Hereditary Leiomyomatosis and Renal Cell Cancer
Anders Würgler Hansen1, Zahraa Chayed1, Kristine Pallesen2, Ileana Codruta Vasilescu3 and Anette Bygum2
1Faculty of Health Sciences, University of Southern Denmark, 2Department of Dermatology and Allergy Centre, Odense University Hospital, and 3Department of Pathology, Odense University Hospital, Odense, Denmark
Hereditary leiomyomatosis and renal cell cancer is a genodermatosis with an autosomal dominant inheritance pattern. It is a tumour predisposition syndrome characterized by cutaneous and uterine leiomyomas, and increased susceptibility to develop renal cell carcinoma. There are 200–300 families with hereditary leiomyomatosis and renal cell carcinoma reported worldwide, but the syndrome is believed to be underdiagnosed. Cutaneous leiomyomas are small smooth muscle tumours that tend to grow over time. Larger lesions, in particular, can cause pain or itching. Uterine leiomyomas have a high penetrance in women with hereditary leiomyomatosis and renal cell cancer. They frequently cause symptoms, and surgical intervention is often necessary. Hereditary leiomyomatosis and renal cell cancer-associated renal cell carcinomas have a high potential to metastasize. Patients are diag-nosed by genetic testing if a pathogenic mutation is demonstrated in the gene encoding fumarate hydratase. Immunohistochemistry may be a useful diagnostic approach in patients without a detectable pathogenic mutation. Diagnosed patients should be monitored for renal tumours in a lifelong surveillance programme.
Key words: hereditary leiomyomatosis; cutaneous leiomyomas; uterine leiomyomas; renal cell carcinoma; cancer surveillance.
Accepted Oct 28, 2019; E-published Oct 30, 2019
Acta Derm Venereol 2020; 100: XX–XX.
Corr: Anders Würgler Hansen, Medical Student, Faculty of Health Sciences, University of Southern Denmark, Kloevervaenget 24A 2, DK-5000 Odence C, Denmark. E-mail: anders.wurgler.hansen@rsyd.dk
Hereditary leiomyomatosis and renal cell cancer (HLRCC) is an inherited tumour predisposition syndrome. Around 75% of individuals with HLRCC develop cutaneous leiomyomas, which are skin tumours that can cause pain and itching. Most women with HLRCC develop uterine leiomyomas that often cause gynecological symptoms and typically require surgery. Around 20% develop renal cell carcinoma. HLRCC-associated renal cell carcinomas are aggressive tumours with a high potential to metastasize. Individuals with features suggestive of HLRCC and at-risk family members should undergo genetic testing. Individuals harbouring a pathogenic mutation should be offered lifelong surveillance so renal neoplasms are detected and treated in time.
Hereditary leiomyomatosis and renal cell cancer (HLRCC) is a rare genodermatosis with an autosomal dominant inheritance pattern, caused by inherited or de novo mutations in the gene encoding fumarate hydratase (FH) (1). HLRCC is a tumour predisposition syndrome characterized by the propensity to develop single or multiple cutaneous leiomyomas (CLM), uterine leiomyomas (ULM), and renal cell carcinomas (RCC). Blum & Jean (2) linked leiomyomas of the skin with uterine leiomyomas for the first time in 1954. In the literature, the syndrome is referred to as Reed’s syndrome, multiple cutaneous and uterine leiomyomatosis (MCUL), and leiomyomatosis cutis et uteri, amongst other names (3). The eponym Reed’s syndrome dates back to 1973, when Reed and colleagues noticed an accumulation of the condition in 2 families with an autosomal dominant inheritance pattern (4). The syndrome was subsequently renamed HLRCC in 2001, when the condition was linked with an increased susceptibility to certain subtypes of RCC (5).
The exact prevalence of HLRCC is unknown; however, 200–300 families have been reported in the literature (1, 3). Mostly Western-European, Finnish and North-American families have been reported (6–8). Gardie et al. reported 44 families with confirmed HLRCC in France (9). Toro et al. reported 35 HLRCC families in North America (7), where Wei et al. (10) later reported an additional 21 families. Lehtonen et al. (6) reported 7 Finnish families with HLRCC. Reports of Colombian, Japanese, Indian, Chinese and African-American HLRCC families suggest that the syndrome occurs worldwide (10–14). HLRCC is believed to be an underdiagnosed syndrome, and the actual number of HLRCC families is likely to be higher (8).
The genetic predisposition to CLM, ULM and RCC is caused by mutations in the FH-gene on chromosome 1q (5). HLRCC is an autosomal dominant disease with sporadic cases reported (8, 15).
FH acts as a tumour suppressor gene in accordance with Knudson’s 2-hit hypothesis (5, 16). Tumour tissue displays biallellic FH inactivation where an acquired somatic FH mutation can be demonstrated in addition to the inherited germline mutation (17, 18). An excess of 200 unique potential pathogenic FH variants have been reported (19). The gene product is the enzyme fumarate hydratase or fumarase, which catalyses the conversion of fumarate to malate in the tricarboxylic acid cycle (TCA) (20). An inactivating mutation, most commonly a missense mutation of the wild type allele, leads to decay of the mRNA or truncation of the gene product, resulting in an either markedly reduced or absent enzyme activity (7, 10, 21–23). Fumarate accumulates in cells in the absence of FH (24). The mechanism leading to tumourigenesis is poorly understood, although hypoxia inducible factors (HIF) in the hypoxia path-way are hypothesized to play a role. Fumarate inhibits HIF prolyl hydroxylase (HPH), an enzyme that catalyses the degradation of HIF, leading to elevated intracellular levels of HIF (25). HIF-1α, HIF-2α and HIF-1β promotes the transcription of target genes involved in angiogenesis, cell proliferation and cell survival (26). Direct sequencing reveals a pathogenetic FH germline mutation in 71–100% of families with clinically suggestive HLRCC (3, 8, 9, 18). In cases without detectable pathogenic FH mutations, a reduced or absent FH activity may be detected in tumour tissue by a biochemical assay (22, 27, 28). Whole-gene deletions, exon deletions and large rearrangements have rarely been demonstrated in HLRCC individuals without detectable FH mutations (3, 9, 20, 21, 29).
