SHORT COMMUNICATION
A Case of Bowen’s Disease in the Periungual Region: Raising the Possibility of Genitodigital Transmission of Human Papillomavirus Between Sexual Partners
Ho Sung KIM, Ji An UH, Myoung Shin KIM, Un Ha LEE and Soo-Kyung LEE*
Department of Dermatology, Inje University Sanggye Paik Hospital, Inje University College of Medicine, Seoul, South Korea. E-mail: prisca0624@naver.com
Citation: Acta Derm Venereol 2023; 103: adv13439. DOI https://doi.org/10.2340/actadv.v103.13439.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: Aug 1, 2023; Published: Sep 20, 2023
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Bowen’s disease (BD) is a malignant condition that can affect the periungual region. It often presents as a rough, wart-like growth on the skin surrounding the nail or nail bed, which can be misdiagnosed as a viral wart, leading to inappropriate treatment (1). A chronic high-risk human papillomavirus (HPV) infection is a major risk factor for skin carcinogenesis, and is associated with the development of BD in periungual regions (1). Previous reports indicate that HPV type 16 is the most frequent infection, followed by other high-risk HPV subtypes, including HPV type 73 (2). High-risk HPVs are known to be common causes of genital neoplasms, including cervical cancer. Some studies have suggested that this virus can be transmitted through digital contact, potentially leading to the development of digital warts or neoplasms (2). We report here a case of Bowen’s disease in the periungual region associated with HPV type 73, suggesting the potential for genitodigital transmission between sexual partners.
CASE REPORT
A 26-year-old man presented with a hyperkeratotic papule, 7 mm in size, in the periungual region of his left second finger, which had persisted for 6 months (Fig. 1a). He reported that the size had increased significantly 1 month prior to presentation. He had no significant medical history except for a depressive disorder. His intimate partner had been treated for cervical cancer related to HPV type 73 and they expressed concerns about sexual transmission. The patient showed no signs of genital warts or HPV-related lesions in the genital area. Dermoscopic examination revealed pinpoint bleeding and violaceous to black macules (Fig. 1b). Punch biopsy revealed full-thickness epidermal dysplasia with increased mitotic activity, confirming BD (Fig. 2a, b). Immunohistochemistry staining revealed that P16 was positively expressed in the epidermis and the Ki-67 labelling index was as high as 70% (Fig. 2c, d). HPV genotyping analysis revealed that the patient tested positive for HPV type 73, which was identical to the HPV subtype detected in the intimate partner’s cervical cancer. He underwent urine testing in the urology department for other sexually transmitted infections (STIs), and all results were negative. Preoperative blood tests, including common blood counts and serology for STIs, revealed no pathological findings, suggesting the absence of an immunosuppressed state. To treat the tumour, a wide local excision was performed in consultation with the plastic surgery department. The resected tissue exhibited no evidence of remaining neoplastic cells. The patient was followed up for 2 months for wound assessment and showed no signs of recurrence. Written informed consent for publication was obtained from the patient.
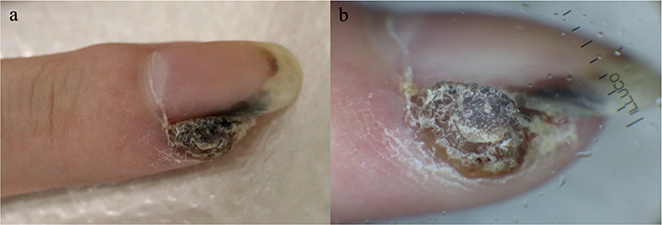
Fig. 1. Clinical and dermoscopic findings. (a) Hyperkeratotic papule, 7 mm in size, in the periungual region of the left second finger. (b) Dermoscopic image of the lesion showing scaly, papillomatous papule, with pinpoint bleeding and violaceous black macules.
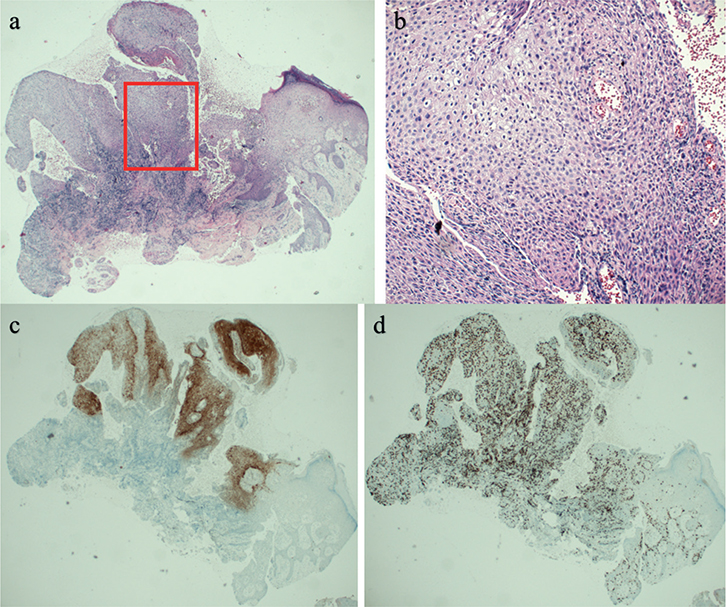
Fig. 2. Histological findings. (a) Low-power view of the punch biopsy tissue showing the tumour lesion (haematoxylin and eosin staining: HE, × 40). (b) High-power view of the red square area in (a), showing full-thickness epidermal dysplasia with increased mitotic activity (HE, × 200). (c, d) Immunohistochemical analysis of p16 (c, p16 × 40) and Ki-67 (d, Ki-67 × 40). P16 was positively expressed and the Ki-67 labelling index was as high as 70%.
