QUIZ SECTION
Painful Erythematous Plaques on the Hands: A Quiz
Anna OCHI1, Yasuhiro MITSUI1,2*, Kohei OGAWA1 and Hideo ASADA1
1Department of Dermatology, Nara Medical University School of Medicine, Kashihara, Japan and 2Department of Dermatology, Nara Prefecture General Medical Center, Nara, Japan. *E-mail: nagaratenroku@yahoo.co.jp
Citation: Acta Derm Venereol 2023; 103: adv12344. DOI https://doi.org/10.2340/actadv.v103.12344.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Published: Jul 13, 2013
Competing interests and funding: The authors have no conflicts of interest to declare.
A 71-year-old man presented with painful erythematous plaques on his hands that had persisted for 1 week (Fig. 1A, B). He had a history of myelodysplastic syndrome (MDS), for which he was administered subcutaneous azacitidine (75 mg/m2/day for 7 consecutive days, every 28 days). A few days after the 7-day azacitidine regimen, erythematous plaques appeared on the palmar and dorsal surfaces of both hands. Vesicles and pustules were also observed, particularly on the left palm (Fig. 1C). At presentation, the patient had a temperature of 38.4°C. Blood tests revealed anaemia (haemoglobin level 6.8 g/dL; normal range 13.7–16.8 g/dL), thrombocytopaenia (platelet count 16,000/μL; normal range 158,000–348,000/μL), elevated C-reactive protein levels (17.77 mg/dL; normal < 0.14 mg/dL), and no leukocytosis or peripheral neutrophilia (white blood cell count 3600/μL, including 37% neutrophils, 43% lymphocytes and 12% blasts). A skin biopsy of the palmer lesion revealed marked papillary oedema, mild extravasation of erythrocytes, and a dense dermal neutrophilic infiltrate with nuclear dust (Fig. 1D, E). No vascular fibrinoid necrosis was observed.
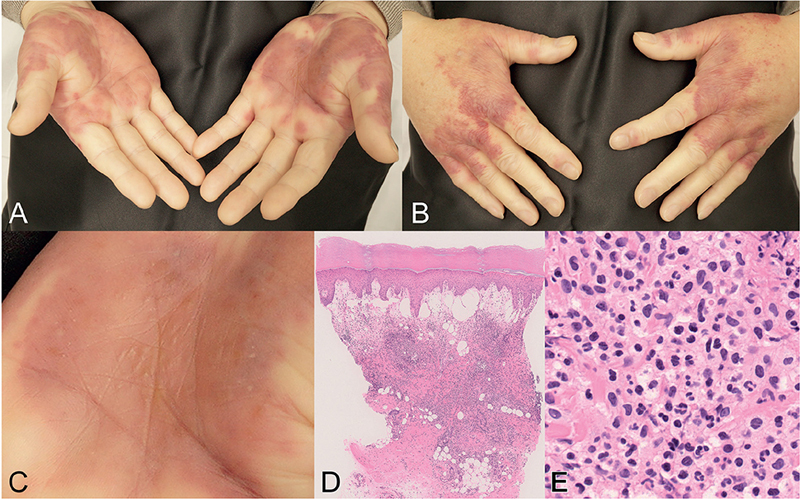
Fig. 1. Clinical and histopathological presentations. Erythematous plaques on (A) the palms and (B) dorsal hands. (C) Vesicles and pustules on the left palm (close-up view). (D) Skin biopsy of the palmar lesion reveals papillary dermal oedema and dense dermal infiltrates (haematoxylin-eosin (HE) staining, original magnification ×100). (E) Infiltration of neutrophils and nuclear dust (HE staining, original magnification ×400).
What is your diagnosis?
Neutrophilic dermatosis of the hands?
Localized cutaneous infection?
Cutaneous vasculitis?
Leukaemia cutis?
See next page for answer.
ANSWERS TO QUIZ
Painful Erythematous Plaques on the Hands: A Commentary
Diagnosis: Neutrophilic dermatosis of the hands
The clinical and histopathological features of this case were consistent with neutrophilic dermatosis of the hands (NDH), for which topical corticosteroid was initiated. The skin lesions mostly disappeared within 2 weeks. A second cycle of azacitidine was administered, and no similar eruptions were observed. Five weeks after the initial presentation, the patient died of pneumonia.