HLRCC displays a broad clinical spectrum, as some cases with FH mutations are asymptomatic while others have severe cutaneous, uterine or renal manifestations (9, 21). The penetrance of CLMs has been reported to be higher in men with FH mutations compared with women, as a study reported that CLMs were present in all men by age 35 years, while being present in only 55% of women (6). Predicting the phenotype based on a specific inherited gene variant is not possible (1, 9, 23). Due to recruitment of individuals based on positive findings in studies and publications of HLRCC, the prevalence of clinical manifestations might be overestimated (7, 8, 10).
Cutaneous leiomyomas
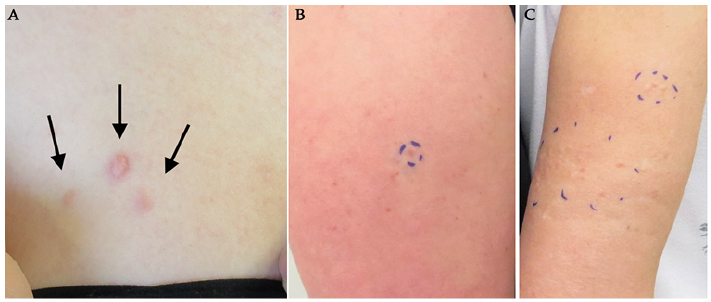
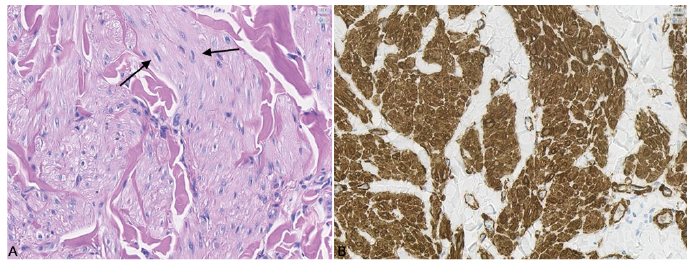
CLMs are the most frequent manifestation of disease leading to a diagnosis (8). They are benign, firm, smooth, skin-coloured to erythematous or hyperpigmented papulonodules (3, 8, 30) (Figs 1 and 2). CLMs range in size between 2 and 20 mm in diameter (3, 8). Histologically, CLMs are subdivided into piloleiomyomas, genital leiomyomas and angioleiomyomas. Piloleiomyomas, being the most frequent in relation to HLRCC, emerge from the arrector pili muscles of hair follicles (Fig. 3) (3). Angio-leiomyomas are derived from the vascular smooth muscle tissue in the tunica media of blood vessels (31). Genital leiomyomas originate from the dartoic smooth muscle tissue of the vulva, scrotum and nipple-areola complex (31, 32). While angioleiomyomas and genital leiomyomas are both rare, the former is often painful and the latter painless (3, 31). Piloleiomyomas can be multiple or solitary (3, 8). They are usually located on extensor surfaces of the trunk, upper/lower extremities, shoulders and, less frequently, on the face and neck (3, 8, 30). Multiple lesions can be described as clustered or scattered, while segmental, zosteriform, linear, and disseminated distributional patterns have also been reported (3, 8, 30). Tumors are usually bilateral, but can be unilateral or symmetrical (3, 8). CLMs appear in 68–84% of HLRCC patients, and up to 100% of HLRCC families (9, 10, 15, 21). In 9–15% of individuals they are the only clinical manifestation of the condition (7, 8, 15, 23). They initially appear in the 2nd to 4th decade, with a mean age at onset of 24–30 years, although they have been reported in a patient as young as 9 years of age (7, 8, 23). Approximately 75–90% of HLRCC individuals experience variable itching or pain from their skin lesions, which may be provoked by direct contact, emotions, or fluctuations in temperature or pressure (3, 7, 8, 30). The number of CLMs varies widely among affected individuals, ranging from a single lesion to more than 100 (7, 8). Lesions generally increase in number and size over time, and especially larger lesions tend to be symptomatic (15, 21). Individuals with CLMs have reported a moderate to severe negative impact on their quality of life caused by their skin lesions (8). The potential of cutaneous and uterine leiomyomas to transform into leiomyosarcomas is not well established. Only 6 cases of cutaneous leiomyosarcomas have been reported in FH mutation carriers (7, 10, 23, 33, 34), 2 of which presented with rapid growth of an existing CLM (23). Similarly, uterine leiomyosarcomas have rarely been linked to HLRCC (4–6, 35). Leiomyosarcomas are difficult to distinguish clinically from CLMs, but may be larger, ulcerated, irregularly shaped and increasingly painful (3). Histopathological examination of tumour tissue is required for a firm diagnosis (36). These tumours rarely metastasize (3). Although speculative, looser diagnostic criteria of leiomyosarcomas in the past may have led to uterine and cutaneous leiomyomas being mistaken for leiomyosarcomas (23).
