ORIGINAL REPORT
“Tattoo Characteristics and Testing for Body Dysmorphic Disorder: An Internet-based Self-questionnaire Survey of 4,809 Individuals with Tattoos”
Justyna PUTEK1, Aleksandra BATYCKA-BARAN2, Jacek C. SZEPIETOWSKI2 and Wojciech BARAN2
1Student Research Group of Experimental Dermatology, Institute and Department of Dermatology, Venereology and Allergology and 2Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Wroclaw, Poland
Tattoos have become very popular worldwide in recent years. The aim of this study was to analyse a group of people interested in having tattoos, and screen them for body image disturbances. This cross-sectional self-administered internet-based survey included 4,809 individuals interesting in having tattoos. The majority of the study population were female (79.1%). The survey was conducted using a self-created questionnaire and the Body Dysmorphic Disorder Questionnaire – Dermatology version. Most tattoos in the study group were located on the forearms and hands (28.1%). The most popular motifs were plants (17.5%) and animals (16.9%). Out of 4,809 individuals, 19.9% had problems with acceptance of some parts of their body and 9.8% were screened for body dysmorphic disorder with the Body Dysmorphic Disorder Questionnaire – Dermatology version. Four percent of individuals reported that tattoos helped to improve their own perception of the appearance of their body by distracting attention from the other problems. Limitations of this study include possible participant selection bias and the overrepresentation of women. In conclusion, clinicians may expect to see more patients with tattoos and, of these, approximately 10% may be screened for body dysmorphic disorder.
Key words: body dysmorphic disorder; tattoos; tattoo motifs.
SIGNIFICANCE
The aim of this study was to analyse individuals interested in having tattoos and screen them for body image disturbances. The study was based on an internet-based survey, conducted on 4,809 individuals from Poland. Information about tattoo location, the most popular tattoo motifs, and the reasons for getting tattoos was analysed. The study group was also screened for body dysmorphic disorder (BDD). Clinicians see increasing numbers of patients with tattoos. This study indicates that almost 10% of them may be positively screened for body dysmorphic disorder.
Citation: Acta Derm Venereol 2024; 104: adv12444. DOI https://doi.org/10.2340/actadv.v104.12444.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Submitted: May 4, 2023; Accepted: Sep 12, 2023; Published: Feb 27, 2024
Corr: Aleksandra Batycka-Baran, Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Wroclaw, Poland, Chalubinskiego 1, PL-50-368 Wroclaw, Poland. E-mail: ola.batycka@interia.pl
Competing interests and funding: The authors have no conflicts of interest to declare.
Wroclaw Medical University SUBZ.C260.23.041.
INTRODUCTION
Humans have used tattoos as body art for at least 5,000 years (1). In recent years tattoos have become very popular worldwide. Familiarity with this type of body art in a socio-demographic context will result in improved healthcare provision. The aims of this study were to characterize tattoos among people interesting in having tattoos, recognize the reasons for getting a tattoo(s), and screen subjects for body image disturbances.
MATERIALS AND METHODS
This was a self-administered internet-based cross-sectional survey of 4,809 individuals from Poland (3,805 (79.1%) females, 1,004 (20.9%) males, age range 14–65 years (mean age ± standard deviation (SD) 27 ± 7.97 years). The survey was conducted using a self-created questionnaire (Fig. 1). This self-administered questionnaire (SAQ) was posted on Facebook groups for people interested in having tattoos. Respondents also completed the Body Dysmorphic Disorder Questionnaire – Dermatology version (BDDQ-DV) supplemented with some questions concerning tattoos. The BDDQ-DV was created by Phillips et al. (2) from Brown University School of Medicine, Rhode Island, USA. It is a screening tool that helps to diagnose patients with body dysmorphic disorder (BDD) (2, 3). The questionnaire is self-reported; therefore it can be used in daily clinical practice as well as in internet-based surveys.

Fig. 1. Self-administered questionnaire.
Respondents were asked if they are very concerned about the appearance of some part of their body that they considered to be especially unattractive. Those who answered “Yes” were further asked whether these concerns preoccupy them (i.e. if they are thinking about them a lot and they are difficult to stop thinking about). Respondents were further asked what these concerns are and what particularly bothers them about the appearance of these body parts, as well as what effect their preoccupation with their appearance has on their life. To diagnose patient for BDD, the individual should report the presence of concerns with the appearance of some part of their body as well as preoccupation with these concerns. The additional criterion is that the defect should at least moderately cause a lot of distress, torment or pain or should at least moderately impair their social, occupational and other important area(s) of functioning (be rated at least 3 on a 5-level Likert scale). The BDDQ-DV was supplemented with questions concerning tattoos. Those respondents who were positively screened for BDD were further asked if they intended for their tattoo(s) to draw attention away from this perceived defect.
