ORIGINAL REPORT
Incidence of Dermatitis Herpetiformis in Sweden 2005 to 2018: A Nationwide Retrospective Cohort Study
Zeyad ALBADRI1, Doua AL BAYATI1, Henrike HÄBEL2, Sandra JERKOVIC GULIN1,4, Carina GRÖNHAGEN3 and Oliver SEIFERT1
1Department of Clinical and Experimental Medicine, Faculty of Health Sciences, Linköping University, Linköping, 2Medical Statistics Unit, Department of Learning, Informatics, Management and Ethics, Karolinska Institutet, Stockholm, 3Department of Dermatology, Lund University, Skåne University Hospital, Malmö and 4Division of Dermatology and Venereology, Region Jönköping County, Jönköping, Sweden
Dermatitis herpetiformis has been investigated in the past; however, only a limited number of studies have reported its incidence based on validated nationwide population-based registries. To address this gap, the aims of this study are to estimate the incidence of dermatitis herpetiformis in Sweden and to validate the National Patient Register (NPR) for diagnosis of dermatitis herpetiformis. A population-based open cohort study was conducted, including all patients diagnosed with dermatitis herpetiformis (International Classification of Diseases 10th revision; ICD-10 code L13.0) in Sweden from 2005 to 2018 (n = 1,724), identified from the NPR. The diagnosis of dermatitis herpetiformis in the NPR was validated using medical records, histopathological and immunopathological data, yielding a positive predictive value (PPV) of 62.5%. The mean annual incidence of dermatitis herpetiformis was 0.93/100,000 (95% confidence interval 0.79–1.08), female to male ratio 1:1, and mean age at diagnosis 60.9 years. In conclusion, this large nationwide cohort study showed a low validity for diagnosis of dermatitis herpetiformis in the NPR, and the adjusted incidence rate of dermatitis herpetiformis in Sweden was estimated to be 0.93/100,000, which is lower than that in previous Swedish studies.
Key words: incidence; dermatitis herpetiformis; population-based cohort study; healthcare registries; medical records.
SIGNIFICANCE
This study reveals important findings regarding the incidence of dermatitis herpetiformis in Sweden as well as the accuracy of the Swedish National Patient Register. The incidence of dermatitis herpetiformis in Sweden is 0.93 per 100,000 inhabitants and the study indicates that dermatitis herpetiformis is more common among the elderly population. The incidence rate for women was significantly higher in the age range 30–49 years, while men had a significantly higher incidence rate for those aged 60 years or older. Information on dermatitis herpetiformis in the National Patient Register is not comprehensive, and miscoding of International Classification of Diseases 10th revision (ICD-10) codes has to be taken into account.
Citation: Acta Derm Venereol 2023; 103: adv13210. DOI https://doi.org/10.2340/actadv.v103.13210.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/)
Accepted: Oct 19, 2023; Published: Nov 16, 2023
Corr: Oliver Seifert, Department of Clinical and Experimental Medicine, Faculty of Health Sciences, Linköping University, SE-581 83, Linköping, Sweden. E-mail: oliver.seifert@liu.se
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Dermatitis herpetiformis (DH) is a bullous skin disorder clinically recognized by an itching, blistering rash with predilection sites on the elbows, knees and buttocks. DH is the most common extraintestinal manifestation of coeliac disease (CD). Both DH and CD have a similar genetic background; notably, the human leukocyte antigen (HLA) pattern HLA-DQ2 and HLA-DQ8 haplotypes are predisposing factors (1).
In CD, tissue transglutaminase (TG2) is the primary autoantigen targeted by IgA antibody responses, and epidermal transglutaminase (TG3) has been identified as the autoantigen for DH (2). Plasma cells in the small bowel generate IgA-TG3 autoantibodies, which become part of circulating immune complexes closely linked to the presence of TG3 enzyme in the dermal deposits (3, 4). DH is differentiated from other bullous skin disorders by the occurrence of granular IgA deposits in the papillary dermis using direct immunofluorescence (DIF) (1, 5). DIF of perilesional skin is considered the gold standard for diagnosing DH. However, if DIF results are negative, DH can also be diagnosed using histopathology, serology and clinical presentation (6).