Uterine manifestations
Uterine fibroids range in number between 1 and 20, and in diameter between 1 and 10 cm (7, 10). HLRCC-associated ULMs are diagnosed in the 2nd to 5th decade, with a mean age of 30 years (6–8, 10). ULMs occur in 73–100% of HLRCC families and in 76–100% of women with HLRCC (7–10, 15, 21, 23). In 7–14% of cases, ULMs are the only disease manifestation (8, 10). The mean age at diagnosis of ULMs is 28–30 years, ranging from 18 to 53 years (7, 8, 10, 37). In the general public, the prevalence of symptomatic uterine fibroids is 9% (38), and they are diagnosed approximately 10 years later than in women with HLRCC (37). The majority of women with HLRCC-associated ULMs experience gynaecological symptoms, most commonly dysmenorrhea, followed by menorrhagia and irregular menses (7, 8, 21, 37). Women with HLRCC often experience gradual worsening of these symptoms prior to diagnosis (8). HLRCC-associated ULMs are associated with female infertility characterized by difficulty achieving conception and occurrence of miscarriages (8). Up to 91% of women with a pathogenic FH mutation undergo surgical intervention, such as hysterectomy or myomectomy, at a mean age of 35–36 years (7, 10, 23), and many undergo surgery before the age of 30 years (7, 10). HLRCC-associated ULMs are associated with various degrees of negative impact on quality of life (8).
Renal manifestations
HLRCC-associated RCC display a broad spectrum of architectural growth patterns, including papillary, tubulo-papillary, tubular, solid and cystic elements (10, 23, 39–41). The syndrome mainly predisposes to RCCs of a type 2 papillary morphology (PRCCII), but tumours of collecting duct, clear cell, sarcomatoid and oncocytic origin have also been reported (7, 9, 22, 23, 40). RCCs are predominantly solid and unilateral, but can also be multifocal and bilateral (10, 14, 40, 42). Tumour cells have large nuclei, with prominent inclusion-like eosinophilic nucleoli, surrounded by a perinuclear clear halo of cyto-plasm (40, 43). Renal tumours vary in size between 2 and 22 cm in diameter (5, 7, 8). RCCs usually display an aggressive growth pattern, with invasion of nearby tissue, and a high potential to metastasize (14, 23, 44). Symptoms include haematuria, flank pain, lower back pain, palpable mass and symptoms from metastases (3). Patients can debut with RCC as the only clinical manifestations of the syndrome (10, 45). HLRCC-associated RCCs have a poor prognosis, with a 5-year survival of 31%, as reported by Toro et al. (7). Furthermore, Muller et al. reported a median survival of 18 months for metastatic disease (23). RCC is diagnosed in approximately 14–62% of HLRCC families (7, 9, 10), and in 16–24% of individuals with HLRCC (7, 9, 10, 23). However, a Dutch study found that only 6% of patients with HLRCC were diagnosed with RCC (21). The mean age at diagnosis of HLRCC is 39–46 years (range 10–90 years) (6–9, 14, 41, 46, 47), approximately 20–25 years earlier than the diagnosis of sporadic RCC in the general European and American population (48, 49).
The need for treatment of CLMs is individual and depends mainly on pain and cosmetic appearance of the lesions. Conservative approaches involve avoiding symptomatic triggers, such as direct contact and changes in temperature (3). Issues of cosmetic appearance might be solved by choice of clothing and use of make-up (3). CLMs can readily be removed by standard excision, electrodessication, CO2 laser ablation or cryotherapy (3, 21). The choice of surgical intervention depends largely on the preferences of the clinician. However, the indication for cosmetic removal of CLMs should be weighed against the risk of scarring and keloids (Fig. 2).
Topical treatment by lidocaine or botulinum toxin may offer pain relief in symptomatic lesions (3). Systemic pharmacological treatment with nitroglycerine, nifedipine, gabapentin, phenoxybenzamine, and doxazocin is sometimes attempted to relieve pain (3, 21, 50).
Gonadotropin-releasing hormone agonists and progesterone-releasing intrauterine devices can be used as medical treatment for ULMs (3). Surgical interventions are most commonly myomectomy and hysterectomy. Myomectomy is a uterus-preserving surgical intervention, with removal of the fibroids from the uterus (50). Other surgical interventions include uterine artery embolism and electrosurgery (3, 8, 10). Patients are counselled on family planning prior to choice of treatment (21).
Due to the often aggressive growth pattern of HLRCC-associated RCCs, surgical intervention is recommended even in small tumours, with extirpation of all neoplastic tissue and possibly retroperitoneal lymph node dissection (47). If possible, nephron-sparing surgery with partial nephrectomy is preferred in order to preserve renal function (47). There is no standard treatment option for metastatic disease, and very limited treatment data avail-able (51). Medical treatment options usually interact with components of the mammalian target of rapamycin (mTOR) pathway and the HIF pathway, including vascular endothelial growth factor (VEGF), platelet-derived growth factor (PDGF) and epidermal growth factor (EGF) (47, 51). The most commonly prescribed drugs targeting these pathways are bevacizumab, temsirolimus, everolimus, pazopanib, axitinib, sunitinib, sorafenib and erlotinib (47, 51). These agents may be used in combination, in order to achieve the best response (47, 51, 52). Choice of treatment modality depends largely on patient preferences and comorbidities (3). Bevacizumab in combination with erlotinib showed promising results in the treatment of metastasized HLRCC-associated RCC (51, 52). There is currently ongoing research of the use of inhibitors of glycolysis in the treatment of HLRCC-associated RCC, as the tumour cells are dependent on glycolysis for ATP production due a TCA cycle defect (47, 53). However, such therapies have not yet proven effective (54).
A diagnosis of HLRCC is confirmed through genetic testing (50). Routine molecular screening of ULM tissue has been suggested (55, 56). Random inactivation of FH is a commonly seen phenomenon in sporadic ULMs (57, 58). This is due to somatic biallelic inactivation rather than germline mutations (57, 58). Therefore, screening of ULM tissue for FH-deficiency was deemed impractical in individuals without features suggestive of HLRCC (57, 59). Pathological screening of ULM morphology was recently proposed to trigger genetic testing, in cases suggestive of FH deficiency (60). This strategy might help to detect women eligible for genetic counselling (60).
