RESEARCH LETTER
Optilume® for panurethral stricture: the good, the bad, and the ridiculous
Lukas A. Jelisejevas†, Gennadi Tulchiner and Peter Rehder†
Department of Urology, Medical University Innsbruck, Innsbruck, Austria
KEYWORDS: Drug-coated balloon dilation; paclitaxel; urethral stricture; urethroplasty; urethral reconstruction; direct vision internal urethrotomy; DVIU
Citation: Scandinavian Journal of Urology 2026, VOL. 61, 166–169. https://doi.org/10.2340/sju.v61.46024.
Copyright: © 2026 The Author(s). Published by MJS Publishing on behalf of Acta Chirurgica Scandinavica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 27 September 2025; Accepted: 13 April 2026; Published: 11 May 2026
CONTACT: Lukas A. Jelisejevas lukas.jelisejevas@i-med.ac.at Department of Urology, Medical University Innsbruck, Anichstrasse 35, 6020 Innsbruck, Austria
†Equally contributing authors.
Introduction
Panurethral strictures are uncommon, with lichen sclerosus representing the most frequent underlying aetiology [1]. Their management is surgically demanding and often requires complex, multistage reconstructive procedures. A variety of techniques – including graft‑ and flap‑based urethroplasties – are available, but they require substantial surgical expertise, and successful outcomes are largely dependent on surgeon experience. Although reconstructive surgery can achieve favourable results when performed in specialised centres, many patients remain unsuitable for such interventions due to comorbidities, frailty, or prior failed operations.
In this population, prolonged use of indwelling urethral catheters is common. Catheter‑associated urethral injuries (CAUIs) occur in up to 80% of individuals with long‑term catheterisation, and as many as 78% of these injuries progress to urethral stricture formation [2]. Given the considerable morbidity associated with chronic catheter dependence, there is a clear unmet need for minimally invasive treatment options for patients who are unfit for formal urethral reconstruction.
The Optilume drug-coated balloon (Laborie, Plymouth, MN, USA) combines coaxial mechanical dilation with local delivery of the antimitotic agent paclitaxel, which inhibits cell proliferation. It is safe and superior to standard endoscopic treatments (urethral dilation and direct visual internal urethrotomy [DVIU]), as shown in ROBUST trials [3, 4]. Current evidence supports the use of drug-coated balloon dilation (DCBD) for recurrent anterior strictures < 3 cm [3]. Several recent studies report on the use of DCBD in longer strictures or in different locations [5–8]. In this case series, we present three patients with panurethral stricture disease, treated with three Optilume DCBDs placed in series one after another from proximal to distal during one session. The aim of this retrospective study was to describe the feasibility, safety, and short‑term functional outcomes of triple DCBD for men with panurethral stricture disease who were unsuitable for or declined urethral reconstruction.
Material and methods
Study population
We conducted a retrospective review of patients who underwent Optilume DCBD for urethral stricture disease at our tertiary referral centre. Between June 2023 and January 2025, three male patients presented with panurethral strictures in the urological outpatient clinic. All patients provided informed consent for the procedure and for inclusion in this analysis. Diagnosis was confirmed and stricture length was measured by urethrocystoscopy and retrograde urethrography; voiding cystourethrography (VCUG) was performed when feasible (Figure 1).

Figure 1. Preoperative voiding cystourethrogram showing multiple urethral strictures.
Surgical technique
All procedures were performed in the outpatient clinic with the patient in the lithotomy position. Local urethral anaesthesia was achieved using lidocaine gel. A 0.035” hydrophilic guidewire was then advanced through the urethra under cystoscopic or radiographic guidance. Predilation to 20 French was carried out using hydrophilic urethral dilators. Over the same guidewire, the first 5‑cm, 30‑French Optilume DCB was introduced into the proximal urethra. Positioning was performed under direct vision alongside a 17‑French endoscope, ensuring at least 0.5 cm of proximal overlap into healthy urethral lumen. The balloon was inflated with sterile saline or contrast medium to 10 bar and maintained for 10 min. The procedure was then repeated in a stepwise fashion for the more distal segments of the stricture until the entire urethra had been treated. In all cases, three Optilume DCBs were deployed sequentially in a proximal‑to‑distal series (Figure 2). Upon completion, a 14‑French Foley catheter was inserted carefully without repeat endoscopy to minimise potential paclitaxel washout. The catheter was removed on postoperative day 5, followed by a VCUG to assess urethral patency. Patients were evaluated every 3 months, including assessment of uroflowmetry, post‑void residual (PVR) volume, catheter‑free voiding, and the ability to pass a 14‑French transurethral catheter. Any requirement for retreatment or catheterisation was considered treatment failure. The study was approved by the Institutional Ethics Committee of Medical University Innsbruck (protocol number 1101/2022).
