QUIZ SECTION
Bilateral Symmetrical Nodules on the Thumbs in a Female Patient: A Quiz
TungChun LEE1, YiKe HUANG1, Juan WANG1* and Zhimiao LIN1,2*
1Department of Dermatology, Xiamen Chang Gung Hospital, No.123 Xiafei Road, Haicang District, Xiamen 361026, China and 2Dermatology Hospital, Southern Medical University, No. 2 Lujing Road, Yuexiu District, Guangzhou 510091, China. E-mail: liumengzhuang@126.com; zhimiaolin@bjmu.edu.cn
Citation: Acta Derm Venereol 2023; 103: adv11143. DOI https://doi.org/10.2340/actadv.v103.11143.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Published: Aug 16, 2023
Competing interests and funding: The authors have no conflicts of interest to declare.
A 22-year-old Chinese woman presented with asymptomatic bilateral solitary nodules on her thumbs, which had been present since birth. There was no history of trauma, injection, or relevant family history. Physical examination revealed symmetrical, smooth, skin-coloured, hard nodules at the level of the metacarpophalangeal joints of the thumbs, measuring 3.0×6.0 mm, with no tenderness, itching, ulceration, or extrusion (Fig. 1). After obtaining informed consent, the lesions were excised, and a histopathological examination was performed.

Fig. 1. Clinical photography. Symmetrical skin-coloured nodules at the level of the metacarpophalangeal joints of the thumb.
What is your diagnosis? See next page for answer.
ANSWERS TO QUIZ
Bilateral Symmetrical Nodules on the Thumbs in a Female Patient: A Commentary
Diagnosis: Rudimentary polydactyly (RP)
Histopathological analysis revealed hyperkeratosis and acanthosis, with elongated rete ridges in the epidermis. Nerve bundles surrounded by thin connective tissues of collagen fibres were seen in the dermis, with no osteoid or cartilage (Fig. 2A, B). Multiple Wagner-Meissner bodies were evident in the deep dermis (Fig. 2C) confirming a diagnosis of rudimentary polydactyly (RP). No recurrence was observed 6 months post-excision.
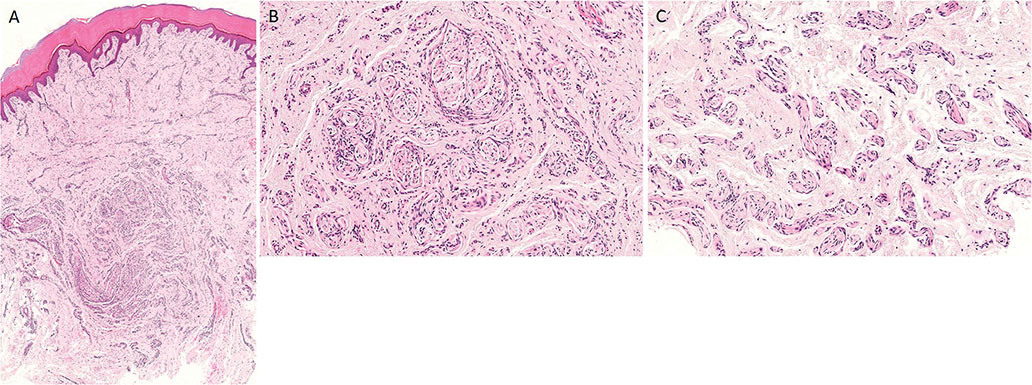
Fig. 2. (A, B) Histopathology shows compact keratin, acanthosis with elongated rete, and numerous intradermal nerve bundles in the dermis. (A: haematoxylin and eosin staining, original magnification ×2.5; B: haematoxylin and eosin staining, original magnification ×10). (C) Higher magnification highlights the multiple Wagner-Meissner bodies within the deep dermis. (Haematoxylin and eosin staining, original magnification ×10).
