The optimal surgical margin width for basal cell carcinoma (BCC) is currently unclear, and the guidelines are inconsistent (1–3). In 2007, recommendations on excision margins were introduced in the Dutch BCC guideline. Surgical margins of 3 mm in small (≤ 10 mm) primary BCC and 5 mm in large (> 10 mm), high-risk (aggressive histological subtype) or recurrent BCC were advised (4). In 2015 the guideline was updated, with the margin for low-risk BCC being adjusted to 3–4 mm, the size-threshold for high-risk BCC increased to 20 mm, and H-zone location was incorporated as a high-risk BCC (2).
The aim of this study is to assess the risk of incomplete excision in case of adherence and non-adherence to the recommended surgical margins according to the 2007 and 2015 Dutch BCC guidelines.
MATERIALS, METHODS and RESULTS
The Pathologic-Anatomic National Automated Archive (PALGA) database was searched for cases of BCC. Inclusion criteria were: BCCs treated with conventional excision at the dermatology department of Maastricht University Medical Centre (MUMC+), Maastricht, the Netherlands, in 2010; with histopathological evaluation of the excision specimen by a pathologist from MUMC+. The institution’s medical ethics committee approved the study. Retrospectively, for each BCC tumour, characteristics were recorded to enable categorization into low-risk vs high-risk BCC. The actual excision margin used and the optimal margin according to the guidelines were recorded, as well as the histopathological completeness of the excision. Non-adherence was defined as the use of an excision margin smaller than recommended by the guidelines. This study evaluates actual non-adherence to the 2007 guideline (as this guideline was valid at the time of the excisions in 2010 included in this study) and theoretical non-adherence to the 2015 guideline. To evaluate whether risk of incomplete excision increases in case of non-adherence, relative risks (RR) of incomplete excision with 95% confidence interval (CI) were calculated. For statistical analysis, the Statistical Package for Social Sciences (SPSS, version 23) and Openepi.com were used. p-values < 0.05 were considered to indicate statistical significance.
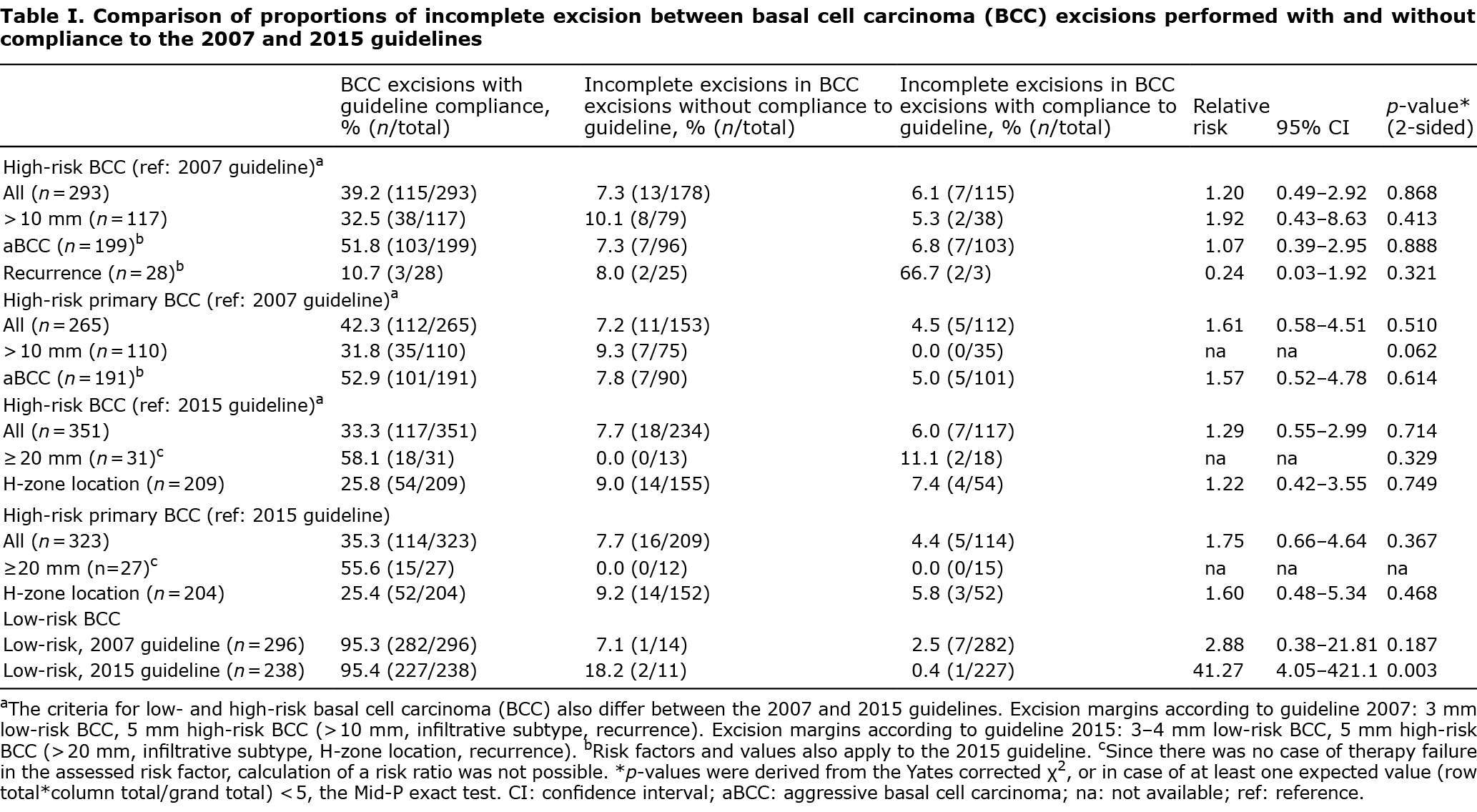
