ORIGINAL REPORT
Off-label Prescription in Paediatric Dermatology: A Retrospective Observational Study in a Tertiary Hospital
Carmen COUSELO-RODRÍGUEZ1,2, Ana BATALLA1,2, Sandra MARTÍNEZ-FERNÁNDEZ1,2, Carmela DÁVILA-POUSA3, Diego SOTO-GARCÍA1,2, Lucía VILANOVA-TRILLO1,2 and Ángeles FLÓREZ1,2
1Department of Dermatology, University Hospital of Pontevedra, Pontevedra, 2DIPO Research Group, Galicia Sur Health Research Institute (IIS Galicia Sur), Sergas-Uvigo and 3Department of Pharmacy. University Hospital of Pontevedra, Pontevedra, Spain
Abstract
Off-label prescription in paediatric patients is common, where some studies indicate that dermatological conditions are more prone to off-label treatment. This is the first study to analyse the prevalence of off-label prescription in paediatric dermatology consultation. This retrospective observational study was performed using the medical records of paediatric patients who were evaluated in a paediatric dermatological consultation in Pontevedra University Hospital, Pontevedra, Spain. Of the 468 patients reviewed, 186 prescriptions were issued and 51.10% were off-label prescription drugs. The dermatological conditions for which off-label prescription was most common were atopic dermatitis (29.0%), followed by warts (12.9%) and infantile haemangiomas (11.8%). With respect to drugs, topical tacrolimus (23.7%) was the most frequently prescribed off-label drug. The main reason for prescribing an off-label drug was for a disease not included on the label (62.4%), followed by issuing it at a lower age than authorized (55.9%). There was a significant association between a higher percentage of off-label prescription and younger age (p < 0.001), and the treatment of vitiligo, infantile haemangiomas and warts (p < 0.001). Likewise, the off-label prescription was significantly more common in the case of topical terbinafine, timolol, desloratadine and topical salicylic acid (p < 0.001). To conclude, off-label prescription is predominant in paediatric dermatology, as observed in 51.1% of our patients.
SIGNIFICANCE
This study analysed the prevalence of off-label prescription in paediatric dermatology consultation and determined the characteristics and factors associated with this prescription. To the best of our knowledge, this issue had not been addressed previously. Off-label prescription was found to be the predominant situation in paediatric dermatology, as was observed in 51.1% of prescriptions in this study.
Key words: child; dermatology; off-label use; prevalence; paediatrics.
Citation: Acta Derm Venereol 2023; 103: adv11937. DOI: https://doi.org/10.2340/actadv.v102.11937.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: Oct 10, 2023; Published: Dec 11, 2023
Corr: Carmen Couselo-Rodríguez, Dermatology Department, Centro de Especialidades Mollabao, Rúa Simón Bolivar S/N, ES-36001 Pontevedra, Spain. E-mail: carmen.couselo.rodriguez@sergas.es; carmencouselo@hotmail.com
Competing interests and funding: CC-R received honoraria, support for training activities or has participated in clinical trials from: Mylan, Sanofi, Leo-Pharma and Pierre Fabre. AB received honoraria, support for training activities or has participated in clinical trials from: Abbvie, Celgene, Faes pharma, Isdin, Janssen, Leo-Pharma, Leti Pharma, Lilly, Mylan, Novartis, Pfizer, Pierre Fabre and Sanofi-Genzyme. DS received honoraria, support for training activities or has participated in clinical trials from Sun Pharma. LV-T received honoraria and support for training activities from Lilly and Company and UCB. ÁF received honoraria, support for training activities or has participated in clinical trials from: Abbvie, Almirall, Amgen, Celgene, Janssen, Kyowa Kirin, Leo-Pharma, Lilly, Novartis, Pfizer, Roche Farma, Sanofi, Sun Pharma, Takeda and UCB Pharma.
