SHORT COMMUNICATION
Palmar Basal Cell Carcinoma in Darker Skin Tone Patient: A Case Study
Nada ALGHAMDI1, Bader ALGAMDI1, Ahmed A. ALSAATI2* and Areej M. AL NEMER3
1Department of Dermatology, Imam Abdulrahman Bin Faisal University, Khobar, 2Department of Dermatology, College of Medicine, King Faisal University, Al-Hofuf and 3College of Medicine, Imam Abdulrahman Bin Faisal University, King Fahad Hospital of the University, Khobar, Saudi Arabia. *E-mail: Alsaati.ahmedaj@gmail.com
Citation: Acta Derm Venereol 2023; 103: adv13345. DOI: https://doi.org/10.2340/actadv.v103.13345.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: Oct 3, 2023; Published: Nov 20, 2023
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Basal cell carcinoma (BCC) is the most common form of skin cancer worldwide. Although BCC can develop in any skin type, it predominantly affects individuals with lighter skin tones, such as Fitzpatrick skin types I and II, and occurs less frequently in those with darker skin (1, 2). BCC usually presents as a slowly expanding nodule in sun-exposed areas, such as the head and neck (3); however, it is rarely encountered on acral surfaces, including the palm and plantar region (3–5). In numerous instances, certain factors that increase the likelihood of developing palmar BCC have been identified. These factors include exposure to arsenic, ionizing radiation, repetitive physical trauma, and genetic syndromes such as Gorlin syndrome, Bazex-Dupré-Christol syndrome, and xeroderma pigmentosum. However, the occurrence of this type of tumour on the palm of the hand as an isolated case, without any identifiable predisposing factors or associated syndromes, is uncommon (3, 6). We report here a case of a dark-skinned man of African descent who developed BCC on his palm without any known predisposing factors.
CASE REPORT
A 64-year-old male patient of Fitzpatrick skin type VI, with a medical history of type II diabetes mellitus, hypertension, and dyslipidaemia presented to the dermatology clinic at King Fahd Hospital of the University, Khobar City, Saudi Arabia, with concerns regarding a skin lesion on his right palm, which had been present for 5 years. The growth of the lesion had been slow, initially asymptomatic, but had seen a significant increase in size and developed accompanying pain in the recent year, limiting the patient’s hand mobility. The patient denied exposure to harmful chemical substances, such as arsenic, or any history of radiation therapy.
Clinical examination revealed a well-defined, greyish nodule at the centre of the right palm, with a focal area of black discoloration. The lesion measured approximately 2 cm in diameter and was firmly attached to the underlying structure (Fig. 1). Pain associated with the lesion interfered with normal finger flexion. Additional examination did not reveal any other significant findings. Based on these observations, we considered nodular melanoma, eccrine poroma, and pigmented BCC for the differential diagnosis. Surgical excision of the lesion was conducted, and the histopathological examination revealed islands of basaloid cells with peripheral palisading, continuous with the undersurface of the epidermis (Fig. 2). Notable features included clefts with mucin deposition between cell nests and adjacent stroma. Tumour cells contained melanin pigments within the cytoplasm, confirming the diagnosis of pigmented nodular BCC on the palm (Fig. 3). Immunohistochemistry results were positive for pancytokeratin, but negative for epithelial membrane antigen (EMA) and carcinoembryonic antigen (CEA). Moreover, analysis revealed the presence of tumour protein 63 (P63), B-cell lymphoma 2 (BCL-2), canalicular immunostaining of neprilysin (CD10), and Ber-EP4. A plastic hand reconstructive surgeon performed surgical excision under local anaesthesia. The lesion was thoroughly excised with a 4-mm margin down to the palmar fascia, and the site was reconstructed with a full-thickness skin graft. Histological evaluation confirmed the total excision of the lesion with a 2-mm free margin. The patient’s postoperative course was uneventful, with successful grafting. Subsequent examination revealed restored hand motion, including flexion.

Fig. 1. Clinical view of the lesion. A well-defined greyish nodule on the centre of the right palm with area of focal blackish discoloration. The lesion is approximately 2 cm in diameter, firmly attached to the underlying structure.
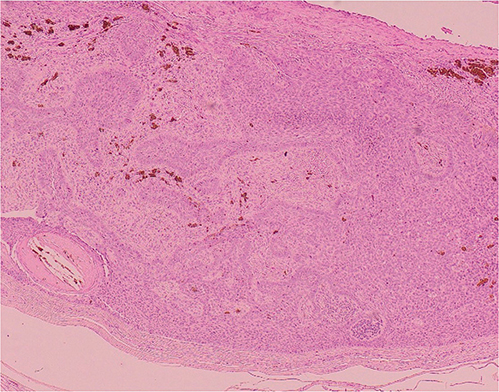
Fig. 2. Low-power microscopy of the lesion (original magnification 40×, haematoxylin and eosin (H&E)). The images depict proliferation of basaloid cells and peripheral palisading. Pigmentation is also evident.
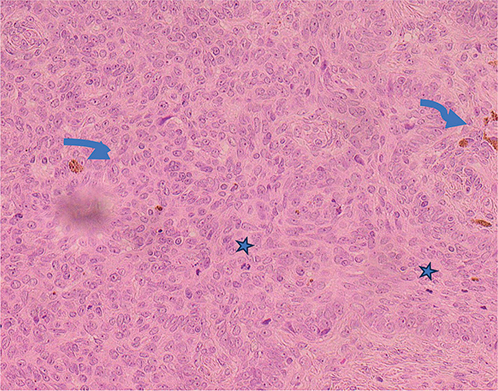
Fig. 3. High-power microscopic images of the lesion (original magnification 40×, haematoxylin and eosin (H&E)). Neoplastic cells are mitotically active, and focally pigmented.