Statistical analysis
Statistical analysis was performed using the software Microsoft Excel (Microsoft 365, USA) and XLMiner Analysis ToolPak (Version 2.0.0.0., Microsoft, USA).
Means and SDs were calculated for all variables. Differences between groups were determined using Student’s t-test. Statistical significance was set at p < 0.05. The data were collected and analysed anonymously.
RESULTS
Study group characteristics
The survey was completed by 4,809 individuals. Of the respondents 3,805 (79.1%) were women and 1,004 (20.9%) were men, age range 14–65 years (mean ± SD 27 ± 7.97 years). 52.8% (2,538) had secondary education, 23.5% (1,129) had graduated from university, 16.7% (804) were university students, and 7.1% (338) had primary education.
Tattoo characteristics
Number of tattoos. Of the respondents, 881 (18.3%) had 1 tattoo, 795 (16.5%) 2 tattoos, 698 (14.5%) 3 tattoos, 498 (10.4%) 4 tattoos, 1,355 (28.3%) 5–10 tattoos, and 569 (11.9%) 11 and more tattoos.
Age of getting first tattoo. Of the respondents, 1,190 (24.7%) got their first tattoo at age 18 years, 502 (10.4%) at age 17 years, 474 (9.9%) at age 19 years, 384 (8%) at age 16 years, 1,487 (31%) between 20 and 29 years, 421 (8.6%) between 30 and 39 years, 234 (4.9%) between 12 and 15 years, and 117 (2.2%) between 40 and 58 years (Fig. 2). The location of tattoos is shown in Fig. 3.
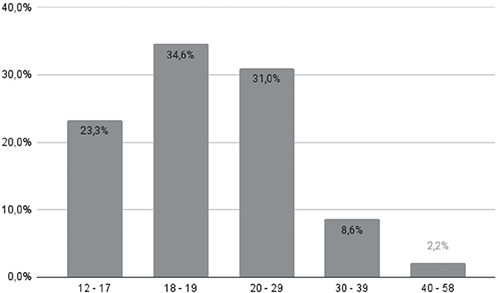
Fig. 2. Age of getting first tattoo.
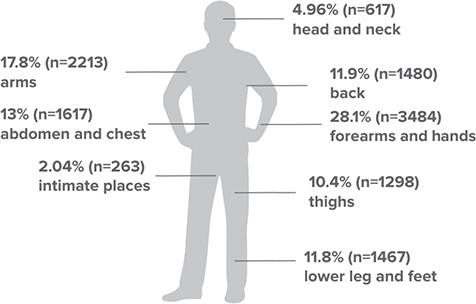
Fig. 3. Body location of tattoos.
Tattoo motifs. Of the motifs depicted in the tattoos, 2,270 (17.5%) were plants, 2,199 (16.9%) were animals, 2,098 (16.2%) were symbols, 1,890 (14.6%) were inscriptions, 989 (7.6%) had a mythical motif, 732 (5.7%) had a motif connected to death, 650 (5%) had a feminine motif, 600 (4.6%) a geometrical motif, 278 (2.2%) a musical motif, 253 (2%) a religious motif, 201 (1.6%) were tribal motifs, 99 (0.8%) had a patriotic motif, 8 (0.1%) were zodiac signs, and 691 (5.2%) had other motifs.
Reasons for getting tattoos. Of the respondents, 2,586 (20.6%) reported that they got a tattoo to express their personality, 1,825 (14.5%) felt more confident with a tattoo, 1,493 (11.9%) did it for aesthetic reasons, 1,459 (11.6%) to express their feelings and emotions, 1,211 (9.6%) to commemorate important events, 943 (7.5%) to commemorate loved ones, 722 (5.8%) to distinguish themselves, 491 (3.9%) to have the same tattoo as other person, 432 (3.4%) to cover scars, 95 (0.8%) because of a trend, and 65 (0.5%) for religious reasons. For 1,064 (8.5%) subjects getting a tattoo was a spontaneous decision, and 172 (1.4%) did it for other reasons (Fig. 4).
