Tuberculosis (TB) is caused by Mycobacterium tuberculosis, an acid-fast bacillus, which is usually transmitted through the respiratory tract (1). The lungs are the most commonly infected site, but the skin, among many other organs, may also be affected (1). Cutaneous TB (CTB) is a rare form of TB, comprising only 1–1.5% of cases of extrapulmonary TB (2). CTB is often classified by the route of propagation: haematogenous dissemination, TB from exogenous source, or TB from endogenous source (2, 3). Clinical manifestations of CTB include lupus vulgaris, tuberculosis verrucosa cutis, scrofuloderma, miliary tuberculosis, orificial tuberculosis, tuberculous chancre, gumma and metastatic tuberculosis (2, 3). In addition to “true” CTB, tuberculids (i.e. erythema induratum of Bazin, papulonecrotic tuberculid and lichen scrofulosorum) are skin manifestations of underlying TB infection where M. tuberculosis may not be found from the lesion itself, but is considered the cause of the skin symptom and is treated successfully with TB treatment (2–4).
CASE REPORT
A 61-year-old Caucasian female was referred to the Department of Dermatology for an ulcer in her face, which had been present for 1.5 months. She was using bisoprolol for dysrhythmia and had been diagnosed with rheumatoid arthritis 5 years earlier. Since then, she had been taking hydroxychloroquine and sulfasalazine for rheumatoid arthritis, and adalimumab had been added to the antirheumatic therapy 5 months previously. Screening for hepatitis B and HIV, interferon gamma release assay (IGRA) for M. tuberculosis, and chest X-ray were performed, with normal results, before initiating adalimumab.
In the late summer, the patient was bitten by a mosquito near an eyebrow and noticed a blister afterwards. The lesion became crusted, expanded and ulcerated. Impetigo was suspected and medicated with fusidic acid ointment and cefalexin, with no improvement. Adalimumab was suspended because of the suspected infection. When the patient developed adenopathy of the neck and reported having fever for several weeks, a general practitioner suspected ulceroglandular tularaemia (Fig. 1A). However, the ulcer expanded during 2 weeks of treatment with doxycycline and the patient was referred to a dermatologist.
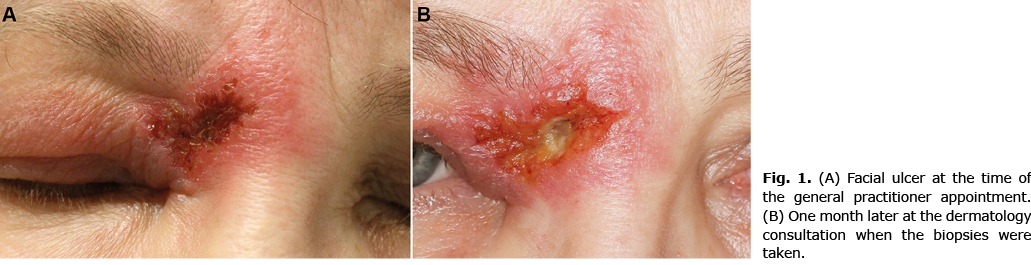
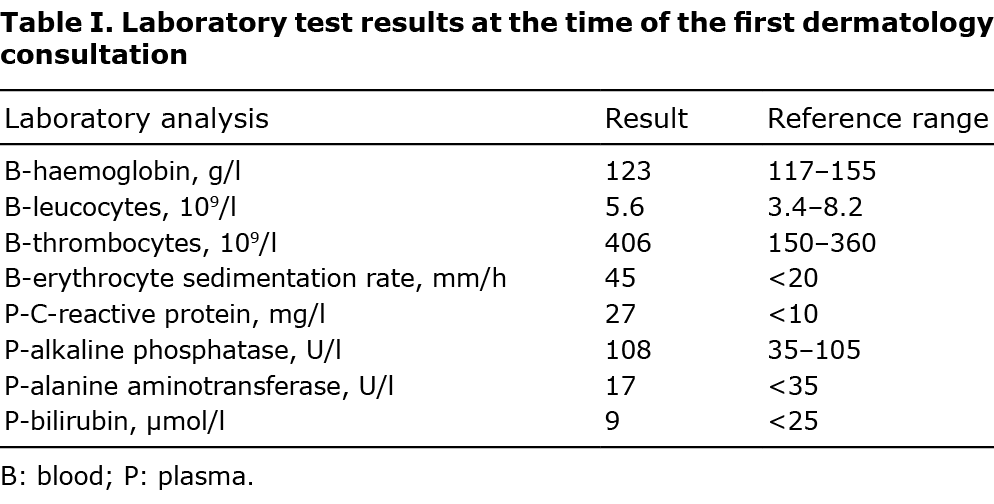
In the consultation, an ulcer surrounded by oedema located medially to the eyebrow was identified. Except for adenopathy of the neck on the same side, physical examination was unremarkable. The laboratory findings are listed in Table I. Tularaemia was still considered the most probable diagnosis, since the area of Oulu University Hospital is endemic for tularaemia, and late summer or early autumn is the typical season for tularaemia in Finland. Moreover, the results for Franciella tularensis antibodies were not yet available. However, when, after 2 weeks of treatment with ciprofloxacin, the ulcer was still expanding (Fig. 1B), biopsies for histological examination and mycobacterial and fungal culture were taken from the ulcerative lesion.