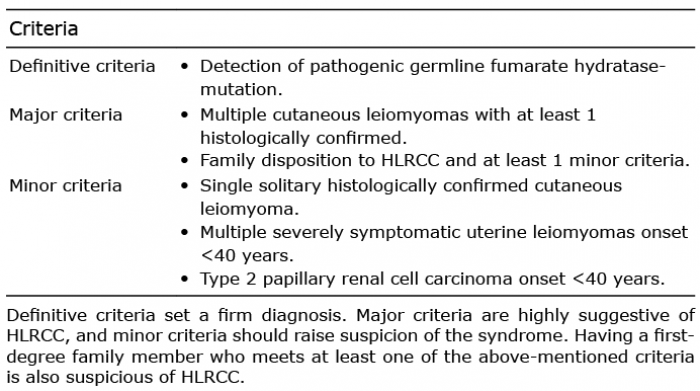
Immunohistochemical (IHC) examination of neoplasms associated with HLRCC can support the diagnosis in cases where a pathogenic germline mutation is not known (47, 59, 61). In addition, IHC examination plays an important role in differentiating HLRCC-associated RCC from other high-grade RCCs (39, 41, 59, 61). Alterations of succinate dehydrogenase (SDH), an acid cycle enzyme linked to renal tumors, cannot be demonstrated by IHC staining of FH-deficient tumor tissue (62). However, loss of FH expression in tumour tissue can be identified by absent FH staining (59). S-(2-succinyl) cysteine (2SC) is another highly specific IHC biomarker in detecting HLRCC-associated RCC (39, 41, 59). 2SC is produced in a process termed protein succination, wherein high levels of fumarate interact with cysteine sulphydryl groups of cellular proteins to form a stable chemical modification (61). Absence of FH staining and/or presence of 2SC staining in tumour tissue is strongly correlated with HLRCC (39, 41, 59, 61, 63). While IHC examination alone cannot replace genetic testing, it may contribute to weakening or strengthening the suspicion of HLRCC (62, 64). Immunostaining of CLMs has been suggested as a routine screening tool for HLRCC (62, 65, 66). However, Harvey & Wood argue that, compared with immunostaining techniques, the very presence of multiple CLMs is more cost-effective and has a higher sensitivity for an underlying germline mutation while the specificity is unestablished (67). A revised proposal for diagnostic criteria of HLRCC is shown in Table I (1, 3, 9, 21, 50).
The differential diagnostic considerations depend on the clinical findings. CLMs are rare and their presence should always lead to a suspicion of HLRCC (1, 43, 68). A large number of skin tumours may cause pain (69). The most relevant differential diagnostic considerations to painful CLMs are shown in Table II (3, 30, 69–71). Although the clinical spectrum of CLMs is broad, many of these tumours can readily be eliminated as likely differential diagnoses based on the clinical findings. A biopsy is required for a firm diagnosis (30).
ULMs are frequent in the general population and constitute the most common pelvic tumour in women (72).
The main differential diagnoses in relation to renal tumours are the autosomal dominant renal cancer syndromes: hereditary papillary renal cancer (HPRC), Von Hippel-Lindau syndrome (VHL) and Birt-Hogg-Dube syndrome (BHDS) (73). Predisposition to papillary type 1 RCC is the only manifestation of HPRC (1). VHL is characterized by clear cell RCC and renal cysts (74). Other common findings include central nervous system haemangioblastoma, pancreatic tumours and cysts, and pheochromocytoma among others (74). VHL can be differentiated from HLRCC by the lack of cutaneous and uterine lesions (1). BHDS is associated with lung cysts, that may erupt and cause pneumothorax, and a triage of skin lesions, including fibrofolliculomas, trichodiscomas and acrochordons (skin tags) (75). Distinctive from CLMs, fibrofolliculomas and trichodiscomas are painless, pale, millimetre small lesions, and are mainly located on the face, neck and upper torso (75). The renal tumours seen in BHDS constitute in a wide histological spectrum. Patients most often present with hybrid tumours, a combination of chromophobe RCC and renal oncytoma, but also chromo-phobe RCCs, clear cell RCCs or renal oncocytomas are frequently associated with BHDS (75). BHDS is not associated with an increased frequency of ULMs (1).
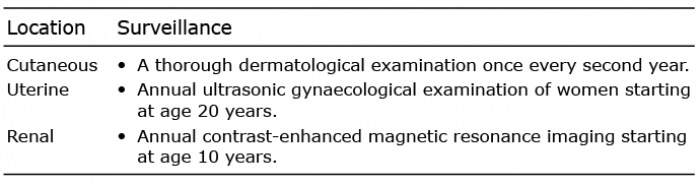
There is a lack of consensus regarding a surveillance programme of pathogenic FH-mutation carriers (30). Al-though suspected, a firm association of cutaneous leiomyosarcomas with HLRCC has not been established (23). We recommend a thorough dermatological examination every second year, starting from the onset of CLMs (Table III). Patients should be instructed to seek medical attention in case of rapid growth in skin lesions. Annual ultrasonic gynaecological examinations starting at the age of 20 years, in FH mutation carriers, is recommended in order to diagnose and monitor asymptomatic ULMs (Table III) (3, 21, 50). Prevention of RCCs is a major focus of the surveillance programme (21). Renal surveillance by annual contrast-enhanced magnetic resonance imaging (MRI) is proposed to start at the age of 10 years by Patel et al. (3), and at the age of 8 years by Schmidt & Linehan (50). Due to numerous reports of HLRCC-associated RCC in individuals younger than 20 years of age (8, 40, 46, 76, 77), the youngest reported at age 10 (30), we propose annual MRI scans starting at age 10 years (Table III). While renal ultrasound has been suggested to play a role in assisting MRI in the surveillance programme (21), Schmidt & Linehan (78) does not recommend this modality for routine screening of HLRCC-associated renal tumours. Furthermore, family members of patients with proven HLRCC should undergo early genetic testing in order to be included in the surveillance programme at an early age (1, 78).