The treatment of choice for patients with DH is a lifelong gluten-free diet (GFD) to which they respond well. However, it takes 1–2 years to relieve the cutaneous symptoms of DH with a GFD alone. Therefore, dapsone is administered until the GFD is fully effective on its own. (7). Dapsone treatment results in such rapid improvement that responsiveness to treatment has been used as a diagnostic tool (8). Response to dapsone is confirmative of DH (9).
The incidence of DH varies among different countries worldwide (10–14). DH is more common among individuals from North America and of northern European descent, while it is very rare in individuals of Asian and African descent (10, 15–17). Most studies assessing this subject were made a long time ago (1972 to 1992), showing that incidence rates in Europe and North America varied between 0.4 and 2.6 per 100,000 (12, 13, 18–20). Recent studies published in 2011, 2014 and 2017 have reported incidence rates of 3.5, 0.8 and 1.2 per 100,000, respectively (10, 11, 21).
DH typically occurs in individuals aged between 40 and 50 years, though it can occur at any age (1). It is slightly more common in males than females, with a ratio of 1.36:1–2:1 (22–24). There have, however, been some studies that have reported ratios that are near equal (10, 11).
In Sweden, all permanent residents are given a unique personal identity number (PIN) from the Swedish National Board of Health and Welfare (NBHW). It is through the PIN that medical records are linked to individual patients. Furthermore, the PIN allows for the maintenance and management of multiple registries in Sweden (25). Since 1964, the National Patient Register (NPR), held by the NBHW, has recorded data on visits to inpatient care units. The register has provided full coverage on inpatient care since 1987 and started to include specialized outpatient care in 2001. Coverage for outpatient care in the NPR between 2001 and 2018 has been 87% (26). The register does not include any data from primary care units. The NPR provides information such as patients’ PIN, sex, age, county of residence and medical information, which, in turn, facilitates the conducting of nationwide epidemiological studies (26, 27). The medical information provided in the NPR, such as diagnosis and medical interventions, is coded using the ICD-10. Overall, the NPR is considered to have high validity for many diagnoses (27). The specific diagnosis of DH, however, has not yet been validated.
This study aims to evaluate the NPR’s validity for DH diagnosis and to determine the incidence of DH in Sweden.
MATERIALS AND METHODS
Study design
In this nationwide, retrospective cohort study, anonymized data on all patients that received a diagnosis of DH between 1990 and 2018 was obtained from the NBHW. The data contained patient information regarding sex, age, and year of diagnosis. Only data from 2005 and onwards were included in the study. That is because the outpatient register started in 2001, and, during 2001 to 2004, the NPR included all patients with previously diagnosed DH, leading to unusually high numbers of DH cases in those years. However, the number of new cases registered in the NPR began to stabilize in 2005, and new registrations from that point on were considered true incident cases. All patients diagnosed with DH as a primary or secondary diagnosis, in 2005 to 2018, using the ICD-10 code L13.0, were included. The patients were only included the first time they received the diagnosis of DH. After having identified our incident cases, they were stratified by sex and age (10-year age bands: 0–9, 10–19, …, 70–79, and 80+ years for all patients over 80 years).
Information on the Swedish population (number of inhabitants stratified by sex, age, and year) was obtained from the database Statistics Sweden (www.scb.se). This information allowed the current study to relate the incident cases to the general population. The entire Swedish population, 2005 to 2018, was considered at risk (n = 9,439,884) when this study estimated the age- and sex-specific incidence rates. DH incidence was estimated by dividing the mean number of cases diagnosed from 2005 to 2018 by the mean background population during the corresponding years.