The biopsy revealed granulomatous inflammation and necrosis. Ziehl-Neelsen stain showed acid-fast bacilli suggestive of mycobacterial infection. Fungal and routine bacterial culture was negative; no PCR test for M. tuberculosis was taken. The patient was referred to the Department of Infectious Diseases for further investigation.
Full-body computed tomography (CT) scan revealed enlarged lymph nodes in the abdomen and neck, and suspected tuberculosis lesions in the lungs and spleen. PCR test for M. tuberculosis was positive from the cervical lymph node and sputum and, later, the culture from the facial ulcer also showed M. tuberculosis. IGRA (using QuantiFERON-TB Gold-in-tube assay, DiaSorin, Saluggia Italy) was now > 4 IU/ml (reference range <0.35 IU/ml). Due to COVID-19 restrictions, the patient had recently had very limited contact with others, and no contacts with active TB were detected. Instead, the patient found out that she had been in contact with a person with active TB in very early childhood, and therefore her condition was considered a reactivation of latent tuberculosis infection (LTBI). Treatment with pyrazinamide 1,500 mg/day, rifampicin 600 mg/day, isoniazid 300 mg/day and ethambutol 1,200 mg/day was initiated for 9 months, and the patient was discharged in good condition.
DISCUSSION
It has been estimated that, globally, 1 one in every 3 people is latently infected with M. tuberculosis (5). However, only a minority of TB infections manifest as active disease. In an individual with LTBI, the lifetime risk of active TB infection is 5–15%, but some subpopulations, such as immunocompromised individuals and those with HIV, are at increased risk (6). Treatment with tumour necrosis factor (TNF)-α inhibitors also poses such a risk because of the important role of TNF in the defence against M. tuberculosis (7, 8). Systematic screening for LTBI is therefore recommended before initiating anti-TNFα therapy (6). The available methods to test LBTI are tuberculin skin test (TST) and IGRA, both of which can be used according to the WHO’s recommendations (6). Many guidelines regarding immunosuppressed patients also recommend chest X-ray and detailed clinical history of risk factors (travelling or migration from endemic areas, exposure to individuals with active TB) in addition to TST or IGRA, some recommend concurrent TST and IGRA testing, and some guidelines suggest recurrent testing during long-term medical immunosuppression (9).