The prognosis of HLRCC depends first and foremost on the detection of HLRCC-associated renal cancers. It is imperative to diagnose the syndrome early, and include patients in an aggressive surveillance programme, so that renal tumours are diagnosed and treated in time.
At-risk family members and offspring of confirmed FH-mutation carriers should undergo genetic testing in order to identify the necessity for inclusion in the surveillance programme. HLRCC patients and at-risk family members should be offered genetic counselling and be provided with information regarding the syndrome (1). FH mutation carriers should ideally receive genetic counselling before starting a family, in order to discuss the following prior to pregnancy; fertility issues, prenatal testing options, and risk-assessments with regards to passing on the pathogenic gene variant to offspring (1).
The authors have no conflicts of interest to declare.
- Pithukpakorn M, Toro JR. Hereditary leiomyomatosis and renal cell cancer. In: Adam MP, Ardinger HH, Pagon RA, Wallace SE, Bean LJH, Stephens K, et al., editors. GeneReviews((R)). Seattle (WA) 2015.
View article Google Scholar - Blum P, Jean L. Leiomyome eruptif de Besnier. Bull Soc Fr Dermatol Syphiligr 1954; 61: 349–350.
View article Google Scholar - Patel VM, Handler MZ, Schwartz RA, Lambert WC. Hereditary leiomyomatosis and renal cell cancer syndrome: an update and review. J Am Acad Dermatol 2017; 77: 149–158.
View article Google Scholar - Reed WB, Walker R, Horowitz R. Cutaneous leiomyomata with uterine leiomyomata. Acta Derm Venereol 1973; 53: 409–416.
View article Google Scholar - Launonen V, Vierimaa O, Kiuru M, Isola J, Roth S, Pukkala E, et al. Inherited susceptibility to uterine leiomyomas and renal cell cancer. Proc Natl Acad Sci U S A 2001; 98: 3387–3392.
View article Google Scholar - Lehtonen HJ, Kiuru M, Ylisaukko-Oja SK, Salovaara R, Herva R, Koivisto PA, et al. Increased risk of cancer in patients with fumarate hydratase germline mutation. J Med Genet 2006; 43: 523–526.
View article Google Scholar - Toro JR, Nickerson ML, Wei MH, Warren MB, Glenn GM, Turner ML, et al. Mutations in the fumarate hydratase gene cause hereditary leiomyomatosis and renal cell cancer in families in North America. Am J Hum Genet 2003; 73: 95–106.
View article Google Scholar - Alam NA, Barclay E, Rowan AJ, Tyrer JP, Calonje E, Manek S, et al. Clinical features of multiple cutaneous and uterine leiomyomatosis: an underdiagnosed tumor syndrome. Arch Dermatol 2005; 141: 199–206.
View article Google Scholar - Gardie B, Remenieras A, Kattygnarath D, Bombled J, Lefevre S, Perrier-Trudova V, et al. Novel FH mutations in families with hereditary leiomyomatosis and renal cell cancer (HLRCC) and patients with isolated type 2 papillary renal cell carcinoma. J Med Genet 2011; 48: 226–234.
View article Google Scholar - Wei MH, Toure O, Glenn GM, Pithukpakorn M, Neckers L, Stolle C, et al. Novel mutations in FH and expansion of the spectrum of phenotypes expressed in families with hereditary leiomyomatosis and renal cell cancer. J Med Genet 2006; 43: 18–27.
View article Google Scholar - Arenas Valencia C, Rodriguez Lopez ML, Cardona Barreto AY, Garavito Rodriguez E, Arteaga Diaz CE. Hereditary leiomyomatosis and renal cell cancer syndrome: identification and clinical characterization of a novel mutation in the FH gene in a Colombian family. Fam Cancer 2017; 16: 117–122.
View article Google Scholar - Kamai T, Abe H, Arai K, Murakami S, Sakamoto S, Kaji Y, et al. Radical nephrectomy and regional lymph node dissection for locally advanced type 2 papillary renal cell carcinoma in an at-risk individual from a family with hereditary leiomyomatosis and renal cell cancer: a case report. BMC Cancer 2016; 16: 232.
View article Google Scholar - Soni SS, Gowrishankar S, Adikey GK, Raman AS. Hereditary leiomyomatosis with renal cell carcinoma. Indian J Dermatol Venereol Leprol 2008; 74: 63–64.
View article Google Scholar - Wong MH, Tan CS, Lee SC, Yong Y, Ooi AS, Ngeow J, et al. Potential genetic anticipation in hereditary leiomyomatosis-renal cell cancer (HLRCC). Fam Cancer 2014; 13: 281–289.
View article Google Scholar - Alam NA, Bevan S, Churchman M, Barclay E, Barker K, Jaeger EE, et al. Localization of a gene (MCUL1) for multiple cutaneous leiomyomata and uterine fibroids to chromosome 1q42.3–q43. Am J Hum Genet 2001; 68: 1264–1269.
View article Google Scholar - Kiuru M, Launonen V, Hietala M, Aittomaki K, Vierimaa O, Salovaara R, et al. Familial cutaneous leiomyomatosis is a two-hit condition associated with renal cell cancer of characteristic histopathology. Am J Pathol 2001; 159: 825–829.
View article Google Scholar - Knudson AG, Jr. Mutation and cancer: statistical study of retinoblastoma. Proc Natl Acad Sci U S A 1971; 68: 820–823.