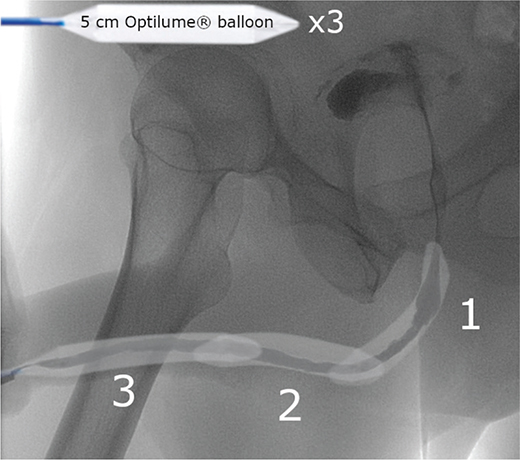
Figure 2. Scheme showing the order and location of three Drug-Coated Balloon Dilations in series.
Safety considerations
None of the patients were sexually active; therefore, recommendations regarding barrier contraception after paclitaxel exposure were not applicable. According to the Food and Drug Administration (FDA) premarket approval data (December 2021), systemic absorption of paclitaxel following intraurethral use of a single Optilume device is minimal, with plasma concentrations remaining below the limit of quantification in 99% of samples and exceeding the limit of detection in only one of 143 measured samples. These findings indicate that systemic exposure is negligible, suggesting that the use of multiple devices within a single procedure is unlikely to pose meaningful toxicological risk. Furthermore, paclitaxel-coated endovascular devices have been extensively used in peripheral artery disease without evidence of increased long‑term mortality, supporting the overall safety profile of paclitaxel‑coated technology [9].
Patient summaries – All with panurethral strictures
Patient 1
A 43‑year‑old male with severe lichen sclerosus and phimosis, for which circumcision had been performed. During follow‑up, he developed multifocal intraurethral papillomas associated with human papillomavirus infection, treated endoscopically with laser ablation. He subsequently developed panurethral stricture disease managed with multiple prior interventions, including DVIU ± intralesional mitomycin, serial urethral dilations, and regular self‑dilation.
Patient 2
A 73‑year‑old male with diabetes mellitus and a history of childhood hypospadias repair performed using a multistage preputial or ventral skin‑flap technique typical of the era. Postoperative complications included meatal stenosis, treated with meatoplasty. In adulthood, he developed bladder neck stenosis, managed with repeated bladder‑neck incisions ± intralesional mitomycin. He also had a recurrent stricture at the proximal margin of his childhood reconstruction and experienced recurrent urinary tract infections.
Patient 3
An 83‑year‑old male with a long history of complex urethral stricture disease. Previous treatments included two staged urethral reconstructions using buccal and lingual mucosa grafts, multiple DVIUs, and more than 15 simple urethral dilations. His American Society of Anaesthesiologists (ASA) classification was III–IV, and he was deemed unfit for further reconstructive surgery or general anaesthesia.
Results
Success was defined as spontaneous voiding without the need for catheterisation or retreatment. Median follow‑up was 19 months (range, 15–24). All three patients maintained urethral patency at their most recent evaluation and required no additional urethral interventions. Objective functional outcomes improved substantially. The mean maximum flow rate (Qmax) increased from 7.4 ± 3.1 mL/s pre‑procedure to 16.8 ± 4.4 mL/s at last follow‑up. Correspondingly, mean PVR volume decreased from 145 ± 57.7 mL to 23.3 ± 20.8 mL. Subjectively, all patients reported marked clinical improvement. On the Patient Global Impression of Improvement (PGI‑I) scale, each rated their outcome as ‘very much better’.
Patient 1 remained symptom‑free for 24 months, voiding effectively with no measurable PVR volume.
Patient 2 demonstrated a patent urethra for 19 months, with a stable PVR of <50 mL and no episodes of urinary tract infection.
Patient 3 maintained patency for 15 months before experiencing a gradual decline in urinary stream strength. Based on his prior clinical course, he requested repeat DCBD to prevent progression to recurrent bladder outlet obstruction.
Discussion
In this case series, we report the feasibility and short‑term outcomes of triple DCBD for panurethral stricture disease in three highly heterogeneous patients who were either unfit for reconstructive surgery or preferred a minimally invasive alternative. All patients experienced symptomatic improvement, maintained urethral patency at their last follow‑up, and reported substantial subjective benefit on the PGI‑I scale.