Validation of the National Patient Register
All patients diagnosed with DH living in Västerbotten and Örebro, 2 of the total 21 counties in Sweden, were included for the validation calculation. These counties were chosen because they reflect diverse geographical locations and differences in population density across Sweden.
The number of patients diagnosed with DH in those counties in 2005 to 2018 were retrieved from the NPR. Each dermatology department was requested to provide the medical records of patients diagnosed with DH using the ICD-10 code L13.0. Two dermatologists manually reviewed the medical records.
The gold-standard laboratory procedure for diagnosis of DH is DIF. In this study, the diagnosis of DH was confirmed if a positive DIF was registered in the medical records. Cases with typical clinical manifestations, but negative DIF microscopy results were classified as DH cases if they at least presented 2 of the minor criteria according to the consensus-based guidelines (S2k-guidelines) published in 2021 (6). These minor criteria are a positive serological test, a histopathological examination compatible with DH, fast response to dapsone treatment, response to GFD, duodenal biopsy with evidence for CD, HLA testing compatible with DH or positive iodine patch test or oral iodine challenge. Validation findings were used to adjust the incidence rates.
Sensitivity analysis
A sensitivity analysis was conducted to adjust the incidence rate estimate accuracy (Table I). Using the validation results from Västerbotten and Örebro, the results were then statistically generalized to the entire country.
Ethics
The Regional Ethical Review Board in Stockholm and in Linköping approved this study (2013/1146-31, 2014/79-32, 2014-1637-32, 2020-01592).
Statistical analysis
To compare means between groups, numerical variables were analysed using the Student’s t-test and categorical variables were analysed with the χ2 test. Age- and sex-specific incidence rates were estimated by dividing the number of cases for the specific age group by the total population in that age group per 100,000 inhabitants and 95% confidence intervals (95% CI) according to Poisson normal approximation. Two-sided p-values are reported: a p-value of < 0.05 was considered as threshold for statistical significance. Due to the explorative nature of this study, no multiplicity adjustments were made. All statistical analyses were performed using IBM SPSS Statistics 27 for Windows (IBM Corp., Armonk, NY, USA).
RESULTS
In Västerbotten and Örebro, 160 patients were diagnosed with DH according to the NPR between 2005 and 2018. All patients were diagnosed at specialized outpatient care units. However, of 160 diagnosed patients according to the NPR, only 144 cases were registered and found in the medical journals of the 2 counties.
The reviewed medical journals revealed that 90 patients were correctly diagnosed with DH. There were 54 misdiagnosed cases and 16 unreviewable cases due to missing medical data. Common point imputation was applied to the missing data. Including all missing records as non-confirmed DH cases yields a PPV of 56.25% (90/160) and assuming all missing records as confirmed DH cases results in a PPV of 66.25% (106/160). The mean PPV (56.3 + 66.2)/2 = 61.25 %) suggests that 10 cases are expected to be true DH cases among the missing cases. As a result, 100 out of 160 patients were accurately diagnosed with DH, representing a PPV of 62.5% (Fig. 1).

Fig. 1. Flowchart of the patients included in the study population for the validation of dermatitis herpetiformis (DH) diagnosis in the Swedish National Patient Register (NPR). Based on data collected from the NPR, matched with the medical records retrieved from 2 counties, Örebro and Västerbotten; the positive predictive value (PPV) of all patients diagnosed with dermatitis herpetiformis (DH) (International Classification of Diseases revision 10; ICD-10 code L13.0) over the period 2005 to 2018 is 62.5%.
A total of 1,724 incident cases of DH were registered in Sweden between 2005 and 2018. Females accounted for 50.3% of those diagnosed. At the time of diagnosis, the mean age was 60.9 years (SD 18.7, range 1–102 years). The mean age at diagnosis for men was 64.8 (SD 15.5) years, and it was significantly older than the mean age of diagnosis for women, 57.1 (SD 20.8) years, p < 0.001. Most patients were diagnosed at an outpatient care setting (96.1%, n = 1,656), and the majority received their diagnosis from a dermatologist (81.3%, n = 1,401). DH was the primary diagnosis for 81.8% (n = 1,411) of the patients.