View article Google Scholar - Lehtonen HJ. Hereditary leiomyomatosis and renal cell cancer: update on clinical and molecular characteristics. Fam Cancer 2011; 10: 397–411.
View article Google Scholar - Bayley JP, Launonen V, Tomlinson IP. The FH mutation database: an online database of fumarate hydratase mutations involved in the MCUL (HLRCC) tumor syndrome and congenital fumarase deficiency. BMC Med Genet 2008; 9: 20.
View article Google Scholar - Tomlinson IP, Alam NA, Rowan AJ, Barclay E, Jaeger EE, Kelsell D, et al. Germline mutations in FH predispose to dominantly inherited uterine fibroids, skin leiomyomata and papillary renal cell cancer. Nat Genet 2002; 30: 406–410.
View article Google Scholar - Smit DL, Mensenkamp AR, Badeloe S, Breuning MH, Simon ME, van Spaendonck KY, et al. Hereditary leiomyomatosis and renal cell cancer in families referred for fumarate hydratase germline mutation analysis. Clin Genet 2011; 79: 49–59.
View article Google Scholar - Alam NA, Rowan AJ, Wortham NC, Pollard PJ, Mitchell M, Tyrer JP, et al. Genetic and functional analyses of FH mutations in multiple cutaneous and uterine leiomyomatosis, hereditary leiomyomatosis and renal cancer, and fumarate hydratase deficiency. Hum Mol Genet 2003; 12: 1241–1252.
View article Google Scholar - Muller M, Ferlicot S, Guillaud-Bataille M, Le Teuff G, Genestie C, Deveaux S, et al. Reassessing the clinical spectrum associated with hereditary leiomyomatosis and renal cell carcinoma syndrome in French FH mutation carriers. Clin Genet 2017; 92: 606–615.
View article Google Scholar - Isaacs JS, Jung YJ, Mole DR, Lee S, Torres-Cabala C, Chung YL, et al. HIF overexpression correlates with biallelic loss of fumarate hydratase in renal cancer: novel role of fumarate in regulation of HIF stability. Cancer Cell 2005; 8: 143–153.
View article Google Scholar - Henegan JC, Jr., Gomez CR. Heritable cancer syndromes related to the hypoxia pathway. Front Oncol 2016; 6: 68.
View article Google Scholar - Semenza GL. Targeting HIF-1 for cancer therapy. Nat Rev Cancer 2003; 3: 721–732.
View article Google Scholar - Hatch MD. A simple spectrophotometric assay for fumarate hydratase in crude tissue extracts. Anal Biochem 1978; 85: 271–275.
View article Google Scholar - Pithukpakorn M, Wei MH, Toure O, Steinbach PJ, Glenn GM, Zbar B, et al. Fumarate hydratase enzyme activity in lymphoblastoid cells and fibroblasts of individuals in families with hereditary leiomyomatosis and renal cell cancer. J Med Genet 2006; 43: 755–762.
View article Google Scholar - Ahvenainen T, Lehtonen HJ, Lehtonen R, Vahteristo P, Aittomaki K, Baynam G, et al. Mutation screening of fumarate hydratase by multiplex ligation-dependent probe amplification: detection of exonic deletion in a patient with leiomyomatosis and renal cell cancer. Cancer Genet Cytogenet 2008; 183: 83–88.
View article Google Scholar - Malik K, Patel P, Chen J, Khachemoune A. Leiomyoma cutis: a focused review on presentation, management, and association with malignancy. Am J Clin Dermatol 2015; 16: 35–46.
View article Google Scholar - Ramesh P, Annapureddy SR, Khan F, Sutaria PD. Angioleiomyoma: a clinical, pathological and radiological review. Int J Clin Pract 2004; 58: 587–591.
View article Google Scholar - Hammer P, White K, Mengden S, Korcheva V, Raess PW. Nipple leiomyoma: a rare neoplasm with a broad spectrum of histologic appearances. J Cutan Pathol 2019; 46: 343–346.
View article Google Scholar - Wang C, Tetzlaff M, Hick R, Duvic M. Reed syndrome presenting with leiomyosarcoma. JAAD Case Rep 2015; 1: 150–152.
View article Google Scholar - Weiler L, Poulalhon N, Slama A, Guillaud-Bataille M, Thomas L. Isolated cutaneous leiomyosarcoma revealing a novel germline mutation of the fumarate hydratase gene. Br J Dermatol 2016; 175: 1104–1106.
View article Google Scholar - Ylisaukko-oja SK, Kiuru M, Lehtonen HJ, Lehtonen R, Pukkala E, Arola J, et al. Analysis of fumarate hydratase mutations in a population-based series of early onset uterine leiomyosarcoma patients. Int J Cancer 2006; 119: 283–287.
View article Google Scholar - Pijpe J, Broers GH, Plaat BE, Hundeiker M, Otto F, Mastik MF, et al. The relation between histological, tumor-biological and clinical parameters in deep and superficial leiomyosarcoma and leiomyoma. Sarcoma 2002; 6: 105–110.
View article Google Scholar - Stewart L, Glenn GM, Stratton P, Goldstein AM, Merino MJ, Tucker MA, et al. Association of germline mutations in the fumarate hydratase gene and uterine fibroids in women with hereditary leiomyomatosis and renal cell cancer. Arch Dermatol 2008; 144: 1584–1592.
View article Google Scholar - Fernandez H, Chabbert Buffet N, Allouche S. Prévalence du fibrome utérin en France et impact sur la qualité de vie à partir d’une enquête menée auprès de 2500 femmes de 30–55 ans. J Gynecol Obstet Biol Reprod (Paris) 2014; 43: 721–727.