DISCUSSION
BCC is the most prevalent cutaneous malignancy that occurs with UV ray exposure, especially Ultraviolet B, which happens to be a major risk factor in the development of the disease. BCC typically manifests in sun-exposed skin regions, such as the head and neck. However, superficial BCC can also appear on parts of the body that are not typically exposed to the sun, such as the trunk and lower back, as seen in fibroepithelioma of Pinkus. Other associated risk factors include; Fitzpatrick skin types I and II, Northern European ethnicity, intense sun exposure, and use of tanning salons (1, 2). Isolated BCC tumours on the palms and soles are exceedingly rare, barring the presence of other predisposing factors, such as BCC inherited syndrome, exposure to arsenic, or ionizing radiation or scar formation (2, 4, 6, 11).
The first thoroughly documented instance of BCC appearing on the palm was reported by D. E. Jonson in 1960 (8), followed by additional reports from Hunter in 1960 (9) and Hyman in 1965 (12). Since then, there have been a handful of rare cases reported, totalling 18 in English-language medical literature. Most of these cases were associated with various predisposing factors (2–7, 13). The most frequently reported clinical manifestations were scaly plaques, erosion or ulceration and, less commonly, tumours or nodules (4, 6, 7, 13). Lopez et al. suggested that, despite its rarity, BCC should be included in the differential diagnosis for solitary palmar lesions (4). From a histological perspective, Hyman et al. (12) characterized BCC as having a significant compact horny layer, a thick granular layer, and clusters of basal cell epithelioma occupying a large portion of the cutis, extending with palisading. However, other crucial differential diagnoses, such as squamous cell carcinoma, Bowen’s disease, and eccrine poroma, should always be taken into account. Eccrine poroma can be differentiated by its distinctive small tumour cells, the formation of keratohyalin granules, and focal proliferation of intraepidermal sweat ducts. Lopez-Sanchez et al. (4) pointed out that positive staining with BerEP4 antibodies, which target epithelial cell adhesion molecules, can aid in distinguishing BCC from squamous cell carcinoma (SCC). However, the potential for concurrent BCC and SCC should not be dismissed, as illustrated in the unusual case reported by Lam et al. (5), where the initial biopsy and frozen histology revealed features consistent with both SCC in situ and BCC. BCC should be treated with caution due to its potential to grow, ulcerate, and deeply invade the bone, possibly leading to osteomyelitis and amputation, or even lymph node metastasis (10).
In conclusion, although isolated BCC are uncommon in darker-skin individuals, it is very rare for it to develop on site such as the palm, especially in the absence of precipitating factors. Thus, the current case is highly unusual, as a union of multiple rare factors was present in a single case. However, palmar BCC in dark-skin patients should be considered within the differential diagnosis of any clinically suspected lesions, even in the absence of pre-disposing factors, in order to avoid delayed BCC diagnosis that can lead to unfavourable complications.
REFERENCES
- McDaniel B, Badri T, Steele RB. Basal cell carcinoma. StatPearls. Treasure Island (FL): StatPearls Publishing; 2022. https://www.ncbi.nlm.nih.gov/books/NBK482439/
- Ramadan S, Sharma N, Hassan Z. Palmar psoriasis or missed BCC? – A case report. JPRAS Open 2021; 28: 29–32.
- Lateo S, Charlton FG, Ormond P. A palmar injury that failed to heal. Clin Exp Dermatol 2006; 31: 731–732.
- López-Sánchez C, Ferguson P, Collgros H. Basal cell carcinoma of the palm: an unusual presentation of a common tumour. Australas J Dermatol 2019; 61: 69–70.
- Lam C, Fuller C, Flamm A, Billingsley EM. Collision tumor of basal and squamous cell carcinoma of the palm. J Clin Aesthet Dermatol 2019; 12: 28–30.
- Starzycki Z, Stachura J. Rodent ulcer of the palm. Dermatology 1984; 168: 195–198.
- Alonso-Corral MJ, Gómez-Avivar MP, Berenguel-Ibañez MM, Ruiz-Villaverde R. Palmar basal cell carcinoma: an unusual site? Actas Dermosifiliogr 2014; 105: 623–624.
- Johnson DE. Basal-cell epithelioma of the palm. Arch Dermatol 1960; 82: 253.
- Hunter GA, Hell FF. Tumours of the palm and sole resembling basal cell epithelioma. Br J Dermatol 1960; 72: 283–287.
- Russell E, Udkoff J, Knackstedt T. Basal cell carcinoma with bone invasion: a systematic and pooled survival analysis. J Am Acad Dermatol 2022; 86: 621–627.
- Torrelo A, Vicente A, Navarro L, et al. Early-onset acral basal cell carcinomas in Gorlin syndrome. Br J Dermatol 2014; 171: 1227–1229.
- Hyman AB. Basal cell epithelioma of the palm. Arch Dermatol 1965; 92: 571.
- Machida M, Ansai S, Hida Y, Kubo Y, Arase S, Kuramoto K. Basal cell carcinoma arising on the palm. J Dermatol 2010; 38: 94–96.