There were a mean of 123 cases of DH between 2005 and 2018; the number of cases ranged from 73 to 160 cases per year. During the corresponding years, the mean background population was 9,439,884. Thus, the mean annual incidence rate of DH was 1.3/100,000 (95% CI 1.1–1.5) (Fig. 2).
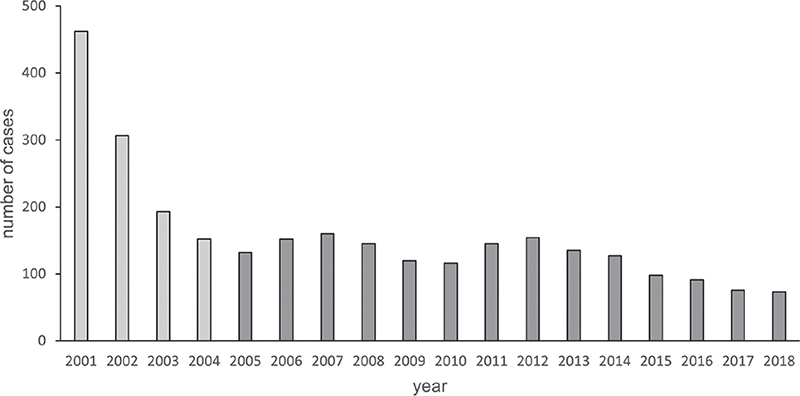
Fig. 2. The number of incident and prevalent cases of dermatitis herpetiformis (DH), 2001 to 2018, in Sweden based on data from the National Patient Register (NPR). The data includes patients diagnosed at both inpatient and outpatient care units. The light-coloured bars represent a mix of prevalent and incidence cases in the NPR and were excluded from the study. Patients of all ages, diagnosed with DH between 2005 and 2018, were included in the study (dark-coloured bars). The mean number of DH cases during those years was 123, by dividing it by the mean background population during that period (n = 9,439,884) the incidence rate was estimated. Incidence of DH in Sweden 2005 to 2018 were 123/9,439,884 = 1.3 cases/100,000 (95% confidence interval (95% CI) 1.1–1.5).
Table I shows the result of the sensitivity analysis. A standardized review of medical records was used to validate the diagnosis of DH in the NPR, which yielded a PPV of 62.5%. Taking the NPR coverage of inpatient and outpatient care into account, the adjusted incidence rate of DH is 0.93 per 100,000 inhabitants (95% CI 0.79–1.08).
During 2005 to 2018, patients in the age range 60–69 years were the most frequently diagnosed with DH (n = 329) (Fig. S1), whereas the peak incidence rate was observed among patients 80 years of age or older, 2.8/100,000 (95% CI 2.55–3.02) (Fig. 3a). The incidence of DH among paediatric patients was observed to be 0.3/100,000 during the first decade of life and 0.6/100,000 for those in the second decade of life (Fig. 3a and b).
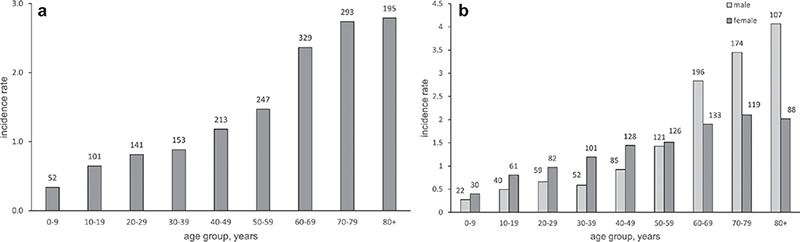
Fig. 3. (a) Age-specific and (b) age- and sex-specific incidence rate of dermatitis herpetiformis (DH) per 100,000 in Sweden, 2005 to 2018. To estimate the mean age-specific incidence rate of DH, the number of patients (number above the bars) in each age group were used and the incidence rates were adjusted to the Swedish population during the corresponding years.
