Lesion of the Anal Margin in a Young Child: A Quiz
Claire Le Helloco1, Annabel Maruani1,2, Anne Le Touze3, Denis Herbreteau4 and Sophie Leducq1,2
1Department of Dermatology and Reference Center for Rare Diseases and Vascular Malformations (MAGEC), 3Department of Pediatric Surgery and 4Department of Neuroradiology and Interventional Radiology, University Hospital Center of Tours, Avenue de la République, FR-37044 Tours Cedex 9 and 2Universities of Tours and Nantes, INSERM 1246-SPHERE, Tours, France. E-mail: claire.le.helloco@gmail.com
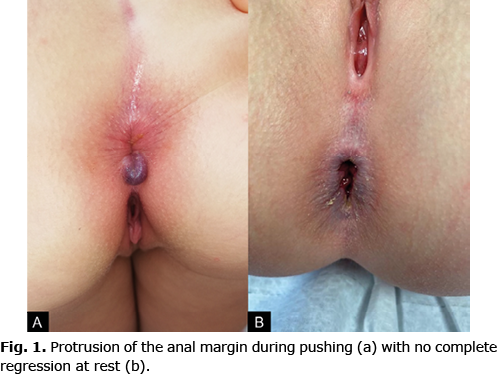
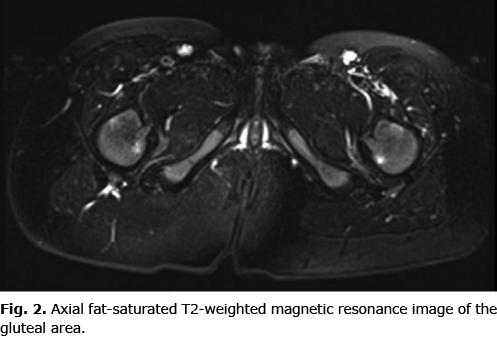
A 6-year-old girl, with no personal or family history, presented a 4-year history of painful anal mass prolapse. She had no constipation and no anal fissure. Oral laxatives and dietary modification were ineffective, and the condition worsened, leading to constant discomfort during defecation. Physical examination revealed protrusion of the anal margin during pushing (Fig. 1a), which did not completely disappear during rest (Fig. 1b), without anal fissure or perianal abscess. The parents did not report any bleeding. The rest of the clinical examination was normal. Magnetic resonance imaging (MRI) was performed and did not reveal any endo-canal extension (Fig. 2).
What is your diagnosis? See next page for answer.
Lesion of the Anal Margin in a Young Child: A Commentary
Acta Derm Venereol 2022; 102: adv00696.
DOI: 10.2340/actadv.v102.1177
Diagnosis: Venous malformation of the anal margin
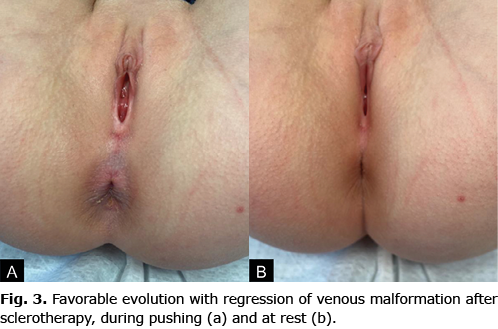
The lesion was treated under general anaesthesia with colonoscopy control by sclerotherapy with lauromacrogol (aethoxysklerol; or polidocanol). Despite difficulties in correctly visualizing the venous malformation (VM) while the child was under anaesthesia, sclerotherapy allowed for complete regression of the lesion as well as relief of pain and discomfort during defecation (Fig. 3).
VMs are congenital anomalies that might involve capillary, lymphatic, venous and arterial vessels (1). They are usually present at birth, although not always visible, and tend to worsen with age. They are most often located on the head, neck, trunk and limbs, with a unifocal lesion. VMs can spontaneously thrombose and induce pain and swelling (2). The diagnosis of VMs is most often made on clinical examination, but imaging (MRI) is required for a definitive diagnosis and diagnosis extension. A rectal localization of a VM, previously called a diffuse cavernous haemangioma of the rectum, is unusual and might be misdiagnosed as haemorrhoids. Management of rectal VMs may include surgery, which can induce significant morbidity, or sclerotherapy, if the rectal VM is symptomatic (3). Treatment by sclerotherapy under general anaesthesia is complex when reducing the VM volume with the patient in the supine position, and therefore requires a trained operator.
In the current patient, a diagnosis of haemorrhoids was initially suspected when she was 2 years old. However, haemorrhoids are rare in young children, and their existence is controversial. Indeed, the condition usually affects patients 45–65 years old, with a very low incidence under age 20 years (4). The clinical presentation of haemorrhoids is painless rectal bleeding during defecation with or without prolapsing anal tissue (5). Clinical examination shows dilated purplish-blue veins with prolapsed internal haemorrhoids and perianal skin tags with external haemorrhoids (6). Haemorrhoids are more common in older children with comorbidities than rectal venous malformations: in the literature, the most common cause of haemorrhoids in young children is portal hypertension (7, 8). Because rectal VM is a rare condition and not well known, inappropriate or delayed diagnosis and treatment often occurs. Thus, the diagnosis of VM must be considered in cases of pseudo-like haemorrhoidal lesions in children with no risk factors for haemorrhoids.
REFERENCES
- Wassef M, Blei F, Adams D, Alomari A, Baselga E, Berenstein A, et al. Vascular anomalies classification: recommendations from the International Society for the Study of Vascular Anomalies. Pediatrics 2015; 136: e203–e214.
- Behravesh S, Yakes W, Gupta N, Naidu S, Chong BW, Khademhosseini A, et al. Venous malformations: clinical diagnosis and treatment. Cardiovasc Diagn Ther 2016; 6: 557–569.
- Wang HT, Gao XH, Fu CG, Wang L, Meng RG, Liu LJ. Diagnosis and treatment of diffuse cavernous hemangioma of the rectum: report of 17 cases. World J Surg 2010; 34: 2477–2486.
- Johanson JF, Sonnenberg A. The prevalence of hemorrhoids and chronic constipation. An epidemiologic study. Gastroenterology 1990; 98: 380–386.
- Lohsiriwat V. Treatment of hemorrhoids: a coloproctologist’s view. World J Gastroenterol 2015; 21: 9245–9252.
- Hussain JN. Hemorrhoids. Prim Care 1999; 26: 35–51.
- Watanabe T, Ohno M, Tahara K, Tomonaga K, Ogawa K, Takezoe T, et al. Efficacy and safety of sclerotherapy with polidocanol in children with internal hemorrhoids. Pediatr Int 2021; 63: 813–817.
- Heaton ND, Davenport M, Howard ER. Symptomatic hemorrhoids and anorectal varices in children with portal hypertension. J Pediatr Surg 1992; 27: 833–835.