INTRODUCTION
Off-label prescription in paediatric patients is common due to the lack of clinical trials that evaluate the safety and efficacy of drugs in children. Factors that could influence this situation are the costs of these studies and the legal and ethical implications (1). Some studies carried out in paediatrics indicate that dermatological prescriptions are prone to be off-label more frequently than prescriptions for non-dermatological diseases (2, 3).
The aim of this study was to analyse the prevalence of off-label prescription in a paediatric dermatology consultation, and to determine the characteristics and factors associated with this off-label prescription. To the best of our knowledge, this is the first study to assess this issue.
MATERIALS AND METHODS
This retrospective observational study was performed using the medical records of paediatric patients who were evaluated in a paediatric dermatological consultation in Pontevedra University Hospital, Pontevedra, Spain, during a period of 1 year, from 1 January 2019 to 31 December 2019. This monographic consultation of paediatric dermatology is carried out 1 day a week and evaluates patients from 0 to 14 years, both included. A power calculation was performed. The study intended to extract a sample size using the prevalence estimation formula to test the hypothesis that the expected proportion of off-label drugs that were prescribed exceeded half of the total (51%). A total of 1,092 consultations were included in the study during the 1-year period. Thus, considering an accuracy of 3.5% in estimating a ratio using a normal asymptotic bilateral confidence interval with correction for finite populations to 95%, it was estimated that it would be necessary to include a minimum of 467 subjects in the study.
The inclusion criteria consisted of patients who attended the paediatric dermatology consultation that had received a systemic or topical drug on the day of the consultation. Patients receiving topical corticosteroids in monotherapy were excluded for 3 reasons: (i) due to wide use for conditions not always indicated on the label; (ii) for having been frequently prescribed by non-dermatologist physicians prior to assessment by a dermatologist; and (iii) due to their being available without prescription in pharmacies. In addition, it is common for patients to have previously administered leftover corticosteroids at home; thus, patients sometimes use a different topical corticosteroid from the one prescribed by the dermatologist. Patients who received medication and healthcare products in the context of a clinical trial were also excluded.
Besides demographic data and patients’ weight, characteristics of the prescribed drugs were recorded (treated disease according to International Classification of Diseases – 10th revision (ICD-10) classification; therapeutic group according to the WHO; therapeutic drug; type of administration; drug concentration if topical; drug dosage; existence of label, indications on label with respect to age, weight, dosage and pathology; and the reason for usage off-label). If the label did not provide a numerical value for the authorized age, the announcement “should not be used in children” was interpreted as “should not be used in patients under 18 years of age” (4).
Four categories were considered for age group classification: neonate (0–27 days); infant (28 days to 23 months); children (2–11 years); and adolescent (12–14 years).
Prescriptions were divided into the following categories: unlicensed (compounded topical preparations); off-label (licensed drugs used outside the officially approved conditions of use for a medicine); and on-label (licensed drugs used according to the officially approved conditions of use for a medicine). Usage under off-label conditions included an age, weight, disease, or dosage different from that registered on the label.
Patient data were collected in a pseudonymized manner, and the study was authorized by the Research Ethics Committee of our centre(CEIm-G (Comité de Ética da Investigación con medicamentos de Galicia), Santiago de Compostela (Galicia); CEIm-G project number 2020/549).
Statistical analysis
Data were analysed with R Statistics program (version R i386 3.4.2; R Core Team (2021) https://www.R-project.org/.1). A descriptive analysis was performed. A χ2 test was applied to compare qualitative variables. Quantitative variables were compared by Student’s t-test. A p-value less than 0.05 was considered significant.
RESULTS
Of the 468 patients reviewed, 138 (29.49%) received some topical or systemic drug (53.62% males, mean age 8.17 years). Most of the cases received only 1 drug (101/138; 73.19%), while the remaining (37/138; 26.81%) received 2 or more.