The incidence rate peaked for men in the 80+ year age group with 4.1/100,000, while incidence peak for women was observed in the 70–79-year age group with 2.1/100,000 (Fig. 3b). The incidence rate for women were significantly higher between the ages 30 and 49 years, p < 0.001, while men had a significantly higher incidence rate for those aged 60 years or older, p < 0.001 (Table II).
DISCUSSION
This study found that the specific diagnosis of DH had a PPV of 62.5% in the NPR, which is low compared with other diagnoses in the NPR, which is renowned for its high validity (27). This suggests that DH is a rare diagnosis and that there is a risk of misdiagnosis.
The mean annual incidence of DH is estimated to be 0.93 per 100,000 inhabitants. Previous studies in Sweden reported an incidence of 0.89–1.45 for the years 1943 to 1982 in central Sweden (19) and an incidence of 1.1 for the years 1976 to 1981 per 100,000 in western Sweden (13). These findings indicate a decreasing incidence of DH in Sweden. A Finnish cohort study and a British register study have further confirmed this decreasing trend. Salmi et al. reported a decrease in the annual incidence from 5.2 to 2.7 per 100,000 between 1980 and 2009 (10), and another Finnish study reported an incidence of 1.2 per 100,000 between 2005 and 2014 (21). Between 1990 and 2011, West et al. reported a decrease in the incidence of DH from 1.82 to 0.8 per 100,000 in the UK (11).
In the meantime, both the UK and Finland reported an increase in the incidence of CD (11, 28) suggesting that the risk of developing DH decreases by finding patients with CD and treating them at an early stage of the disease (11). It is widely accepted that all patients with DH have gluten sensitivity (29) and it is proposed that subclinical and untreated CD is required to develop DH. A study confirmed that patients diagnosed with CD not adhering to GFD later develop DH (30). However, the development of serological markers as screening tests has facilitated the diagnosis of CD (31). Therefore, patients with subclinical CD can be diagnosed early and receive treatment with GFD and, thus, not develop DH (29, 32).
The incidence of DH varies worldwide. The incidence rate in Sweden (13, 19) is lower than in Finland (3.5 and 1.2 per 100,000) (10, 21), but higher than in the UK (0.8 per 100,000) (11). In comparison, Japan reported only 91 patients in the whole country over 35 years (23).
This study revealed that the incidence of DH increases with advancing age, reaching its peak among patients over 80 years of age. However, age at time of diagnosis peaked between 60 and 69 years of age. West et al. found the highest incidence rate among those between the ages 50 and 69 years. Regarding the incidence by sex, the highest incidence among men was also found among those aged 80 years or older. Women had the highest incidence rate a decade earlier. Salmi et al. (10) demonstrated that peak incidence rates in Finland were observed among men aged 60–69 years and women aged 50–59 years. This aligns with the finding of the current study, that women are affected by the disease earlier in life than men.
This study identified a total of 1,724 cases, with men and women being diagnosed at an equal ratio. Previous studies have demonstrated male predominance, ranging up to 2.1:1 (22–24, 33). This finding is backed up by Salmi et al., who found a male to female ratio of 1.1:1, and West et al., who also reported an almost equal sex distribution (10, 11). The reason behind the proportion differences found in different studies is unclear (10).
The mean age among the patients diagnosed with DH in Sweden was 60.9 years. Meanwhile, the mean ages reported in earlier studies are lower in European, American (10, 22, 33), and Asian countries (23, 24, 34), ranging between 32 and 53 years. Salmi et al. reported that the mean age of patients with DH increased from 35.8 to 48.6 years in Finland between 1970 and 2009 (10). This study suggested that, over the last decades in Finland, the annual consumption of wheat, rye, and other cereals per person has decreased by more than 50% (10). Therefore, one could suppose that a decreased gluten consumption postpones disease onset (10, 29) potentially elucidating the reason behind the higher age at diagnosis observed in the current study. However, diagnosing DH is not consistently straightforward and might lead to confusion with other subepidermal blistering conditions, such as bullous pemphigoid (BP), particularly among the elderly population. Cases of DH and BP exhibiting overlapping features have been documented in the past (35).