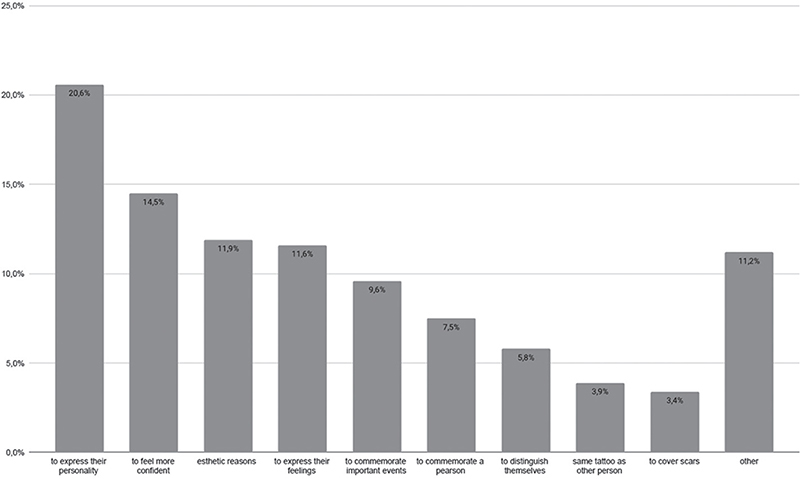
Fig. 4. Reasons for getting a tattoo.
Future plans. Of the respondents, 4,739 (98.5%) did not regret getting a tattoo, while 70 (1.5%) would not do it again. Of the respondents, 4,712 (98%) were willing to have a new tattoo in the future; however, 97 (2%) did not plan to have a new tattoo in the future. A total of 255 (5.3%) respondents had removed or planned to remove 1 of their tattoos; nevertheless, 4,554 (94.7%) subjects did not wish to remove a tattoo.
Screening for body image disturbances
The survey revealed that 956 respondents (19.9% of all respondents) were very concerned about some part of their body that they considered especially unattractive. Those respondents who answered “Yes” to this question were further asked what were these concerns. It was possible to give more than 1 answer to this question. The majority of subjects replied that the part of the body they were concerned about was too large (n = 601), that the skin in this location had scars or hyperpigmentation (n = 304) and that the part of the body was crooked or mis-shaped (n = 198). Other answers to this question were: that the part of the body was too small (n = 74), had stretch marks (n = 4), that the hair in this region bothered them (n = 2), that they had acne (n = 2), psoriasis (n = 2), cellulite (n = 1), an unidentified skin condition (n = 1) or alopecia (n = 1).
Of respondents, 562 (11.7%) additionally reported being preoccupied by this defect/problem. Those respondents were further asked whether the problem/defect caused a lot of distress, torment or pain and what was its severity on a 5-level Likert scale: 80 (1.7%) reported none and 35 (0.7%) mild, 227 (4.7%) subjects reported moderate, but still manageable, distress, 201 (4.2%) severe and very disturbing distress, and 19 (0.4%) extreme and disabling distress. Subjects then reported how this problem/defect impairs their social life, work and other important areas of life: 110 (2.3%) respondents reported no limitation, 163 (3.4%) reported that the interference was mild, but overall the performance was not impaired, 184 (3.8%) reported moderate and definite interference, which was still manageable, 88 (1.8%) reported that interference was severe and caused substantial impairment and 17 (0.4%) individuals reported that the interference was extreme and incapacitating.
Individuals were further asked if their perceived defect often significantly interfered with their social life; 341 (7.1%) answered “Yes” and gave examples. It was possible to give more than 1 answer to this question. Subjects were ashamed of this part of their body and felt unconfident (n = 322), had problems meeting new partners (n = 117), had difficulties meeting new people (n = 92) or were not willing to meet their friends very often (n = 64). Moreover, 76 (1.6%) respondents reported that their defect significantly interfered with their school, work, job or ability to function in their role. A total of 465 (9.7%) individuals answered that they avoided some things because of their defect.
Of respondents 470 (9.8%) were screened for BDD according to the BDDQ-DV. This group comprised 445 (94.7%) women and 25 (5.3%) men, age range 16–50 years (mean ± SD 24.6 ± 7.3 years).