NDH was originally described as “pustular vasculitis of the hands” in 1995 (1). The original study reported 6 patients with skin lesions restricted to the dorsal hands and fingers, characterized by neutrophilic infiltrates with features of leukocytoclastic vasculitis (LCV). In addition, in 2000, a report described 3 similar patients without vasculitis on histopathology and proposed the designation “neutrophilic dermatosis of the dorsal hands” (2). Since lesions also affect the lateral hand and palm, the term NDH was used to collectively describe these unique manifestations (3). In some cases, other sites, such as the back and legs, were minimally involved (4). The presence or absence of vasculitis in patients with NDH has been discussed since the original description of the disease. If the findings of vasculitis in NDH are interpreted as LCV secondary to dense neutrophilic infiltrates similar to those in Sweet syndrome (SS), concluding that NDH is a subtype of SS becomes reasonable (5). Currently, this concept is generally accepted.
Similar to SS, NDH is characterized by fever, painful erythematous plaques, and peripheral and tissue neutrophilia (5). Tissue neutrophilia is present in almost all patients with NDH (95%), whereas leukocytosis or peripheral neutrophilia is observed in 33% of patients (6). In the current patient, tissue neutrophilia was present, but peripheral neutrophilia was not; however, this did not exclude the diagnosis of NDH.
NDH also shares a clinical feature with pyoderma gangrenosum (PG). Classic PG is characterized by ulceration commonly affecting the lower extremities. NDH may manifest ulceration, pustules, or bullae (6). Vesicular or bullous PG occurring on the hands may be diagnosed as NDH (6).
NDH is associated with various diseases and medications (7–9). The most common neoplasms are haematological disorders, including MDS, multiple myeloma, and acute myeloid leukaemia (7). NDH has also been reported in patients with solid organ tumours, such as lung cancer and renal cell carcinoma (3, 7). The most common inflammatory disorder is ulcerative colitis (3). Although rare, NDH has been reported to be induced by vaccines and lenalidomide (8, 9). There is also a report of NDH triggered by mechanical trauma (10). These associations have raised awareness about the importance of evaluating medical and drug histories, and prior mechanical trauma in patients with NDH.
The patient received azacitidine for MDS. Prior mechanical trauma was not evident. At the initial presentation, the timing of the appearance of skin lesions suggested a possible association between NDH and azacitidine. Although there are no reports regarding azacitidine-induced NDH, several studies have reported on azacitidine-induced SS (11, 12). Therefore, it was challenging to decide whether to discontinue azacitidine, which might have been the drug that induced NDH, or continue azacitidine to treat MDS possibly associated with NDH. Azacitidine is usually administered for 7 consecutive days, followed by a rest period of 21 days. In the current case, the skin lesions almost resolved within the rest period, which led us to decide on the re-administration of azacitidine. Given the absence of NDH recurrence after azacitidine re-administration, we postulated that in the current patient, NDH was secondary to MDS rather than to azacitidine.
NDH is treated with systemic and/or topical corticosteroids, dapsone, and colchicine (7). The patient responded well to treatment with topical corticosteroids. Systemic corticosteroids may be necessary for patients with NDH who are refractory to topical corticosteroids. Other alternatives, such as treatment of possible underlying diseases and termination of causative drugs, should be discussed on a case-by-case basis.