The paediatric incidence of DH in this study was found to be 0.3 per 100,000 for those in the first decade of life and 0.6 per 100,000 for those in the second decade of life, accounting for 8% of all diagnosed with DH. A study from Finland diagnosed 18 children (3.8%) with DH over a timeframe of 40 years (10) and reported a childhood incidence of 0.56 per 100,000 (36). By contrast, in an Italian case series of 159 patients collected between 1995 and 2012, the mean age was 32 years, and 36% of all diagnosed were under the age of 20 years (37). Their second case series confirmed their finding of a relatively high incidence among children in Italy, with 21.4% of 151 patients being under the age of 18 years (38). A large case series from Hungary, including 117 children with DH, have also been published (39). The incidence of paediatric DH seems to be higher in the southern parts of Europe compared with the northern parts (40). It is suggested that different patient recruitment practices among clinical centres, differences in dietary habits, or genetic variation may be responsible for the observed differences in DH occurring at young ages (38). However, HLA findings are similar in those populations, hence genetics is less likely to be the explanation (36). It is suggested that certain aspects influencing immunoregulation, such as endocrine or other sex-specific factors, could cause the noted age variations in DH (10).
Some strengths of this study include its nationwide coverage and its population-based setting reducing the risk of selection bias. Our large cohort and the long time-frame of 13 years also reduces the risk of selection bias as well as it allowed us to estimate an accurate incidence rate. The validation of the NPR for DH diagnosis included 2 dermatologists manually examining the patient records of 2 counties. This methodology allowed us to compare the medical data against data found in the NPR, thus allowing us to accurately detect discrepancies between the 2 sources.
This study also has some limitations, mainly due to the retrospective design of the study; the information that could be accessed for the patients diagnosed with DH was limited. The study analyses are influenced by the accuracy of the ICD-codes reported to the NPR. Therefore, we validated the NPR for the diagnosis of DH and later performed a sensitivity analysis in which we accounted for the PPV found for DH in the NPR. Data from primary healthcare is not included in the NPR, which means that patients who do not visit special care will not be included in the register. One noteworthy limitation in the current study that require consideration is the utilization of only 2 counties for NPR validation. This narrow scope may introduce bias and should be acknowledged when interpreting the results.
In conclusion, future epidemiological studies using the NPR to analyse DH should consider the low PPV. The annual incidence rate of DH in Sweden is declining, just as in some other countries.
The incidence rate of DH in Sweden increases with age and the highest incidence rate is observed among people in their 80s and older. This study indicates that, both men and women are equally affected by DH. Finally, the incidence of DH in young individuals seems to be lower in northern European countries compared with other countries in Europe.
REFERENCES
- Reunala T, Hervonen K, Salmi T. Dermatitis herpetiformis: an update on diagnosis and management. Am J Clin Dermatol 2021; 22: 329–338.
- Sardy M, Karpati S, Merkl B, Paulsson M, Smyth N. Epidermal transglutaminase (TGase 3) is the autoantigen of dermatitis herpetiformis. J Exp Med 2002; 195: 747–757.
- Sankari H, Hietikko M, Kurppa K, Kaukinen K, Mansikka E, Huhtala H, et al. Intestinal TG3- and TG2-specific plasma cell responses in dermatitis herpetiformis patients undergoing a gluten challenge. Nutrients 2020; 12: 467.
- Taylor TB, Schmidt LA, Meyer LJ, Zone JJ. Transglutaminase 3 present in the IgA aggregates in dermatitis herpetiformis skin is enzymatically active and binds soluble fibrinogen. J Invest Dermatol 2015; 135: 623–625.
