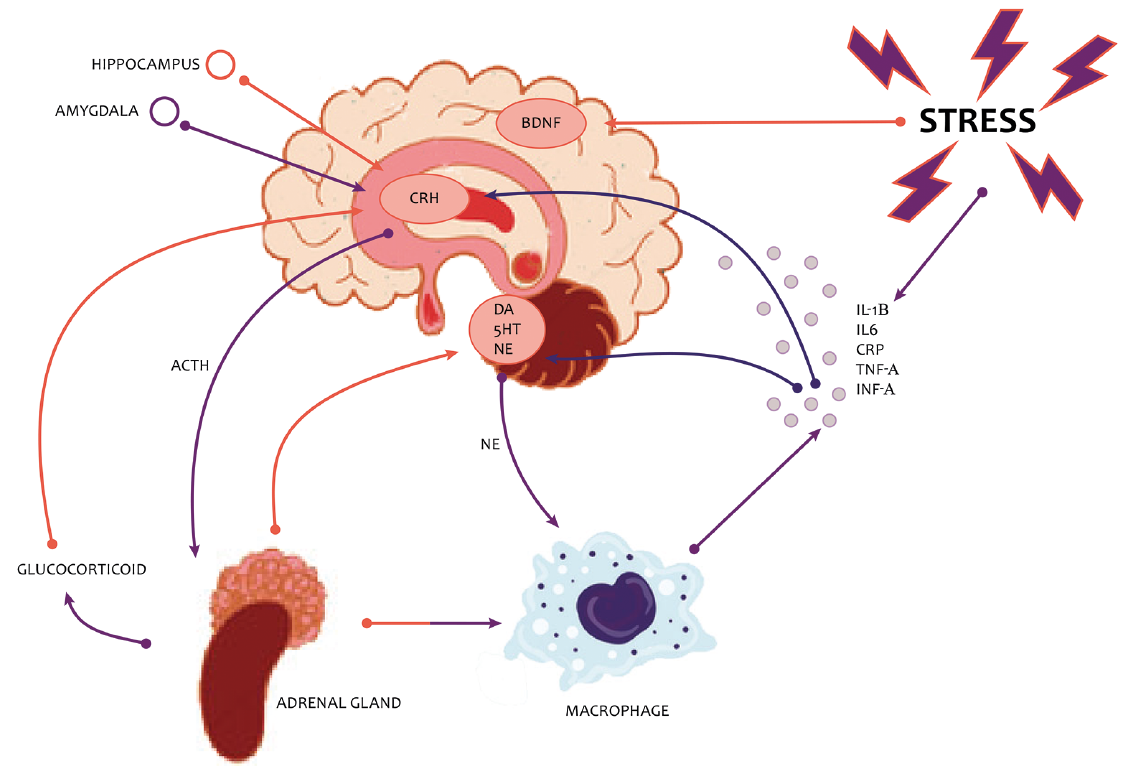
Fig. 1. Hypothalamic-pituitary-adrenal (HPA) axis and depression. BDNF: brain-derived neurotrophic factor; CRH: corticotropin-releasing hormone; DA: dopamine; 5HT: serotonin; NE: noradrenaline.
1Dermatology Centre, Salford Royal NHS Foundation Trust, 2Division of Neuroscience and Experimental Psychology, School of Biological Sciences, Faculty of Biology, Medicine and Health, University of Manchester, Manchester Academic Health Science Centre, Manchester, UK, 3National Heart, Lung, and Blood Institute, National Institutes of Health, Bethesda, USA, 4Clinical Epidemiology Unit, IDI-IRCCS, Rome, Italy, 5School of Healthcare Sciences, College of Biomedical & Life Sciences, Cardiff University, Cardiff, 6School of Health Sciences, NIHR Manchester Biomedical Research Centre, University of Manchester, Manchester, UK, 7Harvard Medical School and Beth Israel Deaconess Medical Center, Boston, 8International Psoriasis Council, St. Louis, USA, 9Dermatology Centre, University of Manchester, NIHR Manchester Biomedical Research Centre, Manchester, UK, 10Dermatology Department, University of Chile and Probity Medical Research, Santiago, Chile, and 11Department of Dermatology, Hospital de la Santa Creu i Sant Pau, Universitat Autònoma de Barcelona, Barcelona, Spain
Psoriasis is a systemic, relapsing, inflammatory disease associated with serious comorbidities including mood problems and/or unhealthy lifestyle behaviours. Cutaneous and systemic abnormalities in innate and acquired immunity play a role in its pathogenesis. The exact pathogenetic mechanism remains elusive. Evidence is accumulating that TNF-alpha, IL-17 and IL-23 signalling are highly relevant as targeting these pathways reduces disease activity. Evidence suggests a strong link between psoriasis and depression in adults. The International Psoriasis Council (IPC) held a roundtable event, “Psoriasis and Mental Health”, in Barcelona, Spain which focused on the presence of depression and suicidality, plus the role of neuroinflammation in psoriasis, sleep disruption and the impact of depression on cardiovascular disease outcomes. We summarize here the expert presentations to provide additional insight into the understanding of psychiatric comorbidities of psoriasis and of the impact of chronic, systemic inflammation on neuro- and cardiovascular outcomes. the associations between psoriasis and other psychiatric comorbidities are still controversial and warrant further attention.