View article Google Scholar - Chen YB, Brannon AR, Toubaji A, Dudas ME, Won HH, Al-Ahmadie HA, et al. Hereditary leiomyomatosis and renal cell carcinoma syndrome-associated renal cancer: recognition of the syndrome by pathologic features and the utility of detecting aberrant succination by immunohistochemistry. Am J Surg Pathol 2014; 38: 627–637.
View article Google Scholar - Merino MJ, Torres-Cabala C, Pinto P, Linehan WM. The morphologic spectrum of kidney tumors in hereditary leiomyomatosis and renal cell carcinoma (HLRCC) syndrome. Am J Surg Pathol 2007; 31: 1578–1585.
View article Google Scholar - Trpkov K, Hes O, Agaimy A, Bonert M, Martinek P, Magi-Galluzzi C, et al. Fumarate hydratase-deficient renal cell carcinoma is strongly correlated with fumarate hydratase mutation and hereditary leiomyomatosis and renal cell carcinoma syndrome. Am J Surg Pathol 2016; 40: 865–875.
View article Google Scholar - Moch H, Cubilla AL, Humphrey PA, Reuter VE, Ulbright TM. The 2016 WHO classification of tumours of the urinary system and male genital organs – part a: renal, penile, and testicular tumours. Eur Urol 2016; 70: 93–105.
View article Google Scholar - Skala SL, Dhanasekaran SM, Mehra R. Hereditary leiomyomatosis and renal cell carcinoma syndrome (hlrcc): a contemporary review and practical discussion of the differential diagnosis for HLRCC-associated renal cell carcinoma. Arch Pathol Lab Med 2018; 142: 1202–1215.
View article Google Scholar - Grubb RL, 3rd, Franks ME, Toro J, Middelton L, Choyke L, Fowler S, et al. Hereditary leiomyomatosis and renal cell cancer: a syndrome associated with an aggressive form of inherited renal cancer. J Urol 2007; 177: 2074–2079; discussion 9–80.
View article Google Scholar - Noguchi G, Furuya M, Okubo Y, Nagashima Y, Kato I, Matsumoto K, et al. Hereditary leiomyomatosis and renal cell cancer without cutaneous manifestations in two Japanese siblings. Int J Urol 2018; 25: 832–835.
View article Google Scholar - Alrashdi I, Levine S, Paterson J, Saxena R, Patel SR, Depani S, et al. Hereditary leiomyomatosis and renal cell carcinoma: very early diagnosis of renal cancer in a paediatric patient. Fam Cancer 2010; 9: 239–243.
View article Google Scholar - Menko FH, Maher ER, Schmidt LS, Middelton LA, Aittomaki K, Tomlinson I, et al. Hereditary leiomyomatosis and renal cell cancer (HLRCC): renal cancer risk, surveillance and treatment. Fam Cancer 2014; 13: 637–644.
View article Google Scholar - Doehn C, Grunwald V, Steiner T, Follmann M, Rexer H, Krege S. The diagnosis, treatment, and follow-up of renal cell carcinoma. Dtsch Arztebl Int 2016; 113: 590–596.
View article Google Scholar - Karakiewicz PI, Jeldres C, Suardi N, Hutterer GC, Perrotte P, Capitanio U, et al. Age at diagnosis is a determinant factor of renal cell carcinoma-specific survival in patients treated with nephrectomy. Can Urol Assoc J 2008; 2: 610–617.
View article Google Scholar - Schmidt LS, Linehan WM. Hereditary leiomyomatosis and renal cell carcinoma. Int J Nephrol Renovasc Dis 2014; 7: 253–260.
View article Google Scholar - Park I, Shim YS, Go H, Hong BS, Lee JL. Long-term response of metastatic hereditary leiomyomatosis and renal cell carcinoma syndrome associated renal cell carcinoma to bevacizumab plus erlotinib after temsirolimus and axitinib treatment failures. BMC Urol 2019; 19: 51.
View article Google Scholar - Choi Y, Keam B, Kim M, Yoon S, Kim D, Choi JG, et al. Bevacizumab plus erlotinib combination therapy for advanced hereditary leiomyomatosis and renal cell carcinoma-associated renal cell carcinoma: a multicenter retrospective analysis in Korean patients. Cancer Res Treat 2019; 51: 1549–1556.
View article Google Scholar - Linehan WM, Rouault TA. Molecular pathways: Fumarate hydratase-deficient kidney cancer – targeting the Warburg effect in cancer. Clin Cancer Res 2013; 19: 3345–3352.
View article Google Scholar - Yamasaki T, Tran TA, Oz OK, Raj GV, Schwarz RE, Deberardinis RJ, et al. Exploring a glycolytic inhibitor for the treatment of an FH-deficient type-2 papillary RCC. Nat Rev Urol 2011; 8: 165–171.
View article Google Scholar - Martinek P, Grossmann P, Hes O, Bouda J, Eret V, Frizzell N, et al. Genetic testing of leiomyoma tissue in women younger than 30 years old might provide an effective screening approach for the hereditary leiomyomatosis and renal cell cancer syndrome (HLRCC). Virchows Arch 2015; 467: 185–191.
View article Google Scholar - Tolvanen J, Uimari O, Ryynanen M, Aaltonen LA, Vahteristo P. Strong family history of uterine leiomyomatosis warrants fumarate hydratase mutation screening. Hum Reprod 2012; 27: 1865–1869.
View article Google Scholar - Harrison WJ, Andrici J, Maclean F, Madadi-Ghahan R, Farzin M, Sioson L, et al. Fumarate hydratase-deficient uterine leiomyomas occur in both the syndromic and sporadic settings. Am J Surg Pathol 2016; 40: 599–607.
View article Google Scholar - Lehtonen R, Kiuru M, Vanharanta S, Sjoberg J, Aaltonen LM, Aittomaki K, et al. Biallelic inactivation of fumarate hydratase (FH) occurs in nonsyndromic uterine leiomyomas but is rare in other tumors. Am J Pathol 2004; 164: 17–22.