The differential diagnoses of NDH include localized cutaneous infections, vasculitis, skin involvement of myeloid malignancy such as leukaemia cutis (LC) and myelodysplasia cutis (MC). In many reported cases, NDH was initially misdiagnosed as cutaneous infections (1–3, 6). In patients exhibiting ulcerative plaques appropriate for sampling, bacterial culture should be performed to exclude infection. Even in cases where infection is initially suspected, the lack of response to antibiotics raises suspicion of NDH. Cutaneous vasculitis and NDH exhibit overlapping histopathological features. However, unlike NDH, cutaneous vasculitis clinically presents with palpable purpura and affects the extremities, not only the hands. Particularly in patients with myeloid malignancies, differentiating NDH from LC or MC might be difficult. Of note, in patients with myeloid malignancy-associated SS, neutrophils in the skin and malignant cells in haematopoietic samples showed common genetic profiles (13), suggesting that SS, LC and MC represent the disease spectrum (14). Histopathologically, LC and MC show infiltration of blasts and immature non-blast myeloid cells, respectively. However, SS exhibits infiltrates mainly comprising terminally differentiated neutrophils (15). A study of 7 MC cases showed that mature neutrophils were not identified in skin samples (14). In the current case, dermal infiltrates of mature segmented neutrophils were easily detectable. In addition, LC and MC usually show disseminated papules and plaques clinically. Although we could not definitely exclude the possibility of LC or MC without immunohistochemistry and genetic studies, the characteristic distribution of the lesions and histopathology favoured the diagnosis of a distributional variant of SS, NDH rather than LC or MC.
Dermatologists should be aware that neutrophilic dermatosis may occur solely on the hands. Evaluation of underlying diseases and possible associated drugs is necessary for the diagnosis and proper management of NDH.
REFERENCES
- Strutton G, Weedon D, Robertson I. Pustular vasculitis of the hands. J Am Acad Dermatol 1995; 32: 192–198.
- Galaria NA, Junkins-Hopkins JM, Kligman D, James WD. Neutrophilic dermatosis of the dorsal hands: pustular vasculitis revisited. J Am Acad Dermatol 2000; 43: 870–874.
- Weenig RH, Bruce AJ, McEvoy MT, Gibson LE, Davis MD. Neutrophilic dermatosis of the hands: four new cases and review of the literature. Int J Dermatol 2004; 43: 95–102.
- DiCaudo DJ, Connolly SM. Neutrophilic dermatosis (pustular vasculitis) of the dorsal hands: a report of 7 cases and review of the literature. Arch Dermatol 2002; 138: 361–365.
- Cohen PR. Skin lesions of Sweet syndrome and its dorsal hand variant contain vasculitis: an oxymoron or an epiphenomenon? Arch Dermatol 2002; 138: 400–403.
- Walling HW, Snipes CJ, Gerami P, Piette WW. The relationship between neutrophilic dermatosis of the dorsal hands and sweet syndrome: report of 9 cases and comparison to atypical pyoderma gangrenosum. Arch Dermatol 2006; 142: 57–63.
- Micallef D, Bonnici M, Pisani D, Boffa MJ. Neutrophilic dermatosis of the dorsal hands: A review of 123 cases. J Am Acad Dermatol 2023; 88: 1338–1344.
- Hoverson AR, Davis MD, Weenig RH, Wolanskyj AP. Neutrophilic dermatosis (Sweet syndrome) of the hands associated with lenalidomide. Arch Dermatol 2006; 142: 1070–1071.
- Wolf R, Barzilai A, Davidovici B. Neutrophilic dermatosis of the hands after influenza vaccination. Int J Dermatol 2009; 48: 66–68.
- Gloor AD, Feldmeyer L, Borradori L. Neutrophilic dermatosis of the dorsal hands triggered by mechanical trauma. J Eur Acad Dermatol Venereol 2021; 35: e20–e21.
- Tintle S, Patel V, Ruskin A, Halasz C. Azacitidine: a new medication associated with Sweet syndrome. J Am Acad Dermatol 2011; 64: e77–e79.
- Trickett HB, Cumpston A, Craig M. Azacitidine-associated Sweet’s syndrome. Am J Health Syst Pharm 2012; 69: 869–871.
- Passe M, Lepelletier C, Vignon-Pennamen MD, Chasset F, Hirsch P, Battistella M, et al. Next-generation sequencing in myeloid neoplasm-associated Sweet’s syndrome demonstrates clonal relation between malignant cells and skin-infiltrating neutrophils. J Invest Dermatol 2020; 140: 1873–1876.e5.
- Delaleu J, Kim R, Zhao LP, de Masson A, Vignon-Pennamen MD, Cassius C, et al. Clinical, pathological, and molecular features of myelodysplasia cutis. Blood 2022; 139: 1251–1253.
- Calvo KR. Skin in the game: the emergence of myelodysplasia cutis. Blood 2022; 139: 1132–1134.