- Collin P, Salmi TT, Hervonen K, Kaukinen K, Reunala T. Dermatitis herpetiformis: a cutaneous manifestation of coeliac disease. Ann Med 2017; 49: 23–31.
- Gorog A, Antiga E, Caproni M, Cianchini G, De D, Dmochowski M, et al. S2k guidelines (consensus statement) for diagnosis and therapy of dermatitis herpetiformis initiated by the European Academy of Dermatology and Venereology (EADV). J Eur Acad Dermatol Venereol 2021; 35: 1251–1277.
- Antiga E, Caproni M. The diagnosis and treatment of dermatitis herpetiformis. Clin Cosmet Investig Dermatol 2015; 8: 257–265.
- Wolf R, Matz H, Orion E, Tuzun B, Tuzun Y. Dapsone. Dermatol Online J 2002; 8: 2.
- Huber C, Trueb RM, French LE, Hafner J. Negative direct immunofluorescence and nonspecific histology do not exclude the diagnosis of dermatitis herpetiformis Duhring. Int J Dermatol 2013; 52: 248–249.
- Salmi TT, Hervonen K, Kautiainen H, Collin P, Reunala T. Prevalence and incidence of dermatitis herpetiformis: a 40-year prospective study from Finland. Br J Dermatol 2011; 165: 354–359.
- West J, Fleming KM, Tata LJ, Card TR, Crooks CJ. Incidence and prevalence of celiac disease and dermatitis herpetiformis in the UK over two decades: population-based study. Am J Gastroenterol 2014; 109: 757–768.
- Smith JB, Tulloch JE, Meyer LJ, Zone JJ. The incidence and prevalence of dermatitis herpetiformis in Utah. Arch Dermatol 1992; 128: 1608–1610.
- Mobacken H, Kastrup W, Nilsson LA. Incidence and prevalence of dermatitis herpetiformis in western Sweden. Acta Derm Venereol 1984; 64: 400–404.
- Hellier FF. The prevalence of dermatitis herpetiformis. Br J Dermatol 1972; 86: 437–438.
- Bolotin D, Petronic-Rosic V. Dermatitis herpetiformis. Part I. Epidemiology, pathogenesis, and clinical presentation. J Am Acad Dermatol 2011; 64: 1017–1024; quiz 1025–1016.
- Hall RP, Clark RE, Ward FE. Dermatitis herpetiformis in two American blacks: HLA type and clinical characteristics. J Am Acad Dermatol 1990; 22: 436–439.
- Shibahara M, Nanko H, Shimizu M, Kanda N, Kubo M, Ikeda M, et al. Dermatitis herpetiformis in Japan: an update. Dermatology 2002; 204: 37–42.
- Reunala T, Lokki J. Dermatitis herpetiformis in Finland. Acta Derm Venereol 1978; 58: 505–510.
- Moi H. Incidence and prevalence of dermatitis herpetiformis in a country in central Sweden, with comments on the course of the disease and IgA deposits as diagnostic criterion. Acta Derm Venereol 1984; 64: 144–150.
- Gawkrodger DJ, Blackwell JN, Gilmour HM, Rifkind EA, Heading RC, Barnetson RS. Dermatitis herpetiformis: diagnosis, diet and demography. Gut 1984; 25: 151–157.
- Virta LJ, Saarinen MM, Kolho KL. Declining trend in the incidence of biopsy-verified coeliac disease in the adult population of Finland, 2005–2014. Aliment Pharmacol Ther 2017; 46: 1085–1093.
- Rose C, Brocker EB, Zillikens D. Clinical, histological and immunpathological findings in 32 patients with dermatitis herpetiformis Duhring. J Dtsch Dermatol Ges 2010; 8: 265–270, 265–271.