In the group who completed the BDDQ-DV, 93 (19.8%) individuals had 1 tattoo (vs 18.3% in the whole group; p > 0.05), 93 (19.8%) had 2 tattoos (vs 16.5% in the whole group; p > 0.05), 84 (17.9%) 3 tattoos (vs 14.5% in the whole group; p > 0.05), 50 (10.6%) 4 tattoos (vs 10.4% in the whole group; p > 0.05), 115 (24.5%) 5–10 tattoos (vs 28.3% in the whole group; p > 0.05) and 35 (7.4%) more than 11 tattoos (vs 11.9% in the whole group; p < 0.05).
Furthermore, in this group 342 (33.8%) tattoos were situated on the forearms and hands (vs 28.1% in the whole group; p > 0.05), 158 (15.6%) on abdomen and chest (vs 13% in the whole group; p > 0.05), 132 (13.1%) on lower leg and feet (vs 11.8% in the whole group; p > 0.05), 124 (12.3%) on thighs (vs 10.4% in the whole group; p > 0.05), 116 (11.5%) on back (vs 11.9% in the whole group; p > 0.05), 60 (5.9%) on head and neck (vs 4.96% in the whole group; p > 0.05), 49 (4.8%) on arms (vs 17.8% in the whole group; p < 0.05) and 30 (3%) on intimate places (vs 2.04% in the whole group; p > 0.05). Regarding motifs, 20.2% (n = 240) of tattoos had plant motifs (vs 17.5% in the whole group; p > 0.05), 18.7% (n = 222) animal motifs (vs 16.9% in the whole group; p > 0.05), 17.1% (n = 203) were symbols (vs 16.2% in the whole group; p > 0.05), 15.7% (n = 187) were inscriptions (vs 14.6% in the whole group; p > 0.05), 6.9% (n = 82) had mythical motifs (vs 7.6% in the whole group; p > 0.05), 5.6% (n = 66) had feminine motifs (vs 5% in the whole group; p > 0.05), 5.2% (n = 62) geometrical motifs (vs 4.6% in the whole group; p > 0.05), 5.2% (n = 62) had motifs connected to death (vs 5.7% in the whole group; p > 0.05), 2.3% (n = 28) had musical motifs (vs 2.2% in the whole group; p > 0.05), 1.5% (n = 18) had tribal motifs (vs 1.6% in the whole group; p > 0.05), 1.3% (n = 16) had religious motifs (vs 2% in the whole group; p < 0.05) and 0.3% (n = 3) had patriotic motifs (vs 0.8% in the whole group; p < 0.05).
Regarding the reasons for getting tattoos in the group of individuals screened positively for BDD, 18.5% (n = 245) of subjects reported that they got a tattoo to express their personality (vs 20.6% in the whole group; p > 0.05), 16.5% (n = 220) felt more confident due to a tattoo (vs 14.5% in the whole group; p < 0.05), 13.1% (n = 175) got a tattoo for aesthetic reasons (vs 11.9% in the whole group; p < 0.05), 12.9% (n = 171) wanted to express their feelings and emotions (vs 11.6% whole group; p < 0.05), 8.2% (n = 110) to commemorate important events (vs 9.6% in the whole group; p > 0.05), for 8.2% (n = 110) subjects it was a spontaneous decision (vs 8.5% in the whole group; p > 0.05), 6.5% (n = 87) wanted to commemorate loved ones (vs 7.5% in the whole group; p > 0.05), 5.7% (n = 76) wanted to distinguish themselves (vs 5.8% in the whole group; p > 0.05), 4.9% (n = 65) wanted to cover scars (vs 3.4% in the whole group; p < 0.05), 4.6% (n = 62) wanted to have the same tattoo as another person (vs 3.9% in the whole group; p > 0.05), 0.8% (n = 11) had a tattoo because of a trend (vs 0.8% in the whole group; p > 0.05) and 0.1% (n = 2) for religious reasons (vs 0.5% in the whole group; p < 0.05). A total of 190 (4.0%) respondents reported that they got a tattoo to distract attention from their from their perceived body defect. In this group of respondents, 456 (97%) did not regret getting a tattoo (vs 98.5% in the whole group; p > 0.05) and 466 (99%) individuals wanted to have a new tattoo in the future (vs 98% in the whole group; p < 0.05). Finally, 431 (91.7%) respondents had no desire to remove a tattoo (vs 94.7% in the whole group; p < 0.05).