A search of the PALGA database for BCC diagnosis in 2010 resulted in 589 BCC in 469 patients eligible for the study. Patients had a mean age of 69.1 (± 12.4) years and 54.4% were male. In total, 83.2% (n = 390) of patients had 1 BCC, 11.1% (n = 52) had 2 BCCs, 4.1% n = 19) had 3 BCCs, and 1.7% (n = 8) had 4–8 BCCs excised. All included tumours were excised with a 2-, 3- or 5-mm margin (n = 19, 442 and 128, respectively). Mean tumour size was 8.2 (± 5.2) mm and 52.8% (n = 311) was located in the head- and neck area, 30.2% (n = 178) on the torso and 17% (n = 100) on the extremities. In low-risk BCC, the risk of incomplete excision was 2.5% and 0.4% after adherence to the 2007 guideline and 2015 guideline, respectively (Table I). For low-risk BCC, non-adherence to the 2015 guideline was associated with a significantly increased risk of incomplete excision (RR 41.27; 95% CI: 4.05–421.3, p = 0.003) and a trend towards increased risk in case of non-adherence to the 2007 guideline (RR 2.88; 95% CI: 0.38–21.81, p = 0.187).
DISCUSSION
In this study, the highest relative risk of incomplete excision was observed for low-risk BCCs excised with a smaller margin than recommended by the guidelines. Overall adherence in low-risk BCC was high. In high-risk BCC, relative risks associated with non-adherence were lower and non-significant, whilst adherence to recommended margins was rather poor.
These results imply that physicians may have a well-developed sense for which high-risk BCCs the use of a margin smaller than recommended in the guideline might be acceptable. Non-adherence rates were especially high for tumours larger than 10 mm and for recurrent tumours. Due to the retrospective nature of this study, it was not possible to track down the reasons for guideline deviations for high-risk BCC. It is likely that a 5-mm margin for these tumours was considered too large by the treating physician. In fact, high-quality evidence for the 10-mm size threshold in the 2007 guideline was lacking and may have been rather arbitrary, because, in the 2015 guideline it was adjusted to 20 mm without new studies to substantiate this modification. Also, most recurrent BCCs occurred after non-invasive treatment of superficial BCCs and recurrence was not accompanied by other high-risk features in the majority of cases. For non-melanoma skin cancer, guideline deviation associated with patient’s age, tumour localization and surgeon’s experience has been reported (5). According to a systematic review, non-adherence to clinical (non-dermatological) guidelines is often intentional and due to valid reasons, such as comorbidity and contra-indications, which does not necessarily lead to impaired quality of care (6). This is probably also the case in the current study. The poor adherence in high-risk BCCs is in line with the results of another study in the Netherlands, in which self-reported BCC guideline adherence with respect to excision margins was 37.9% (7).