- Ohata C, Ishii N, Hamada T, Shimomura Y, Niizeki H, Dainichi T, et al. Distinct characteristics in Japanese dermatitis herpetiformis: a review of all 91 Japanese patients over the last 35 years. Clin Dev Immunol 2012; 2012: 562168.
- Handa S, Dabas G, De D, Mahajan R, Chatterjee D, Saika UN, et al. A retrospective study of dermatitis herpetiformis from an immunobullous disease clinic in north India. Int J Dermatol 2018; 57: 959–964.
- Ludvigsson JF, Otterblad-Olausson P, Pettersson BU, Ekbom A. The Swedish personal identity number: possibilities and pitfalls in healthcare and medical research. Eur J Epidemiol 2009; 24: 659–667.
- The Swedish Board of Health and Welfare. Quality of data and reporting procedures – National Patient register 2018. Available from: www.socialstyrelsen.se, 2018 (in Swedish).
- Ludvigsson JF, Andersson E, Ekbom A, Feychting M, Kim JL, Reuterwall C, et al. External review and validation of the Swedish national inpatient register. BMC Public Health 2011; 11: 450.
- Virta LJ, Kaukinen K, Collin P. Incidence and prevalence of diagnosed coeliac disease in Finland: results of effective case finding in adults. Scand J Gastroenterol 2009; 44: 933–938.
- Fry L. The falling incidence and prevalence of dermatitis herpetiformis. Br J Dermatol 2011; 165: 229.
- Salmi TT, Hervonen K, Kurppa K, Collin P, Kaukinen K, Reunala T. Celiac disease evolving into dermatitis herpetiformis in patients adhering to normal or gluten-free diet. Scand J Gastroenterol 2015; 50: 387–392.
- Catassi C, Verdu EF, Bai JC, Lionetti E. Coeliac disease. Lancet 2022; 399: 2413–2426.
- Gardner K, Crawford R. A decreasing incidence of dermatitis herpetiformis in a gluten-free era. J Am Acad Dermatol 2017; 76: AB12.
- Alonso-Llamazares J, Gibson LE, Rogers RS, 3rd. Clinical, pathologic, and immunopathologic features of dermatitis herpetiformis: review of the Mayo Clinic experience. Int J Dermatol 2007; 46: 910–919.
- Zhang F, Yang B, Lin Y, Chen S, Zhou G, Wang G, et al. Dermatitis herpetiformis in China: a report of 22 cases. J Eur Acad Dermatol Venereol 2012; 26: 903–907.
- Kaplan RP, Callen JP. Overlapping cutaneous disorders related to dermatitis herpetiformis. Clin Dermatol 1991; 9: 361–368.
- Hervonen K, Salmi TT, Kurppa K, Kaukinen K, Collin P, Reunala T. Dermatitis herpetiformis in children: a long-term follow-up study. Br J Dermatol 2014; 171: 1242–1243.
- Antiga E, Verdelli A, Calabro A, Fabbri P, Caproni M. Clinical and immunopathological features of 159 patients with dermatitis herpetiformis: an Italian experience. G Ital Dermatol Venereol 2013; 148: 163–169.
- Antiga E, Bonciolini V, Cazzaniga S, Alaibac M, Calabro AS, Cardinali C, et al. Female patients with dermatitis herpetiformis show a reduced diagnostic delay and have higher sensitivity rates at autoantibody testing for celiac disease. Biomed Res Int 2019; 2019: 6307035.
- Dahlbom I, Korponay-Szabo IR, Kovacs JB, Szalai Z, Maki M, Hansson T. Prediction of clinical and mucosal severity of coeliac disease and dermatitis herpetiformis by quantification of IgA/IgG serum antibodies to tissue transglutaminase. J Pediatr Gastroenterol Nutr 2010; 50: 140–146.
- Reunala T, Salmi TT, Hervonen K. Dermatitis herpetiformis: pathognomonic transglutaminase IgA deposits in the skin and excellent prognosis on a gluten-free diet. Acta Derm Venereol 2015; 95: 917–922.