Thus, a total of 186 prescriptions were issued (53.23% males, mean age 8.47 years) (Table I). Atopic dermatitis was the main disease treated (77/186; 41.40%), followed by acne (21/186; 11.29%). With respect to treatment, topical tacrolimus was the most frequently prescribed drug (51/186; 27.42%), and topical administration the predominant route of administration (140/186; 75.27%). Taking into account all prescribed drugs, most (182/186; 97.85%) were licensed drugs. The remaining 4 (2.15%) were unlicensed drugs, which required compounded topical preparations (Fig. 1).
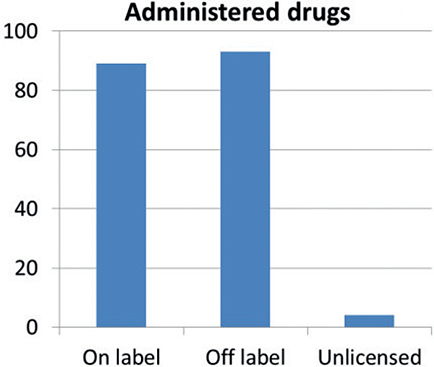
Fig. 1. Administered drugs. Unlicensed drugs that required compounded topical preparations: rapamycin 0.4% o/w; anthralin 1% o/w; carbocisteine 10% + urea 5% o/w; clobetasol propionate 0.015% + retinoic acid 0.025% + minoxidil 2% hydroalcoholic solution.
Among the licensed drugs, off-label prescription was predominant (93/182; 51.10%). The age group that most frequently received off-label prescription was children (52/93; 55.91%), followed by infants (25/93; 26.88%) (Table II).
The pathologies for which off-label prescription was most common were atopic dermatitis (27/93; 29.03%), followed by warts (12/93; 12.90%) and infantile haemangiomas (11/93; 11.83%). Topical tacrolimus (22/93; 23.66%), desloratadine (19/93; 20.43%) and topical timolol (9/93; 9.68%) were the most frequently prescribed off-label drugs. Most of the off-label treatments were administered topically (65/93; 69.89%). In particular, topical tacrolimus 0.1% was prescribed off-label in patients with atopic dermatitis under 16 years of age (15/93) and in patients with vitiligo (8/93); desloratadine was prescribed off-label to relieve pruritus in atopic dermatitis (17/93) and after arthropod bites (1/93), and topical timolol was indicated off-label to superficial infantile haemangiomas (9/93). Terbinafine and topical salicylic acid were used for approved diseases (fungal infections and warts respectively) but at a younger age than authorized.
The main reason for prescribing an off-label drug was for a disease not included on the label (58/93; 62.37%), followed by issuing it at a lower age than authorized (52/93; 55.91%) (Table III). No patient received a drug at a dose other than that indicated by weight. Three-quarters (71/93; 76.34%) of the prescribed drugs account for only 1 reason to be used off-label, while 22/93 (23.66%) complied with 2 or more reasons.
There was a significant association between a higher percentage of off-label prescription and younger age (p < 0.001). A higher prevalence of off-label drug use in the treatment of vitiligo, infantile haemangiomas and warts was also significant (p < 0.001). Likewise, the off-label prescription was significantly more common in the case of topical terbinafine, timolol, desloratadine and topical salicylic acid (p < 0.001).
DISCUSSION
In paediatric ages, off-label medications are commonly prescribed because of the lack of effective available alternatives (5, 6). Nevertheless, this form of prescription is often supported by medical literature (4). A narrative review has shown that the frequency of paediatric patients exposed to at least 1 off-label drug ranged from 36.3 to 97% (7). When studying dermatological prescriptions in a general paediatric consultation, Schirm et al. (4) found that 73.3% of prescriptions were off-label. Similarly, the current study found that 51.10% of prescriptions were off-label. This high percentage of off-label use in the dermatological field might be explained by the more frequent usage of the topical route of administration, since topical drugs are more likely to be used off-label than systemic drugs (4, 7).
