LETTER TO THE EDITOR
Sweden’s nationwide transition to transperineal prostate biopsy: implications for implementation across Europe
Matthias Maya, Christian Gilfricha, Uwe-Bernd Liehrb and Steffen Lebentraub,c
aDepartment of Urology, St. Elisabeth Hospital Straubing, Medical Campus Lower Bavaria (MCN), Straubing, Germany; bDepartment of Urology, Urooncology, Robot-Assisted and Focal Therapy, University Hospital Magdeburg, Otto-von Guericke University Magdeburg, Magdeburg, Germany; cDepartment of Urology, Werner Forssmann Hospital, Eberswalde, Germany
KEYWORDS: transrectal route; infectious morbidity; antibiotic prophylaxis; antimicrobial stewardship; hospital readmission; registry cohort
Citation: Scandinavian Journal of Urology 2026, VOL. 61, 163–165. https://doi.org/10.2340/sju.v61.45984.
Copyright: © 2026 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 25 March 2026; Accepted: 10 April 2026; Published: 6 May 2026
CONTACT: Prof. Dr. Matthias May, matthias.may@klinikum-straubing.de Department of Urology, St. Elisabeth Hospital Straubing, Medical Campus Lower Bavaria (MCN), Straubing, Germany
Competing interests and funding: The authors declare no conflict of interest.
No funding was received for this work.
We read with great interest the nationwide Swedish cohort study by Bonnedahl et al. on infectious outcomes after transperineal (TP) versus transrectal (TR) prostate biopsy in 31,222 men diagnosed with prostate cancer between 2020 and 2023 [1]. They provide timely, clinically relevant real-world data from a national registry at a moment when biopsy route, post-biopsy infection and antimicrobial stewardship have become closely intertwined in contemporary prostate cancer diagnostics. Their principal finding is both clear and clinically important: hospital admission after biopsy occurred less often after TP than after TR biopsy, and urinary tract-related antibiotic prescriptions were likewise less frequent after TP biopsy [1].
Beyond comparative safety, the Swedish cohort also captures a pronounced real-world implementation shift: the annual proportion of TP biopsy among all recorded prostate biopsies rose from 3.3 in 2020 to 7.2% in 2021, 12.2 in 2022 and 26.3% in 2023, representing an almost eightfold increase over 4 years [1]. This is highly relevant because it reflects not only a difference in procedural outcomes but also a broader process of implementation. Put differently, the Swedish data document both a safer contemporary pathway and a health system actively moving towards it. That dual message deserves particular emphasis because it links outcome advantage to observable health-system adoption. It is also consistent with current European guidance, which increasingly positions TP biopsy as the preferred route and recognises that, in patients at low infectious risk, routine antibiotic prophylaxis may not be required in the TP setting [2, 3].
At the same time, the Swedish cohort should be interpreted as a route-comparative real-world implementation study rather than a controlled comparison of standardised infection-prevention pathways. In addition to the lack of granular data on administered prophylaxis and incomplete uptake of rectal povidone-iodine preparation during the study period, the analysis was restricted to men with biopsy-detected prostate cancer and spanned a period of rapid national transition from transrectal to transperineal practice, leaving room for residual confounding despite adjustment [1]. This nuance does not diminish the central clinical message. Rather, it sharpens an important practical distinction: a pathway that relies on increasingly complex antimicrobial strategies and rectal antisepsis to remain acceptable is structurally different from one that bypasses contaminated rectal mucosa altogether. That distinction is also supported by the contemporary evidence base. In a systematic review and meta-analysis of 10 randomised trials comprising 4188 biopsies, Stangl et al. found that TP biopsy was associated with markedly lower odds of infection-related hospital admission than TR biopsy (odds ratio [OR] 0.23, 95% confidence interval [CI] 0.10–0.54) and a significantly lower rate of post-biopsy fever (OR 0.68, 95% CI 0.52–0.89), while no significant difference in sepsis was observed [4]. By contrast, our systematic review addressed the complementary question within the TP pathway itself and found, across 23 comparative studies including 12,324 men, that periprocedural antibiotic prophylaxis did not significantly reduce genitourinary infections (0.50 vs 0.37%; OR 1.37, 95% CI 0.74–2.54), sepsis (0.16 vs 0.13%; OR 1.30, 95% CI 0.46–3.67) or infection-related readmission (0.35 vs 0.29%; OR 1.45, 95% CI 0.70–3.03) [5]. Taken together, these data shift the debate away from route comparison alone and towards pathway design, namely which biopsy strategy achieves the lowest infectious burden with the least antibiotic exposure.
For this reason, the study by Bonnedahl et al. should also be read in a broader implementation context. As illustrated in Figure 1, a parallel shift is also visible in German Diagnosis Related Groups (DRG)-based inpatient administrative data, where the annual share of TP biopsy rose from 8.2 in 2020 to 58.3% in 2024, with the underlying absolute inpatient case numbers shown below the panels [6]. These trajectories are not directly comparable at the national level, because the Swedish data derive from a nationwide registry-based cohort, whereas the German data are restricted to inpatient DRG-coded procedures and do not capture outpatient biopsies, which may underestimate the continuing contribution of the TR route to overall German practice [1, 6]. Even with that caveat, the convergent directional shift across two distinct data environments suggests that the transition towards TP biopsy is no longer confined to selected expert centers but is becoming visible at the health-system level. Contemporary registry data, randomised evidence, meta-analyses and current European and German guidance now point in the same direction: the central question is no longer whether TP biopsy represents the more rational infectious-risk pathway, but how rapidly this evidence can be translated into a harmonised, risk-adapted European standard in which TP biopsy serves as the default route and antibiotic exposure is restricted to clearly defined higher-risk situations [1–5, 7].