Key words: psoriasis; depression, cardiovascular, mental health, sleep, neuroinflammation.
Accepted Nov 19, 2019; E-published Nov 19, 2019
Acta Derm Venereol
Corr: Luís Puig, Department of Dermatology, Hospital de la Santa Creu i Sant Pau, Sant Antoni Maria Claret 167, ES-08025 Barcelona, Spain. E-mail: LPuig@santpau.cat
Psoriasis is a chronic, systemic disease which is marked by a significant psychosocial burden. In recent years, multiple lines of evidence support the strong association between psoriasis and psychosocial comorbidities. The role of neuro-inflammation in psoriasis pathology, sleep disruption and the impact of depression on cardiovascular outcomes was explored in a workshop convened by the International Psoriasis Council. The workshop was assembled to increase the understanding of depression as an important comorbidity of psoriasis and elevate awareness of the impact of chronic, systemic inflammation on neuro- and cardiovascular outcomes. Studies discussed at this workshop suggest that depression is consistently associated with psoriasis, while suicidal ideation is not. Increased awareness of and concern about effective depression management in patients with psoriasis will undoubtedly improve overall disease management.
Psoriasis is a chronic inflammatory skin disorder with a broad and variable range of phenotypes, treatments, and associated comorbidities including metabolic syndrome (1), liver disease (2), respiratory disease (3), psoriatic arthritis (4), cardiovascular disease (5) and psychosocial disorders (6). It has been proposed that in psoriasis its cutaneous and specific systemic manifestations are driven by a shared pathogenic inflammatory mechanism.
Psoriasis provides an ideal model within which to study relationships between chronic inflammation and depression and other psychiatric co-morbidities. For clinical practice, greater awareness of the association between psoriasis and depression is important (6).
The term ‘depression’ covers a range of experiences, from low mood symptoms that may be a transient reaction to adverse life events to the enduring and potentially life threatening disorder. The latter is more accurately called Depressive Disorder (International Classification of Diseases [ICD-10]) or Major Depressive Disorder (MDD; Diagnostic and Statistical Manual of Mental Disorders [DSM-5]) (7, 8). Although these disorders are not identical constructs, they overlap to a consider-able extent and represent a common clinical syndrome characterized by sustained depressed mood and/or anhedonia (reduced motivation for or pleasure from previously enjoyable activities) and impairing somatic (sleep, energy, sensorimotor, appetites) and cognitive (self-esteem, concentration) functioning as well as the will to live (suicidal thinking and actions).
An influential current hypothesis of the neurobiology of MDD emphasizes a complex and interacting dysregulation of endocrine, immune, and monoamine neurotransmitter systems, often triggered initially by environmental stress but gradually becoming self-sustaining and resulting in impaired regional brain structure and function (9, 10).
Thus, chronic stress activates the hypothalamic-pituitary-adrenal (HPA) axis resulting in increased release of glucocorticoids from the adrenal cortex which, in turn, dysregulates amygdala function (Fig. 1) (10). The elevated adrenal activity and associated increase in sympathetic tone causes the release of proinflammatory cytokines which, along with the increased glucocorticoids, increase the activity of the enzyme monoamine oxidase (MAO) which in turn causes reduced levels of the monoamine neurotransmitters serotonin (5-HT), noradrenaline, and dopamine. The elevated cytokines and glucocorticoids also depress neurotrophic factors such as brain-derived neurotrophic factor (BDNF) resulting in decreased neuro-genesis in the hippocampus and reduced hippocampal volume. Amygdala and hippocampus dysregulation then maintains abnormal glucocorticoids, BDNF and cytokines, and increased proinflammatory cytokines give rise to physical illness symptoms and increased risk of inflammatory disorders such as cardiovascular disease (CVD).