Atopic dermatitis was the dermatological condition that most frequently required any treatment in the current study, and it was also the most common disease for which off-label drugs were prescribed. The main reason arose from the fact that tacrolimus 0.03% is indicated in the product license for patients older than 2 years old and tacrolimus 0.1% for patients older than 16 years old. Moreover, in the period when this study was conducted (year 2019) pimecrolimus was approved only for patients older than 2 years, although it is currently indicated from 3 months of age onwards. Furthermore, tacrolimus 0.1% is often prescribed for patients younger than 16 years. In addition, desloratadine, an antihistamine indicated for urticaria and allergic rhinitis according to label, was prescribed for pruritus control in patients with atopic dermatitis.
With respect to warts, topical salicylic acid is the treatment with the best evidence base and is the only option approved for warts by the Food And Drug Administration (8). This treatment is approved for patients older than 12 years. In the current study 9 out of 11 (81.82%) patients treated with topical salicylic acid were younger. Moreover, topical retinoids were administered to 3 patients below the authorized age who presented flat warts.
Infantile haemangioma often receives treatment with topical timolol. This treatment is supported by clinical trials as a safe and effective therapeutic option for early proliferative infantile haemangiomas (9). However, it is not approved for this condition, as it is only indicated for glaucoma. Moreover, propranolol, a non-selective beta-adrenergic receptor antagonist, is indicated for infantile haemangioma, but should be initiated between 5 weeks and 5 months of life. Again, the use of propranolol outside this age range, constitutes an off-label use. In the current study, propranolol was administered in 2 infants aged 6 and 7 months.
There are no approved drugs for the treatment of vitiligo, thus topical calcineurin inhibitors are often prescribed as first-line treatment in off-label conditions (10). As in atopic dermatitis, these topical calcineurin inhibitors are commonly prescribed in higher concentrations or at earlier ages than those indicated on the label.
Parikh et al. (5) published a study in which 29% of children younger than 12 years old who consulted for acne, received off-label drugs. In the current study 2 of the 21 prescriptions for acne were in patients younger than 12 years, both receiving off-label topical retinoids.
In a recent study, Mahe et al. (11) found that 34.9% of paediatric patients with psoriasis evaluated in public hospitals received off-label prescriptions, where topical vitamin D was the main off-label treatment. Although this disease was scarcely represented in our study population (n = 4), all the patients with psoriasis received topical off-label treatments (tacrolimus, calcipotriol and calcipotriol combined with betamethasone).
Interestingly, it was found that the main reason for prescribing an off-label drug in dermatology paediatric patients was to prescribe it for a pathology not indicated on the label. In contrast, the main reason given for paediatricians for prescribing off-label in general paediatrics was to use a drug for a lower age than approved (12). None of our patients received a drug at a different dose than that corresponding to weight, which could be explained by the predominant topical administration.
As in other studies carried out by paediatricians, we also found a statistically significant association between lower patient ages and high off-label prescriptions (13, 14). With respect to the diseases and drugs in which off-label administration was most common in the current study population, the lack of studies dealing with this issue in paediatric dermatology prevents us from establishing comparisons.
The possibility that off-label prescription leads to a higher incidence of adverse drug reactions is a controversial finding (7). Nevertheless, it is notable that none of the patients who received an off-label prescription in this study presented any side-effects. Based on this observation, we consider that off-label prescription in paediatric dermatology patients is not an unsafe practice if supported by medical literature.
This study has several limitations. It took into account the label available at the time of prescription; hence pimecrolimus was considered off-label in patients under 2 years of age. Although this might have overestimated the off-label prescription, only 2 of the 93 (2.15%) off-label prescriptions corresponded to pimecrolimus in children under 2 years of age. Moreover, the study was conducted in a specific paediatric dermatology consultation, where conditions of high prevalence such as acne, are under-reported due to their greater management in general consultations. Finally, even though this is a single-centre study, to the best of our knowledge, it is the first study to evaluate off-label prescription in a paediatric dermatology consultation.
