonc.2024.1375882
- [30] Hieta NK, Haataja MAM, Tapana L. Comorbidities in male patients with lichen sclerosus: a case-control study. J Low Genit Tract Dis. 2023;27(4):378–383. https://doi.org/10.1097/LGT.0000000000000769