Stress has been shown to trigger psoriasis onset and contribute to psoriasis flares in patients (6). The role of the HPA axis activity dysregulation and the link to the modulation of immune response in psoriasis have been explored (11, 12). Verhoeven et al. (13) demonstrated that flares of psoriasis are characterised by high activity of daily stressors and low cortisol levels. Furthermore, patients with persistently high levels of stressors have related lowered cortisol levels and may be particularly vulnerable to the influence of stressors on their psoriasis.
Fig. 1. Hypothalamic-pituitary-adrenal (HPA) axis and depression. BDNF: brain-derived neurotrophic factor; CRH: corticotropin-releasing hormone; DA: dopamine; 5HT: serotonin; NE: noradrenaline.
A number of changes in the HPA axis have been identified by neuroimaging. Molecular positron emission tomography (PET) studies during major depressive episodes (MDE), have found significantly elevated density of MAO-A – which could result in chronically low synaptic 5-HT levels through increased metabolism in a range of brain regions. Further evidence from PET studies demonstrates that 5-HT1A receptors (14) and 5-HT2A receptors (15, 16) are upregulated in MDD, suggesting an adaptive response to reduced 5-HT transmission, and that higher levels of 5-HT1A receptors predict higher suicidal ideation and attempts of greater lethality and intent (17).
Functional magnetic resonance imaging (fMRI) shows the amygdala is overly active in people with MDD when shown sad stimuli, but under-active when shown positive stimuli (18), suggesting a neural basis for the negative cognitive bias in MDD which is the therapeutic target of cognitive behavioural therapy.
Increasing evidence suggests involvement of inflammation in MDD in a proportion of individuals (19–22). Inflammatory disorders such as psoriasis are associated with a high prevalence of depression (23, 24). Similarly, symptoms of depression develop in a high proportion of patients administered pro-inflammatory cytokines for therapeutic reasons (25–27) and in healthy volunteers following peripheral immune challenges, such as vaccination or bacterial endotoxin injection, which result in a mild immune activation (28, 29). In MDD, several peripheral pro-inflammatory cytokines are elevated (30–33) and polymorphisms in inflammatory cytokine genes are associated with MDD and treatment response (34). Several PET studies have now investigated whether MDD is also associated with evidence for central neuroinflammation using tracers specific for the 18 kDA translocator protein (TSPO), a mitochondrial membrane protein which is over-expressed on activated microglia and, to a lesser extent, astrocytes. One study did not find elevated TSPO during a mild-to-moderate MDE (35). However, a subsequent study in more severely symptomatic patients (moderate-to-severe MDE) found significantly elevated TSPO, most prominent in prefrontal cortex, anterior cingulate cortex (ACC), and insula, and positively correlated with symptom severity (36). More recent data from a clinically and demographically comparable cohort of patients in a moderate-to-severe MDE replicates the TSPO elevation in the ACC, but suggests that microglial activation may be more strong-ly associated with the presence of suicidality than the diagnosis of MDD itself (37). These studies in working age adults with MDD are supported by the finding of elevated ACC TSPO in a recent small PET study in patients with late-life depression who had largely recovered from a depression episode but who had remaining evidence of peripheral inflammation (38). Thus, PET evidence for neuroinflammation in MDD, and potentially suicidality, seems to be converging on the ACC, a brain region playing an important role in regulating cognitive and emotional processing (39). Interestingly, no PET evidence for neuro-inflammation was found in non-depressed patients with moderate-to-severe plaque psoriasis and raised peripheral cytokines (40). However, a comparable study in depressed psoriasis patients has not yet been conducted, and the neurobiological mechanism underlying the increased incidence of depression in psoriasis remains to be elucidated.
More recently increased TSPO binding has been shown in the brains of patients with MDD and post hoc analysis extended these findings by demonstrating that this abnormality is significant in unmedicated but not in medicated MDD subjects (41). Moreover, in drug-naïve patients in a moderate-severe MDE, improvement in depressive symptoms following successful psychotherapy has been shown to be associated with a normalisation of elevated TSPO (42).