Our patient was screened for LTBI by IGRA and chest X-ray before initiating adalimumab. However, she had been taking 10 mg prednisolone daily for a week before the IGRA sample was taken, and during the preceding weeks she had also had several intra-articular corticosteroid injections, which may have systemic effects (10). Immunosuppression may affect the reliability of LTBI screening (11). The estimations of IGRA sensitivity for LTBI vary and are somewhat conflicting. A sensitivity of approximately 80–90%, depending on the method used, has been suggested in countries with low incidence of TB (12). In another meta-analysis, sensitivity of 52% was estimated in immune-competent adults, and in immunocompromised individuals the sensitivity was even lower (13). In meta-analyses, specificity of IGRA and TST for LBTI is 93–100% and 88–100%, respectively, but BCG vaccination significantly reduces the specificity of TST (12–14).
Screening for LTBI is important before initiating biological agents, especially TNF-α inhibitors. However, the limitations of LTBI screening must be observed and it is necessary to remain vigilant for symptoms and signs of TB, even though the initial screening shows normal results. Recurrent LTBI testing should be considered, particularly if the patient develops unexpected new clinical signs.
REFERENCES
- Flynn JL, Chan J. Immunology of tuberculosis. Ann Rev Immunol 2001; 19: 93–129.
- van Zyl L, du Plessis J, Viljoen J. Cutaneous tuberculosis overview and current treatment regimens. Tuberculosis 2015; 95: 629–638.
- Bravo FG, Gotuzzo E. Cutaneous tuberculosis. Clin Dermatol 2007; 25: 173–180.
- Barbagallo J, Tager P, Ingleton R, Hirsch RJ, Weinberg JM. Cutaneous tuberculosis: diagnosis and treatment. Am J Clin Dermatol 2002; 3: 319–328.
- Getahun H, Matteelli A, Chaisson RE, Raviglione M. Latent Mycobacterium tuberculosis infection. N Engl J Med 2015; 372: 2127–2135.
- World Health Organization. Latent tuberculosis infection: updated and consolidated guidelines for programmatic management. 2018. Available from: https://apps.who.int/iris/bitstream/handle/10665/260233/9789241550239-eng.pdf.
- Gómez-Reino JJ, Carmona L, Rodríguez Valverde V, Mola EM, Montero MD. Treatment of rheumatoid arthritis with tumor necrosis factor inhibitors may predispose to significant increase in tuberculosis risk: a multicenter active-surveillance report. Arthritis Rheum 2003; 48: 2122–2127.
- Askling J, Fored CM, Brandt L, Baecklund E, Bertilsson L, Cöster L, et al. Risk and case characteristics of tuberculosis in rheumatoid arthritis associated with tumor necrosis factor antagonists in Sweden. Arthritis Rheum 2005; 52: 1986–1992.
- Hasan T, Au E, Chen S, Tong A, Wong G. Screening and prevention for latent tuberculosis in immunosuppressed patients at risk for tuberculosis: a systematic review of clinical practice guidelines. BMJ Open 2018; 8: e022445.
- Habib GS. Systemic effects of intra-articular corticosteroids. Clin Rheumatol 2009; 28: 749–756.
- Wong SH, Gao Q, Tsoi KKF, Wu WKK, Tam LS, Lee N, et al. Effect of immunosuppressive therapy on interferon γ release assay for latent tuberculosis screening in patients with autoimmune diseases: a systematic review and meta-analysis. Thorax 2016; 71: 64–72.
- Pai M, Denkinger CM, Kik S v., Rangaka MX, Zwerling A, Oxlade O, et al. Gamma interferon release assays for detection of Mycobacterium tuberculosis infection. Clin Microbiol Rev 2014; 27: 3–20.
- Doan TN, Eisen DP, Rose MT, Slack A, Stearnes G, McBryde ES. Interferon-gamma release assay for the diagnosis of latent tuberculosis infection: a latent-class analysis. PLoS ONE 2017; 12: e0188631.
- Diel R, Goletti D, Ferrara G, Bothamley G, Cirillo D, Kampmann B, et al. Interferon-γ release assays for the diagnosis of latent Mycobacterium tuberculosis infection: a systematic review and meta-analysis. Eur Respir J 2011; 37: 88–99.