DISCUSSION
In the 1950s and 1960s tattoos were not regarded positively, and were found mainly among sailors, criminals or other marginal groups. However, tattoos are currently very popular among people in generation X and Millennials. The prevalence of tattoos is increasing in all social groups. The worldwide prevalence of tattoos is reported to range from 10% to 20% (1, 4–6)
In the past, tattoos were more common in men than women, but this is no longer the case (6). In some studies the incidence of tattoos is equal in both sexes (6) and in other studies (5), women are more likely to be tattooed. In the current survey 79.1% of respondents were female; however, we assume that this may be because females are more likely than males to complete online questionnaires.
According to Quaranta et al. (7) 36.1% of adolescents get a tattoo without informing their parents or gaining their consent. In the current study 1,120 (23.3%) of respondents got their first tattoo when they were juveniles. The most common age of getting a first tattoo was 18 years (24.7%), which is presumably related to reaching legal age at this point in Poland. Most subjects (81.6%) had more than 1 tattoo and 40.2% had more than 5 tattoos. At the same time, 98% of subjects wanted to get another tattoo in the future, hence the number of tattoos among respondents is expected to increase in the coming years.
According to Heywood et al. (8) tattoos are, to some extent, associated with people with low socioeconomic or educational status. However, in the current study the majority (52.8%) of respondents had finished high school and 40.2% of subjects had higher education degrees or would gain them soon. This may indicate that tattoos have become more popular in all social and educational groups. Understanding the motivations for getting a tattoo helps us to gain information about individuals. In the current survey most subjects got a tattoo to express their personality, strengthen their self-esteem and demonstrate their feelings and emotions, and only 1.5% of respondents regretted getting a tattoo. Nonetheless, these rates are higher in other studies, ranging from 14% to 4.9% (5, 9, 10).
Body image disturbances are considered as general dissatisfaction or distress about the body or a part of the body image, associated with impairment in quality of life (11). Cash et al. (12) suggested that there may be a spectrum of psychological disturbances, where the less severe cases may be considered as body image dissatisfaction and more severe ones may be diagnosed as BDD. BDD is a common psychiatric disorder, which consists in distressing and impairing preoccupation with one’s own appearance, in particular with an imagined/non-existent or slight defect usually regarding the skin or body build (2, 3, 13, 14). Constant thoughts about imperfections causes misery among patients and leads to problems in social and work life. BDD is often associated with depression, addictive disorders, obsessive compulsive disorders, or even suicide (14, 15).
In the current study 19.9% of respondents had problems with acceptance of some parts of their body and 11.7% reported being preoccupied with their perceived defect. In this survey 9.8% of individuals were screened for BDD according to the BDDQ- DV. There is a lack of research concerning the association between getting tattoos and the prevalence of BDD. According to Kertzman et al. (16) young women with tattoos have significantly lower self-esteem than women without tattoos. Tattoos are used to improve self-esteem through creating “a perfect” body image (16). Kertzman et al. (16) found that the tattooed group displayed a much greater discrepancy between their present body and the ideal body than women without tattoos. In the current study 4.0% of individuals reported that tattoos help to improve perception of the appearance of their body by distracting attention from the real problem. According to the literature, the weighted prevalence of BDD in a community sample is approximately 2% and it is higher in student populations (2.2%) and psychiatric patients (7.4%) (17, 18). The prevalence of BDD among patients visiting dermatologists is significantly higher and has been reported as 4.9%, 10.5%, 11.3% and 14.1% (19–22). The current study showed that, in the group of respondents screened for BDD, fewer tattoos were situated on the arms and they were less likely to have religious and patriotic motifs. Furthermore, individuals screened for BDD statistically more often reported that they got their tattoo to feel more confident, to improve their appearance, to express their feelings and emotions, or to cover scars. The majority of subjects did not regret getting a tattoo. However, in the group who screened positively for BDD, statistically more respondents had a desire to remove tattoos, but they were also more willing to get a new tattoos in the future.
The current study was based on a self-administered internet questionnaire. The study limitations include participant selection bias, possible misunderstanding of the questions, and overrepresentation of women; therefore the results might be more accurate for female patients interesting in tattooing. However, despite these limitations, the study was conducted on a large number of subjects (n = 4,809), hence we consider that reliable conclusions can be drawn. Clinicians will see increasing numbers of patients with tattoos. An holistic approach means that physicians should be aware of self-acceptance problems occurring among these patients.
REFERENCES
- Deter-Wolf A, Robitaille B, Krutak L, Galliot S. The world’s oldest tattoos. J Archaeol Sci Rep 2016; 5: 19–24.