Depending on the screening method used, depression prevalence estimates vary between 9 and 55% of people with psoriasis (43, 44). One meta-analysis and systematic review estimated rates of clinical depression at 28% using questionnaires while estimates were 12% using International Classification of Diseases codes, 19% using Diagnostic and Statistical Manual of Mental Disorders IV, and 9% for antidepressant use (24). Psoriasis patients in this study had significantly more depressive symptoms (standardized mean differences 1.16; 95% confidence interval (CI) 0.67–1.66), and population-based studies showed that they were at least one and a half times more likely to experience depression (odds ratio [OR] 1.57; 95% CI 1.40–1.76) and used more antidepressant medication than did controls (OR 4.24, 95% CI 1.53–11.76) (Table I). In a multicentre study (45), 13.8% of patients with psoriasis reported depression symptoms using the Hospital Anxiety and Depression scale (HADS) versus 4.3% in controls (OR 2.40, 95% CI 1.67–3.47)).
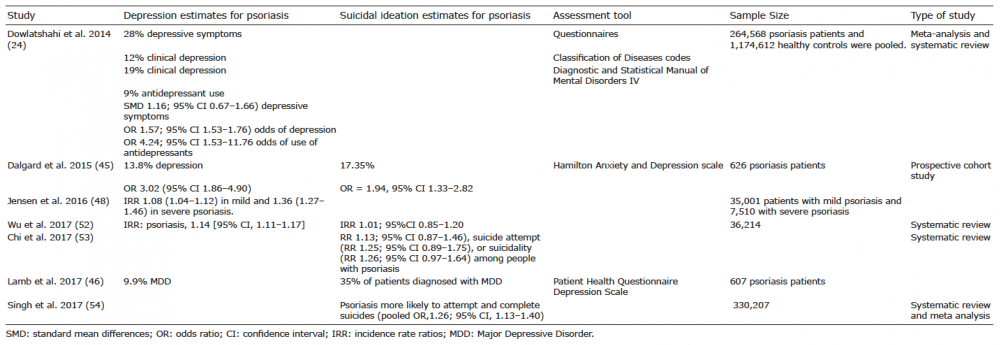
Table I. Psoriasis and psycho-comorbidity studies
Furthermore, in a study including 607 patients with psoriasis, 9.9% (95% CI: 7.5–12.3%) screened positive for MDD, measured using the (Patient Health Question-naire -9 items) PHQ-9 (46). Of these, 42% reported severe symptoms and 25% met criteria for urgent mental health specialist referral. Interestingly, in the 71% of patients from the cohort that identified with severe depression, this clinical finding was de novo. In the patient group diagnosed with MDD, 39% had a Dermatology Life Quality Index (DLQI) score <10 indicating low to medium impact of psoriasis on quality of life. Therefore, using the DLQI alone would potentially miss important depression symptoms that were detected by the PHQ-9.
Severity of psoriasis, as determined by a code for systemic medications, was found to be associated with higher risk of receiving a clinical diagnosis of depression, as evidenced by a hazard ratio of 1.72 (CI 1.57–1.88) in severe psoriasis compared to a hazard ratio of 1.38 (CI 1.35–1.40) in mild psoriasis (47). Depression may act as a trigger or exacerbating factor for psoriasis and may also be a consequence of the disease. Jensen et al. (48) examined the risk of new-onset depression in patients with psoriasis in a nationwide Danish cohort of 5 million people in the timeframe 2001–2011. In a total of 35,001 patients with mild psoriasis and 7,510 with severe psoriasis, incidence rates for depression were 20.0% (95% CI:19.9–20.0), 23.9% (23.1–24.7) and 31.6% (29.5–33.8) for the reference population, mild, and severe psoriasis, respectively. This finding indicates that in patients with severe disease new onset depression is more frequent.
In a Brazilian study, PASI (Psoriasis Area Severity Index), DLQI, State-Trait Anxiety Inventory (STAI) questionnaire, PHQ-9 and Holmes and Rahe Life Events scale were used to assess the total “load” of stressful life events in 119 psoriasis patients having experienced psoriasis for 3 years or more years and moderate severity (49). Salivary cortisol was assessed. The DLQI and stress questionnaire results demonstrated 20% of patients with depression, and nearly 20% of patients reported severe or very severe impact on QoL. The biometric study showed a positive correlation (r = 0.39, p < 0.001) between salivary cortisol values at bedtime and the PASI score.