For low-risk BCC, non-adherence occurred in only 5% of cases, and for a more straightforward reason: these excisions served a diagnostic rather than a therapeutic purpose because of a differential diagnosis including an atypical melanocytic lesion. In these diagnostic cases, the use of a 2-mm margin is prescribed by the Dutch melanoma guideline (8).
Currently, both the Dutch and the recent European consensus-based guideline on BCC advise margins of 3–4 mm in low-risk BCC and a minimal margin of 5 mm (Dutch guideline) or 5–15 mm (European guideline) in high-risk BCC (2, 3). In our study population, a margin of 3 mm was sufficient in 99.6% of BCCs categorized as low risk by current guidelines (2, 3). Also, a margin of 5 mm for high-risk BCC (2) was effective and led to complete tumour removal in 94% of cases. The study population did not include high-risk facial BCCs, for which micrographic surgery with 3D margin evaluation, rather than larger margins, is preferred (9).
Finding the optimal surgical margin is always a balance between complete tumour removal, for which higher margins are more effective, and unnecessary removal of healthy tissue, for which smaller margins are preferable. The findings of this study indicate that, for high-risk BCC, attempts to prevent incomplete excision have resulted in recommendations by the various guidelines that do not match the desire of treating dermatologists to take into account other factors that drive their decisions regarding the optimal excision margin. Adherence to the guideline in high-risk BCC was poor, but lack of adherence had limited effect on the risk of incomplete excision. Current guidelines seem to be very cautious and defensive, and do not represent clinical practice. Therefore, revision of the guideline recommendations on the excision margin for high-risk BCC may be warranted. However, a problem in providing evidence-based recommendations is the lack of high-quality research on this subject.
A limitation of this study is the relatively low sample size. As a result, the power to detect small, but relevant, increases in risk of incomplete excision due to non-adherence is limited. Furthermore, the study has been performed in a single centre, which may limit the generalizability of the results.
In conclusion, the results of this study suggest that non-adherence to guidelines is associated with an increased risk of incomplete excision for low-risk BCC. For high-risk BCC, guideline adherence was poor, but the observed increase in risk of incomplete excision was less substantial, so clinicians seem to be able to judge in which cases deviations from guideline recommendations can be deemed acceptable. With high-quality evidence still lacking, we need to be wary of advising unnecessary large margins for situations in which micrographic surgery might be the better option.
The authors have no conflicts of interest to declare.
REFERENCES
- Nahhas AF, Scarbrough CA, Trotter S. A review of the global guidelines on surgical margins for nonmelanoma skin cancers. J Clin Aesthet Dermatol 2017; 10: 37–46.
- Dutch Society of Dermatology and Venereology. Basal cell carcinoma, national guideline version 2.1. Utrecht: Dutch Society of Dermatology and Venereology; 2015. Published online at www.oncoline.nl.
- Peris K, Fargnoli MC, Garbe C, Kaufmann R, Bastholt L, Seguin NB, et al. Diagnosis and treatment of basal cell carcinoma: European consensus-based interdisciplinary guidelines. Eur J Cancer 2019; 118: 10–34.
- Dutch Society of Dermatology and Venereology. Evidence-based guideline on the treatment of basal cell carcinoma. Utrecht: Dutch Society of Dermatology and Venereology; 2007. Published online at www.oncoline.nl.
- Marchetti Cautela J, Mannocci A, Reggiani C, Persechino F, Ferrari F, Rossi E, et al. Identifying the factors that influence surgeon’s compliance with excisional margins of non-melanoma skin cancer. PLoS One 2018; 13: e0204330.
- Arts DL, Voncken AG, Medlock S, Abu-Hanna A, van Weert HC. Reasons for intentional guideline non-adherence: a systematic review. Int J Med Inform 2016; 89: 55–62.
- Borgonjen RJ, van Everdingen JJ, Bruijnzeel-Koomen CA, van de Kerkhof PC, Spuls PI. A national study on adherence to a basal cell carcinoma guideline; development of a tool to assess guideline adherence. Br J Dermatol 2015; 172: 1008–1013.
- Dutch Melanoma Working Group. Melanoma, national guideline, version 3.0. 2019.
- van Delft LCJ, van Loo E, Mosterd K, Kelleners-Smeets NWJ. Comment on “Diagnosis and treatment of basal cell carcinoma: European consensus-based interdisciplinary guidelines”. Eur J Cancer 2020; 131: 98–99.