View article Google Scholar - Andrici J, Gill AJ, Hornick JL. Next generation immunohistochemistry: emerging substitutes to genetic testing? Semin Diagn Pathol 2018; 35: 161–169.
View article Google Scholar - Rabban JT, Chan E, Mak J, Zaloudek C, Garg K. Prospective detection of germline mutation of fumarate hydratase in women with uterine smooth muscle tumors using pathology-based screening to trigger genetic counseling for hereditary leiomyomatosis renal cell carcinoma syndrome: a 5-year single institutional experience. Am J Surg Pathol 2019; 43: 639–655.
View article Google Scholar - Bardella C, El-Bahrawy M, Frizzell N, Adam J, Ternette N, Hatipoglu E, et al. Aberrant succination of proteins in fumarate hydratase-deficient mice and HLRCC patients is a robust biomarker of mutation status. J Pathol 2011; 225: 4–11.
View article Google Scholar - Carter CS, Skala SL, Chinnaiyan AM, McHugh JB, Siddiqui J, Cao X, et al. Immunohistochemical characterization of fumarate hydratase (fh) and succinate dehydrogenase (sdh) in cutaneous leiomyomas for detection of familial cancer syndromes. Am J Surg Pathol 2017; 41: 801–809.
View article Google Scholar - Llamas-Velasco M, Requena L, Adam J, Frizzell N, Hartmann A, Mentzel T. Loss of fumarate hydratase and aberrant protein succination detected with S-(2-Succino)-cysteine staining to identify patients with multiple cutaneous and uterine leiomyomatosis and hereditary leiomyomatosis and renal cell cancer syndrome. Am J Dermatopathol 2016; 38: 887–891.
View article Google Scholar - Chan E, Rabban JT, Mak J, Zaloudek C, Garg K. detailed morphologic and immunohistochemical characterization of myomectomy and hysterectomy specimens from women with hereditary leiomyomatosis and renal cell carcinoma syndrome (HLRCC). Am J Surg Pathol 2019; 43: 1170–1179.
View article Google Scholar - Buelow B, Cohen J, Nagymanyoki Z, Frizzell N, Joseph NM, McCalmont T, et al. Immunohistochemistry for 2-succinocysteine (2SC) and fumarate hydratase (FH) in cutaneous leiomyomas may aid in identification of patients with HLRCC (hereditary leiomyomatosis and renal cell carcinoma syndrome). Am J Surg Pathol 2016; 40: 982–988.
View article Google Scholar - Llamas-Velasco M, Requena L, Kutzner H, Scharer L, Rutten A, Hantschke M, et al. Fumarate hydratase immunohistochemical staining may help to identify patients with multiple cutaneous and uterine leiomyomatosis (MCUL) and hereditary leiomyomatosis and renal cell cancer (HLRCC) syndrome. J Cutan Pathol 2014; 41: 859-865.
View article Google Scholar - Harvey NT, Wood BA. Is immunohistochemical screening of cutaneous leiomyomas for the early detection of hereditary leiomyomatosis and renal cell carcinoma syndrome justified? Am J Dermatopathol 2018; 40: 939–940.
View article Google Scholar - Stewart L, Glenn G, Toro JR. Cutaneous leiomyomas: a clinical marker of risk for hereditary leiomyomatosis and renal cell cancer. Dermatol Nurs 2006; 18: 335–341; quiz 42.
View article Google Scholar - Cohen PR, Erickson CP, Calame A. Painful tumors of the skin: “CALM HOG FLED PEN AND GETS BACK”. Clin Cosmet Investig Dermatol 2019; 12: 123–132.
View article Google Scholar - Bin Saif GA, Buraik MA, Pokharel A, Sangueza OP. Recurrent reactive angioendotheliomatosis in pregnancy: a case report. Int J Dermatol 2015; 54: e480–e482.
View article Google Scholar - Lima LAF, Lisboa GM, Silva Filho EAD, Rabelo G. Multiple dermatomyofibromas. An Bras Dermatol 2018; 93: 268–270.
View article Google Scholar - Drayer SM, Catherino WH. Prevalence, morbidity, and current medical management of uterine leiomyomas. Int J Gynaecol Obstet 2015; 131: 117–122.
View article Google Scholar - Moch H, Ohashi R, Gandhi JS, Amin MB. Morphological clues to the appropriate recognition of hereditary renal neoplasms. Semin Diagn Pathol 2018; 35: 184–192.
View article Google Scholar - Haas NB, Nathanson KL. Hereditary kidney cancer syndromes. Adv Chronic Kidney Dis 2014; 21: 81–90.
View article Google Scholar - Jensen DK, Villumsen A, Skytte AB, Madsen MG, Sommerlund M, Bendstrup E. Birt-Hogg-Dube syndrome: a case report and a review of the literature. Eur Clin Respir J 2017; 4: 1292378.
View article Google Scholar - Refae MA, Wong N, Patenaude F, Begin LR, Foulkes WD. Hereditary leiomyomatosis and renal cell cancer: an unusual and aggressive form of hereditary renal carcinoma. Nat Clin Pract Oncol 2007; 4: 256–261.
View article Google Scholar - van Spaendonck-Zwarts KY, Badeloe S, Oosting SF, Hovenga S, Semmelink HJ, van Moorselaar RJ, et al. Hereditary leiomyomatosis and renal cell cancer presenting as metastatic kidney cancer at 18 years of age: implications for surveillance. Fam Cancer 2012; 11: 123–129.
View article Google Scholar - Schmidt LS, Linehan WM. clinical features, genetics and potential therapeutic approaches for Birt-Hogg-Dube syndrome. Expert Opin Orphan Drugs 2015; 3: 15–29.
View article Google Scholar