The association of psoriasis with anxiety and psychological stress is well established. In order to evaluate psycho-logical impact, it is important to use instruments such as the HADS and PHQ-9, which are validated measures of anxiety and depressive symptomatology. Studies have demonstrated that using the DLQI to measure impact on life is not sufficient to identify depression as about one in 3 patients with MDD or major anxiety reported low to medium DLQI scores (46).
Effective biologic psoriasis treatments reduce signs and symptoms of psoriasis, lower disease impact (DLQI) and may also improve mental health outcomes (50, 51). Examination of depression through a prospective, longitudinal psoriasis registry (PSOLAR) demonstrated that treatment with biologics in moderate-to-severe psoriasis patients may reduce the risk of depressive symptoms (50). Similarly, a large cross-sectional study consisting of over 2 million patients with moderate-to-severe psoriasis demonstrated reduction of psychological stress and depression, in patients treated with biologics compared to those treated with oral therapies as measured by the Kessler Psychological Distress Scale- 6 (K6) and Patient Health Questionnaire-2 (PHQ2) tools (51).
The association between psoriasis, depression and suicidal ideation has been summarized in Table I. Depression and suicidal ideation tend to be more frequent in patients with severe disease. Although depression is consistently associated with psoriasis, suicidal ideation is not (52, 53). One cross-sectional multicentre study found that suicidal ideation was significantly associated with psoriasis (45) and some studies indicate that psoriasis is significantly linked to all 3 measures of suicidality (54), but the avail-able data on suicide attempts and death by suicide is limited and less consistent. Younger patients and patients with more severe psoriasis are at significantly higher risk of suicidality (54). Higher levels of psoriasis-related stressors and reduced QoL were significantly associated with suicidality in people with psoriasis.
A large population-based study utilizing a primary care database in the United Kingdom with linked hospital and mortality records indicated that the prevalence of depression was raised in patients with psoriasis and this may lead to a greater risk of self-harm. Nevertheless, the risk of suicide was lower in patients with psoriasis compared with those without psoriasis, and it was postulated that increased contacts with healthcare professionals for treatment of skin and coexistent depression may have ameliorated suicide risk (55).
Alexithymia, the difficulty in recognising and describing emotions as measured by the Toronto Alexithymia Scale (TAS-20), has been linked to psoriasis. The observed prevalence of alexithymia in patients with psoriasis ranges between approximately 15.6% and 33%, which is significantly higher than found among the general public (56–59). In a multicentre study which included 670 patients with psoriasis, the prevalence of alexithymia was 24.8% (95% CI: 21.7–28.2) (59). Some studies have shown that alexithymia is stable over time in the general population (60). However, it may be partly modifiable with therapeutic interventions, and reversal of alexithymia improves QoL, anxiety and depression (61, 62). It is likely that “trait alexithymia” and “state alexithymia” exist – the latter may be modified by therapeutic intervention or change in psychological status. It is important to identify alexithymic patients with psoriasis in clinical practice as they suffer from a higher disease burden, including significant impairment of QoL, higher levels of anxiety and depression, higher risk of alcohol dependency and impairment of work productivity, compared to patients without alexithymia (63).
Sleep is a complex behavioural and physiological process necessary for healthy functioning of the immune and metabolic systems, neuro-cognitive activity and emotional regulation. There is a large body of evidence demonstrating the vital role sleep has in maintaining health (64–66) and optimal physiological (67) and psychological functioning (68, 69). Persistent sleep disturbance is related to a number of medical illnesses including diabetes (70) and has established relationships with depression (71, 72).
Sleep disturbance is associated with a range of adverse health outcomes including elevated risk for a range of physical diseases, several of which people with psoriasis are already more susceptible to (e.g. diabetes (73), hyper-tension (74), CVD (75). Moreover, sleep disturbance increases risk of psychological illness (e.g. depression (72), anxiety (76)) and, over time, all-cause mortality (77).