- Phillips KA, Dufresne RG, Wilkel CS, Vittorio CC. Rate of body dysmorphic disorder in dermatology patients. J Am Acad Dermatol 2000; 42: 436–441.
- Danesh M, Beroukhim KO, Nguyen C, Levin E, Koo J. Body dysmorphic disorder screening tools for the dermatologist: a systematic review. Pract Dermatol 2015; 2: 44–49.
- Laumann AE, Derick AJ: Tattoos and body piercings in the United States: a national data set. J Am Acad Dermatol 2006; 55: 413–421.
- Kluger N. Epidemiology of tattoos in industrialized countries. Curr Probl Dermatol 2015; 48: 6–20.
- Lahousen T, Linder MD, Gieler U, Hofmeister D, Trapp EM, Borkenhagen A, et al. Body modification in Germany: prevalence, gender differences and attitude towards cosmetic surgery. G Ital Dermatol Venereol 2019; 154: 646–649.
- Quaranta A, Napoli C, Fasano F, Montagna C, Caggiano G, Montagna MT. Body piercing and tattoos: a survey on young adults’ knowledge of the risks and practices in body art. BMC Public Health 2011; 11: 774.
- Heywood W, Patrick K, Smith AM, Simpson JM, Pitts MK, Richters J, et al. Who gets tattoos? Demographic and behavioral correlates of ever being tattooed in a representative sample of men and women. Ann Epidemiol 2012; 22: 51–56.
- Braverman, S. One in five US adults now has a tattoo. The Harris Poll 2012; 22: 1–6.
- Klügl I, Hiller KA, Landthaler M, Bäumler W. Incidence of health problems associated with tattooed skin: a nation-wide survey in German-speaking countries. Dermatology 2010; 221: 43–50.
- Callaghan GM, Duenas JA, Nadeau SE, Darrow SM, Van der Merwe J, Misko J. An empirical model of body image disturbance using behavioral principles found in functional analytic psychotherapy and acceptance and commitment therapy. Int J Behav Consult Ther 2012; 7: 16–24.
- Cash TF, Theriault J, Annis NM. Body image in an interpersonal context: Adult attachment, fear of intimacy, and social anxiety. J Soc Clin Psych 2004; 23: 89–103.
- Phillips KA, Wilhelm S, Koran LM, Didie ER, Fallon BA, Feusner J, et al. Body dysmorphic disorder: some key issues for DSM-V. Depress Anxiety 2010; 27: 573–591.
- F. Krebs G, Fernández de la Cruz L, Mataix-Cols D. Recent advances in understanding and managing BDD. Evid Based Ment Health 2017; 20: 71–75.
- G. Phillips KA, Siniscalchi JM, McElroy SL. Depression, anxiety, anger, and somatic symptoms in patients with body dysmorphic disorder. Psychiatr Q 2004; 75: 309–320.
- Kertzman S, Kagan A, Hegedish O, Lapidus R, Weizman A. Do young women with tattoos have lower self-esteem and body image than their peers without tattoos? A non-verbal repertory grid technique approach. PLoS One 2019; 14: e0206411.
- Danesh M, Beroukhim K, Nguyen C, Levin E, Koo J. Body dysmorphic disorder screening tools for the dermatologist: a systematic review. Pract Dermatol 2015; 2: 44–49.
- Hardardottir H, Hauksdottir A, Bjornsson AS. Body dysmorphic disorder: symptoms, prevalence, assessment and treatment. Laeknabladid 2019; 105: 125–131.
- Brohede S, Wyon Y, Wingren G, Wijma B, Wijma K. Body dysmorphic disorder in female Swedish dermatology patients. Int J Dermatol 2017; 56: 1387–1394.
- AlShahwan MA. Prevalence and characteristics of body dysmorphic disorder in Arab dermatology patients. Saudi Med J 2020; 41: 73–78.
- Veale D, Gledhill LJ, Christodoulou P, Hodsoll J. Body dysmorphic disorder in different settings: a systematic review and estimated weighted prevalence. Body Image 2016; 18: 168–186.
- Schut C, Dalgard FJ, Bewley A, Evers AWM, Gieler U, Lien L, et al. ESDAP Study collaborators. Body dysmorphia in common skin diseases: results of an observational, cross- sectional multicentre study among dermatological out-patients in 17 European countries. Br J Dermatol 2022; 187: 115–125.