Managing panurethral strictures remains challenging, particularly in patients with significant comorbidities or prior failed reconstructions. For some individuals, long‑term indwelling catheterisation may be the only viable alternative; however, CAUI is common and contributes to stricture formation and morbidity. In this context, DCBD offers a minimally invasive option that can be performed under local anaesthesia and may help reduce the need for chronic catheter use or repeated endoscopic procedures.
The use of three DCBs in a single session represents an off‑label and relatively aggressive approach. While such an approach may be inappropriate for patients with severe frailty – particularly those who already require indwelling catheters for medical management – it may be reasonable in selected individuals with functional status preserved enough to benefit from catheter‑free voiding. A tailored approach is necessary, and these findings highlight the importance of individualised decision‑making based on patient goals, comorbidities, and life expectancy.
Cost considerations
Cost is an important factor in evaluating the clinical applicability of this technique. Using three devices in a single procedure significantly increases the financial burden. This expense must be justified by anticipated clinical benefit, especially in elderly or multimorbid patients for whom long‑term durability may be limited. Future economic analyses are warranted to better assess cost‑effectiveness and guide patient selection.
Limitations
This study has several limitations. Firstly, the sample size is very small (n = 3), which restricts the generalisability of our findings. Secondly, the observational nature of this case series limits any conclusions regarding relative efficacy compared with established surgical or endoscopic approaches. Thirdly, follow‑up duration was limited, and longer‑term outcomes – including durability beyond 24 months – remain unknown. Larger prospective studies with standardised outcome reporting are needed to validate these preliminary observations and to define the role of extended‑length drug‑coated balloon treatment in panurethral stricture disease.
Conclusion
Triple DCBD appears feasible and provides short‑term symptomatic relief in selected patients with panurethral stricture disease who are unsuitable for or decline reconstructive surgery. Given the small sample size, limited follow‑up, and substantial cost, this approach should be considered cautiously and reserved for carefully selected individuals. Larger controlled studies are required to determine long‑term efficacy, safety, and cost‑effectiveness.
References
[1] Kulkarni S, Kulkarni J, Surana S, et al. Management of panurethral stricture. Urol Clin North Am. 2017;44:67–75. https://doi.org/10.1016/j.ucl.2016.08.011
[2] Jeffery N, Mundy A. Innovations in indwelling urethral catheterisation. BJU Int. 2020;125:664–668. https://doi.org/10.1111/bju.14994
[3] VanDyke ME, Morey AF, Coutinho K, et al. Optilume drug-coated balloon for anterior urethral stricture: 2-year results of the ROBUST III trial. BJUI Compass. 2024;5:366–373. https://doi.org/10.1002/bco2.312
[4] DeLong J, Virasoro R, Pichardo M, Estrella R, Rodríguez Lay R, Espino G, Elliott S. Long-Term Outcomes of Recurrent Bulbar Urethral Stricture Treatment With the Optilume Drug-Coated Balloon: Five-Year Results From the ROBUST I Study. J Urol. 2025 Jan;213(1):90-98. Epub 2024 Aug 30. PMID: 39213367; PMCID: PMC12708045.https://doi.org/10.1097/JU.0000000000004229
[5] Estaphanous P, Khalifa AO, Makar Y. Efficacy and Safety of Optilume Drug-Coated Balloon for Urethral Stricture Treatment: A Systematic Review and Meta-Analysis. Cureus. 2024 Nov 20;16(11):e74069. PMID: 39712830; PMCID: PMC11660187. https://doi.org/10.7759/cureus.74069
[6] Jelisejevas LA, Wassermann J, Tulchiner G, et al. Optilume drug-coated balloon for acute urinary retention after failed treatment for complex recurrent urethral stricture disease. Medicina. 2025;61:700. https://doi.org/10.3390/medicina61040700
[7] Jelisejevas LA, Tulchiner G, Rehder P. Optilume drug-coated balloon dilation for male sphincteric (membranous) urethral strictures: 53 consecutive cases. J Clin Med. 2025;14:8369. https://doi.org/10.3390/jcm14238369
[8] Patel HV, Erickson BA, Abbasi B, et al. Early real-world experience with optilume drug-coated balloon for anterior urethral strictures and posterior urethral stenoses. Urology. 2025;383:S0090-4295(25)01012-X. https://doi.org/10.1016/j.urology.2025.10.025
[9] Nordanstig J, James S, Andersson M, et al. Mortality with paclitaxel-coated devices in peripheral artery disease. N Engl J Med 2020;383:2538–2546. https://doi.org/10.1056/NEJMoa2005206