Sleep disruption, including obstructive sleep apnoea (OSA), may contribute significantly to the health outcomes of psoriasis. A recent study (78) (186 respondents; mean age 39.2 years) assessed validated measures of sleep [Pittsburgh Sleep; Quality Index (PSQI), Berlin Questionnaire, Pre-Sleep Arousal Scale]; chronotype (Morningness-Eveningness Questionnaire); mood (Hospital Anxiety and Depression Scale); itch (5-D Itch Scale); and psoriasis severity (Simplified Psoriasis Index). The mean PSQI score was 9.2 ± 4.3, with 76.3% scoring above the threshold for poor sleep (≥ 6 on the PSQI) and 32.5% scoring ‘positive’ for probable OSA. Poor sleep and high likelihood of OSA were associated with more severe psoriasis (p < 0.05; η = 0.07; η2 = 0.005) (78). The precise mechanisms explaining the health outcomes and sleep link are not fully understood but are thought to include disrupted cortisol and cytokine production and changes in body temperature control all of which are implicated in psoriasis.
Not only is psoriasis accompanied by an increased risk of psychiatric comorbidities, but in particular when coupled with these comorbidities, such as depression, psoriasis promotes a greater risk of CVD events (79).
Due to the complex interaction of psoriasis and comorbidities, evidence is accumulating that psoriasis may trigger the metabolic syndrome and cardiovascular comorbidities. This relationship may be multifactorial, comprising lifestyles and systematic inflammation. Recently it was shown that blockade of IL12/23 reduced aortic vascular inflammation (80).
On the other hand these comorbidities may aggravate psoriasis. Recently, a Mendelian randomization study showed a causal relationship between body mass index (BMI) and psoriasis, whereas there was little support to a possible causal effect of psoriasis genetic risk (81).
The link between psoriasis, depression and CVD was investigated in a nationwide Danish cohort of patients with psoriasis (n = 29,406). Incidence rates were calculated, and incidence rate ratios (IRRs) adjusted for age, gender, socio-economic status, medication and comorbidity were estimated by Poisson regression models. Risk of myocardial infarction (MI) (IRR 1.57, 95% confidence interval (95% CI) 1.07–2.29), stroke (IRR 1.95, 95% CI 1.43–2.66), and death from CVD (IRR 2.24, 95% CI 1.53–3.26) were increased significantly during acute depression, and risk of stroke (IRR 1.51, 95% CI 1.19–1.90) was increased significantly in chronic depression. During remission from depression, only the risk of stroke was increased. In patients with psoriasis, depression is associated with increased risk of MI, stroke and death from CVD, especially during acute depression (82). These findings suggest that the added burden of comorbid depression in patients with psoriasis confers a greater risk of major adverse CVD events.
To further understand whether the impact of psoriasis and comorbid depression occurred prior to CVD events, 36 patients with psoriasis and reported comorbid depression and 36 age- and sex-matched patients with psoriasis but no reported history of psychiatric illness were enrolled in a study for quantifying vascular inflammation and coronary CT angiography using 18-FDG PET/CT (83). Patients with psoriasis and comorbid depression experienced both greater vascular inflammation and greater total and non-calcified coronary plaque burden when compared to psoriasis patients without comorbid psychiatric illness. These differences remained significant after adjustment for age, sex and Framingham risk score, suggesting that comorbid depression in psoriasis contributes to CVD risk beyond what can be attributed to traditional cardiovascular risk factors.
Additionally, a prospective cohort study demonstrated that chronic psychological stress increases neural activity, as measured by amygdala activity, in patients with severe psoriasis disease compared to healthy volunteers (84). Elevated neural activity was found to significantly contribute to the risk of subclinical CVD in patients with psoriasis. Skin clearance after one year of treatment corresponded with reduction of amygdala activity and subclinical CVD factors. Taken together, these studies highlight the strong link between psychological stress and CVD morbidity in psoriasis.
Unfortunately, so far no predictive models nor biomarkers are available to predict the course of the disease and in particular the development of comorbidities. Several studies however suggest that predictive models may become available in the near future. For example, a genome-wide analysis of the British Association of Dermatologists Biologics and Immunomodulators Register (BADBIR) revealed that HLA-C*06:02-negative patients responded better to adalimumab, whereas HLA-C*06:02-positive patients responded better to treatment with ustekinumab (85). Another analysis of this registry indicated that various baseline clinical characteristics predict response to treatment with biologics (86).
Psoriasis, depression and CVD are associated and are probably connected through systemic inflammation; neuroimaging has provided evidence for the common inflammatory pathway connecting these conditions. The interaction of psychological stress with the inflammatory state of psoriasis and depression is complex and poorly understood. Stressful life events can trigger onset, exacerbate and initiate flares of psoriasis. In addition, social interactions, economic challenges, and negative behaviours (alcohol and smoking) also contribute to the complex interactions of these conditions.