In conclusion, off-label prescription is the predominant situation in paediatric dermatology, as was observed in 51.10% of prescriptions in this study. The main reason for this practice is to administer a drug for a pathology that is not authorized on-label. A higher prevalence of off-label prescription was found in younger patients. Regarding pathologies, atopic dermatitis, infantile haemangioma, vitiligo and warts require increased efforts to improve paediatric labelling. Healthcare authorities should support paediatric investigation and encourage pharmaceutical enterprises to provide paediatric drug information on the label. Meanwhile, the medical literature will help clinicians to prescribe off-label medication in the absence of approved therapeutic alternatives.
ACKNOWLEDGEMENTS
The authors acknowledge the contribution of José Aguayo Arjona, for his contribution to statistical analysis.
This study was authorized by the Research Ethics Committee of our centre.
REFERENCES
- Joseph PD, Craig JC, Caldwell PH. Clinical trials in children. Br J Clin Pharmacol 2015; 79: 357–369.
- Lass J, Irs A, Pisarev H, Leinemann T, Lusar I. Off label use of prescription medicines in children in outpatient setting in Estonia is common. Pharmacoepidemiol Drug Saf 2011; 20: 474–481.
- Zhang L, Li Y, Liu Y, Zeng L, Hu D, Huang L et al. Pediatric off-label drug use in China: risk factor and management strategies. J Evid Based Med 2013; 6: 4–18.
- Schirm E, Tobi H, de Jong-van den Berg LTW. Risk factors for unlicensed and off-label drug use in children outside the hospital. Pediatrics 2003; 111: 291–295.
- Parikh SA, David SA, Krowchuk DP, Feldman SR. Common use of prescription off-label acne therapy in children younger than 12 years old. Pediatr Dermatol 2014; 31: 551–555.
- Wittich CM, Burkle CM, Lanier WL. Ten common questions (and their answers) about off-label drug use. Mayo Clin Proc 2012; 87: 982–990.
- Moulis F, Durrieu G, Lapeyre-Mestre M. Off-label and unlicensed drug use in children population. Therapie 2018; 73: 135–149.
- Gerlero P, Hernández-Martín Á. Treatment of warts in children: an update. Actas Dermosifiliogr 2016; 107: 551–558.
- Muñoz-Garza FZ, Ríos M, Roé-Crespo E, Bernabeu-Wittel J, Montesarrat-García MT, Puig L et al. Efficacy and safety of topical timolol for the treatment of infantile hemangioma in the early proliferative stage. JAMA Dermatol 2021; 157: 583–587.
- Roohaninasab M, Mansouri P, Seirafianpour F, Naeini AJ, Goodarzi A. Therapeutic options and hot topics in vitiligo with special focus on pediatrics’ vitiligo: a comprehensive review study. Dermatol Ther 2021; 34: e14550.
- Mahé E, Corgibet F, Maccari F, Hadj-Rabia S, Phan C, Ruer-Mulard M et al. Off-label drugs in childhood psoriasis. Ann Dermatol Venereol 2020; 147: 429–438.
- Blanco-Reina E, Vega-Jiménez MA, Ocaña-Riola R, Márquez-Romero EI, Bellido-Estévez I. Drug prescriptions study in the outpatient setting: assessment of off-label uses in children. Aten Primaria 2015; 47: 344–350.
- Ellul IC, Grech V, Attard-Montalto S. Paediatric off-label and unlicensed prescribing in primary care in Malta: prospective observational drug utilisation study. Int J Risk Saf Med 2015; 27: 123–134.
- Bazzano AT, Mangione-Smith R, Schonlau M, Suttorp MJ, Brook RH. Off-label prescribing to children in the United States outpatient setting. Acad Pediatr 2009; 9: 81–88.