Polydactyly, otherwise known as accessory digits, is rarely managed by dermatologists. RP is a congenital anomaly first described in 1954 (1), which often consists of a poorly formed digit, piece of cartilage, or vestigial nail apparatus, and is considered an autosomal-dominant disorder with an unknown genetic basis (2). RP is characterized by isolated skin-coloured nodules or pedunculated cord-like structures, primarily at the ulnar side of the little finger or sometimes the radial side of the thumb (3). Rudimentary digits on the bilateral radial aspect of the thumbs are extremely rare. Histologically, RP typically shows a marked neural proliferation in the dermis, with many Meissner corpuscles (also known as Wagner-Meissner corpuscles), which are ellipsoid mechanoreceptors that play an essential role in somatosensory acuity (3, 4). Occasionally, abundant Merkel cells are seen in the basal layer or superficial dermis. Some authors consider that the development of Meissner corpuscles and the generation of the cutaneous nerve plexus may be associated with Merkel cells in the early stages of RP (4).
The aetiology of RP is poorly understood. Shapiro et al. investigated RP, finding similar histological features between acquired traumatic neuroma and RP, which suggests that their occurrence is a result of in utero auto-amputation (5). In this case, marked and variably sized nerve structures and a large number of Wagner-Meissner bodies in the dermis were observed. Although these histological features are characteristic of both traumatic neuroma and RP, lack of a precedent trauma helps to exclude the diagnosis of traumatic neuroma.
RP may also be confused with palisaded encapsulated neuroma, which often occurs as a nodule or nodules on the face, and histopathologically with well-circumscribed hypertrophic nerve bundles encapsulated by perineural cells (6). Other differential diagnoses include acquired digital fibrokeratoma and superficial acral fibromyxoma (2). Acquired digital fibrokeratoma typically presents as an asymptomatic, dome or bullet-shaped solitary nodule on the fingers or toes and acanthotic epidermis with thick collagen bundles oriented along the long axis of the lesion on histological analysis (7). Superficial acral fibromyxoma classically presents as a pink to flesh-coloured nodule located on the subungual or periungual region of the toes and fingers. The lesion is composed mainly of spindle-shaped and stellate cells, set in a myxocollagenous stroma with prominent vessels and mast cells (8).
There is no standardized treatment for patients with RP. As most cases are asymptomatic, conservative approaches are generally applied. We do not promote the use of ligatures, as they will leave a more noticeable and potentially painful eminence. Shave excision and laser therapy may cause unacceptable traumatic neuromas (2, 9). Thus, some authors recommend a sufficient depth of surgical excision, which is both curative and diagnostic (10).
The data and figures in this article were collected in accordance with Institutional Review Board (IRB) approval.
REFERENCES
- Hare PJ. Rudimentary polydactyly. Br J Dermatol 1954; 66: 402–408.
- Upjohn E, Barlow R, Robson A. Rudimentary polydactyly in an adult: an unusual presentation to a dermatological surgery unit. Australas J Dermatol 2006; 47: 206–208.
- Kitayama Y, Tsukada S, Ishikura N, Ide Y, Kojima M. Rudimentary polydactyly: report of five cases. J Hand Surg Am 1985; 10: 382–385.
- Ban M, Kitajima Y. The number and distribution of Merkel cells in rudimentary polydactyly. Dermatology 2001; 202: 31–34.
- Shapiro L, Juhlin EA, Brownstein MH. ‘Rudimentary polydactyly’: an amputation neuroma. Arch Dermatol 1973; 108: 223–225.
- Newman MD, Milgraum S. Palisaded encapsulated neuroma (PEN): an often misdiagnosed neural tumor. Dermatol Online J 2008; 14: 12.
- Shih S, Khachemoune A. Acquired digital fibrokeratoma: review of its clinical and dermoscopic features and differential diagnosis. Int J Dermatol 2019; 58: 151–158.
- Ashby-Richardson H, Rogers GS, Stadecker MJ. Superficial acral fibromyxoma: an overview. Arch Pathol Lab Med 2011; 135: 1064–1066.
- Dijkman RR, van Nieuwenhoven CA, Hovius SER, Hülsemann W. Clinical presentation, surgical treatment, and outcome in radial polydactyly. Handchir Mikrochir Plast Chir 2016; 48: 10–17.
- Leber GE, Gosain AK. Surgical excision of pedunculated supernumerary digits prevents traumatic amputation neuromas. Pediatr Dermatol 2003; 20: 108–112.