DISCUSSION
BD of the fingertip is a rare condition that presents with various clinical manifestations, such as verrucous lesions, fissuring, ulceration, paronychia, or nail dystrophy. While HPV-associated BD primarily affects the anogenital region, approximately 30% of cases involve extragenital locations. These are particularly associated with HPV 16 (3). The hand, including the finger and nail unit, is particularly vulnerable to trauma and represents the most commonly affected site for extragenital BD linked to HPV. The involvement of the E6 protein of HPV in the degradation of the tumour suppressor protein p53, leading to the development of cervical cancer, is a well-established fact (4–6). In addition, dysregulation of the Rb/p16INK4a pathway is believed to play a significant role in HPV-induced BD, although the precise underlying mechanisms remain to be fully elucidated (7).
A meta-analysis conducted in 2014 depicted that nearly half of periungual squamous cell carcinoma (SCC) cases were related to high-risk HPVs, indicating a strong link between the virus and the development of cutaneous SCCs (4). It is notable that many patients with periungual SCC also have a history of other HPV-associated lesions, primarily genital carcinomas, suggesting the possible genitodigital transmission of the virus (4). In this case, as the patient’s intimate partner was treated for cervical cancer associated with HPV type 73, the detection of the exact same HPV genotype in the patient strongly suggests genitodigital transmission between sexual partners. This mode of transmission highlights the importance of HPV vaccination, not only for patients, but also for their sexual partners, to prevent HPV-related diseases, including cutaneous SCCs. Although the preventive efficacy of HPV vaccines before sexual debut is well established, there is ongoing debate regarding their therapeutic effects (8). It should be noted that the current HPV vaccines do not include HPV type 73, which has been detected in the patient, thus posing a limitation. Overall, the potential for genitodigital transmission of HPV and the associated development of periungual SCCs further emphasize the importance of proper diagnosis and treatment of BD. Early detection and treatment can prevent the further spread of the virus and the development of more severe diseases.
The current patient’s biopsy specimen demonstrated positivity for p16 and high Ki-67 expression, consistent with previous studies that found that HPV-positive lesions exhibited higher immunopositivity than HPV-negative lesions (9, 10). The P16 protein, also known as p16 INK4a, is commonly overexpressed in oncogenic HPV infections, including anogenital neoplasms (9, 10). In contrast, non-HPV-related SCCs and other tumours have shown mixed results, with some studies reporting protein loss and others reporting overexpression. Kreuter et al. reported 6 cases of periungual HPV-positive SCC (9). The authors demonstrated that HPV-positive tumours showed higher Ki-67 expression (ranging from 70% to 95%), compared with HPV-negative tumours, which showed Ki-67 expression ranging from 5% to 50%. Moreover, they suggested that Ki-67 staining can be used to measure the level of proliferative activity, which is an essential factor indicating aggressive behaviour and a high recurrence rate of periungual HPV-positive SCCs (9).
This case report highlights the possibility of genitodigital transmission of HPV type 73, leading to periungual Bowen disease. Increased awareness of this transmission mode and the role of HPV in cutaneous SCCs can improve diagnosis, treatment, and prevention strategies. Further research is necessary to establish guidelines for prevention and management of affected patients and their partners.
REFERENCES
- Lecerf P, Richert B, Theunis A, Andre J. A retrospective study of squamous cell carcinoma of the nail unit diagnosed in a Belgian general hospital over a 15-year period. J Am Acad Dermatol 2013; 69: 253–261.
- Marti-Marti I, Bosch-Amate X, Morgado-Carrasco D, Albero-Gonzalez R, Santos-Briz A, Puebla-Tornero L, et al. High-risk mucosal human papillomavirus-associated squamous cell carcinoma of the fingers presents distinctive clinicopathological characteristics and outcomes: a bicentric retrospective study. Clin Exp Dermatol 2023; 48: 211–217.
- Ansari SMM, Gupta A, Nayak CS. Bowen’s disease on two different unrelated anatomical sites (genitals and nail) in succession in an immunocompromised patient. Indian J Sex Transm Dis AIDS 2022; 43: 189–191.
- Wang J, Aldabagh B, Yu J, Arron ST. Role of human papillomavirus in cutaneous squamous cell carcinoma: a meta-analysis. J Am Acad Dermatol 2014; 70: 621–629.
- Shimizu A, Kuriyama Y, Hasegawa M, Tamura A, Ishikawa O. Nail squamous cell carcinoma: a hidden high-risk human papillomavirus reservoir for sexually transmitted infections. J Am Acad Dermatol 2019; 81: 1358–1370.
- Piipponen M, Riihilä P, Nissinen L, Kähäri V-M. The role of p53 in progression of cutaneous squamous cell carcinoma. Cancers 2021; 13: 4507.
- Murao K, Yamasaki K, Agawa H, Nakajima M, Iwasaka M, Kubo Y. Bowen disease on the dorsum of the foot associated with human papillomavirus type 16. J Med Invest 2022; 69: 152–154.
- Mo Y, Ma J, Zhang H, Shen J, Chen J, Hong J, et al. Prophylactic and Therapeutic HPV Vaccines: Current Scenario and Perspectives. Front Cell Infect Microbiol 2022; 12: 909223.
- Kreuter A, Gambichler T, Pfister H, Wieland U. Diversity of human papillomavirus types in periungual squamous cell carcinoma. Br J Dermatol 2009; 161: 1262–1269.
- Walts AE, Lechago J, Bose S. P16 and Ki67 Immunostaining is a useful adjunct in the assessment of biopsies for HPV-associated anal intraepithelial neoplasia. Am J Surg Patholog 2006; 30: 795–801.