The association between psoriasis and distress is broader than depression alone. Psychological stress and anxiety are also well established features in many
patients with psoriasis and are aggravating or precipitating factors of depression. Alexithymia, which is also linked to depression, warrants further investigation. Of note, the association between psoriasis and death by suicide may be a matter of debate but suicidal ideation is more frequently associated with psoriasis.
The impairment of patient QoL by psoriasis is common knowledge and is of major importance in the assessment of treatment outcomes. However, awareness of the association of psoriasis with depression, although established in epidemiological studies, is less well-recognised and addressed in the clinic. Early diagnosis of depression through validated tools and insight into related psychological/psychiatric disorders should form important targets in the treatment of patients with psoriasis.
Increased awareness of and concern about effective depression management in patients with psoriasis will undoubtedly improve overall disease management. Quick and easy to perform screening tools for depression and suicidal ideation are necessary if we hope to add depression screening to our clinical repertoire for managing psoriasis patients. For example, The PHQ-2 is a validated measure that screens for depressed mood and anhedonia over the past 2 weeks and includes the first two questions of the PHQ-9 and may prove useful for mood assessment. Many dermatologists report feeling ill-equipped to address psychological/psychiatric comorbidity in the clinic so implementation of resources to increase the accessibility of psychological support and psychiatric referral in dermatologic practices, and especially in the setting of psoriasis dedicated units in referral centers is key. Further research is needed in order to understand how targeting specific pro-inflammatory cytokines which underlie the chronic inflammation of psoriasis affects both CVD events and depression.
Disclosures: CEK has received grants and/or honoraria or consultation and/or research support and/or participated in clinical trials sponsored by Abbvie, Almirall, Celgene, Janssen, Leo-Pharma, Lilly, Merck-Serono, Novartis, Pfizer, UCB. CEK is supported by the NIHR Manchester Biomedical Research Centre. PST has received consulting fees from Galen Limited; Sunovion Pharmaceuticals Europe Ltd; myTomorrows; LivaNova UK Ltd. TA has no conflicts of interest to declare. NNM is a full-time US government employee and has served as a consultant for Amgen, Eli Lilly, and Leo Pharma receiving grants/other payments; as a principal investigator and/or investigator for AbbVie, Celgene, Janssen Pharmaceuticals, Inc, and Novartis receiving grants and/or research funding; and as a principal investigator for the National Institute of Health receiving grants and/or research funding. FS has acted as a consultant for Abbvie, Eli Lilly, Janssen, Pierre Fabre. PvdK received compensation for consultancy services and presenteations from Celgene, Allmirall, Abbvie, Lilly, Novartis, Janssen, Leo, Bristol Mayer Squibb, Dermavant and UCB. ABKl has received compensation as a consultant and an investigator for Novartis, Abbvie, UCB, Lilly, and Janssen and has received fellowship funding from Janssen and Abbvie. CB has received funding for research or honoraria from Abbvie; Almiral; Celgene; Janssen; Lilly; Novartis; Pfizer. CEMG has received grants and/or honoraria or consultation fees from Abbvie, Almirall, BMS, Celgene, Galderma, GSK, Janssen, LEO-Pharma, Lilly, Novartis, Pfizer and UCB Pharma. CEMG is funded in part by the NIHR Manchester Biomedical Research Centre and by MRC grant MR/1011808/1and is an NIHR Emeritus Senior Investigator. FV has received grants and/or honoraria or consultation fees and/or research support and/or participated in clinical trials sponsored by Abbvie, Amgen, Janssen, Leo-Pharma, Lilly, Novartis, Pfizer. JMvdW has no conflicts of interest to declare. DA has received research grants from Abbvie, Almirall, Celgene, Eli Lilly, Novartis, UCB and the Leo Foundation. LP has received grants and/or honoraria or consultation fees and/or research support and/or participated in clinical trials sponsored by Abbvie, Almirall, Amgen, Baxalta, Biogen, Boehringer Ingelheim, Celgene, Gebro, Janssen, Leo-Pharma, Lilly, Merck-Serono, MSD, Novartis, Pfizer, Regeneron, Roche, Sandoz, Sanofi, UCB and has participated in speaker’s bureau for Celgene, Janssen, Lilly, MSD, Novartis, Pfizer.
Funding: AbbVie provided an educational grant to the International Psoriasis Council to support the symposium. This sponsor had no influence on the content and viewpoints in this manuscript.