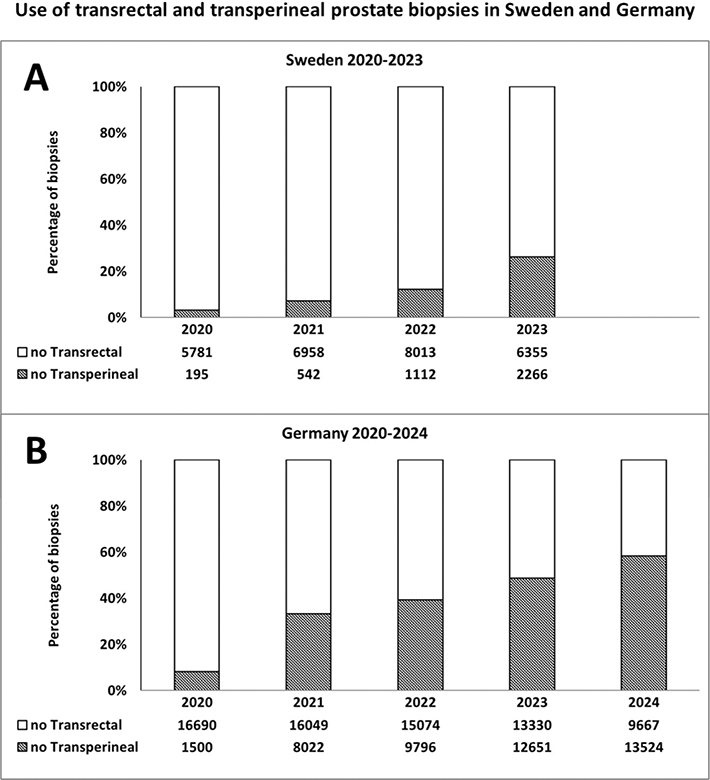
Figure 1. Use of transrectal and transperineal prostate biopsies in Sweden and Germany.
Note: Panel A displays annual proportions of transrectal and transperineal biopsy in the Swedish nationwide population-based cohort reported by Bonnedahl et al. for 2020 to 2023 [1]. Panel B displays annual proportions among DRG-coded inpatient prostate biopsies in Germany for 2020–2024, based on a custom tabulation provided by the Federal Statistical Office of Germany (Destatis) [6]. Absolute yearly case numbers are shown below each panel. The figure illustrates implementation trajectories across distinct data environments; German outpatient biopsies are not captured [1, 6].
References
[1] Bonnedahl J, Lundström KJ, Lampa E, et al. Risk of infectious complications after transperineal prostate biopsy compared to transrectal biopsy: nationwide population-based cohort study in Sweden. Scand J Urol. 2026;61:44–50. https://doi.org/10.2340/sju.v61.45537
[2] Bonkat G, Kranz J, Cai T, et al. EAU Guidelines on Urological Infections. EAU Guidelines. Presented at the EAU Annual Congress, London, United Kingdom, 13-16 March 2026. EAU Guidelines Office, Arnhem, The Netherlands; 2026:1-105.
[3] Cornford P, Tilki D, van den Bergh RCN, et al. EAU-EANM-ESTRO-ESUR-ISUP-SIOG Guidelines on Prostate Cancer. EAU Guidelines. Presented at the EAU Annual Congress, London, United Kingdom, 13-16 March 2026. EAU Guidelines Office, Arnhem, The Netherlands; 2026:1-267.
[4] Stangl FP, Day E, Vallée M, et al. Infectious complications after transrectal versus transperineal prostate biopsy: a systematic review and meta-analysis. Eur Urol Focus. 2026;12(2):275–283. https://doi.org/10.1016/j.euf.2025.07.005
[5] Wolff I, Büchner M, Hauner K, et al. Infectious complications following transperineal prostate biopsy with or without periprocedural antibiotic prophylaxis – a systematic review including meta-analysis of all comparative studies. Prostate Cancer Prostatic Dis. 2026;29(1):47–56. https://doi.org/10.1038/s41391-024-00934-9
[6] Federal Statistical Office of Germany (Destatis). Custom tabulation of DRG-based inpatient transrectal and transperineal prostate biopsy procedures in Germany, 2020-2024. Wiesbaden, Germany: Federal Statistical Office of Germany (Destatis); provided upon request; accessed March 23, 2026.
[7] Hauner K, Kranz J, Wagenlehner FME, et al. Perioperative and peri-interventional antibiotic prophylaxis in urology: key recommendations from the German Interdisciplinary AWMF S3 clinical practice guideline. Urol Int. 2026:1–15. https://doi.org/10.1159/000550029