Table I. Demographic, clinical, laboratory and ultrasound findings in patients with hidradenitis suppurativa (HS) and healthy controls
Departments of 1Dermatology, 2Radiology and 4Internal Medicine Alicante, University General Hospital, Alicante Institute for Health and Biomedical Research (ISABIAL-FISABIO Foundation), Alicante, Spain, and 3Department of Dermatology, Zealand University Hospital Roskilde, Health Sciences Faculty, University of Copenhagen, Denmark
#These authors contributed equally.
Non-alcoholic fatty liver disease (NAFLD) is currently the most common cause of end-stage liver disease. The aim of this controlled cross-sectional study was to assess the association between NAFLD and hidradenitis suppurativa. NAFLD was assessed using hepatic ultrasound. A total of 125 patients with hidradenitis suppurativa and 120 patients without hidradenitis suppurativa were recruited, matched for age, sex and body mass index (< 25 or ≥ 25 kg/m2), a risk factor related to NAFLD. Both groups presented similar proportions of overweight or obesity (89.6% vs 90%). Patients with hidradenitis suppurativa presented significantly higher prevalence of NAFLD compared with those with non-hidradenitis suppurativa (57.6% vs 31.7%, p < 0.001). Multivariable analysis confirmed independent association between hidradenitis suppurativa and NAFLD (odds ratio 2.79, 95% confidence interval 1.48–5.25; p = 0.001) besides age, body mass index, hypertension and hypertransaminasaemia. Hidradenitis suppurativa is significantly associated with the development of NALFD regardless of the presence of classic metabolic risk factors.
Key words: non-alcoholic fatty liver disease; hidradenitis suppurativa; acne inversa; liver steatosis; hepatic ultrasound.
Accepted Jul 7, 2020; Epub ahead of print Jul 29, 2020
Acta Derm Venereol 2020; 100: adv00239.
Corr: Iris González Villanueva, Department of Dermatology, University General Hospital, Alicante Institute for Health and Biomedical Research (ISABIAL-FISABIO Foundation), C/ Maestro Alonso s/n., ES-03010 Alicante, Spain. E-mail: jolairis@gmail.com
Non-alcoholic fatty liver disease has been linked with chronic inflammatory conditions, such as psoriasis. Hidradenitis suppurativa shares key pathogenic features and comorbidities with psoriasis, and this study shows that it is also an independent risk factor for non-alcoholic fatty liver disease. Clinicians should consider routine work-up for non-alcoholic fatty liver disease in patients with hidradenitis suppurativa.
Hidradenitis suppurativa (HS) is a chronic, recurrent inflammatory disease affecting intertriginous areas. It is characterized by painful nodules that progress to abscesses, tunnels and scarring (1), which most commonly appear in the axillary, inguinal, perianal, gluteal and submammary regions (2). The estimated prevalence of HS is approximately 1–4%, and a recent systematic review and meta-analysis found a significant association between HS and obesity, central obesity, active smoking, hypertriglyceridaemia, low levels of high-density lipoprotein (HDL) cholesterol, diabetes and metabolic syndrome (3–8). Similarly, a recent case-control study reported a higher prevalence of insulin resistance in people with HS (9).
For its part, non-alcoholic fatty liver disease (NAFLD) is defined by the presence of steatosis in more than 5% of hepatocytes, with little or no alcohol consumption (10). NAFLD includes a spectrum of conditions, ranging from steatosis, with a predominantly benign evolution, to more severe forms of non-alcoholic steatohepatitis (NASH), which may eventually lead to fibrosis, cirrhosis and hepatocellular carcinoma (11). Indeed, as many as 30–50% of patients with NAFLD may be diagnosed with cirrhosis within 10 years (12), and NAFLD represents the main cause of chronic liver disease in Europe and North America (17–30% of the population). Worldwide, the prevalence of cirrhosis is 2–4%, constituting a serious public health concern (13). Several theories about the aetiopathogenic mechanisms leading to NAFLD have been proposed. As with type 2 diabetes, insulin resistance seems to play a pivotal role in NAFLD (14, 15). Yet, even though NAFLD is more prevalent in obese and diabetic patients, its incidence is not limited to this population (16).
In terms of diagnosing and classifying NAFLD, liver biopsy is currently the gold standard (17). However, in clinical practice, hepatic ultrasound is usually preferred as a non-invasive alternative, incurring lower costs and negligible risk to the patient. Ultrasound has good sensitivity (92.7–100%) and specificity (91–92.5%) for diagnosing hepatic steatosis of 5% or more (18, 19). The severity of hepatic steatosis is classified into 3 levels: mild, moderate, and severe (20, 21).
Over the last decade, evidence has been accumulating of an association between NAFLD and psoriasis: another systemic cutaneous chronic inflammatory disease (22–26). HS and psoriasis also share commonalities in terms of aetiopathogenesis, systemic inflammation and comorbidities, frequently coinciding in the same patient (27). The interleukin 23/T helper 17 pathway has been implicated in the pathogenesis of both psoriasis and HS, and is thought to be the molecular key feature underlying pathomechanistic overlap. However, patients with HS seem to sustain a greater inflammatory load and have a higher overall burden of comorbidities than those with psoriasis (28, 29), including with regard to cardiovascular risk factors, such as central obesity, type 2 diabetes, insulin resistance, dyslipidaemia and hypertension (8). In turn, these conditions increase the risk of developing NAFLD (30).
Two recent studies have begun to articulate an association between HS and NAFLD. The first, a retrospective analysis of a multi-centre investigation, detected NAFLD in 37.2% of a sub-cohort of 84 patients with HS. How-ever, this was a small sized sub-analysis from another study and it was not designed specifically to detect this correlation (31). The second was a single-centre case control study in 70 patients with HS plus 150 age- and sex-matched (but not body mass index (BMI)-matched) controls; Durán-Vian and colleagues, observed a significantly higher prevalence of NAFLD in patients with HS (72.9% vs 24.7%: p < 0.001), and in multivariable regression analysis, this association was independent of age, sex, and classic metabolic risk factors for NAFLD (OR 7.75, confidence interval (CI) 2.54–23.64, p < 0.001). Nonetheless, their groups showed high heterogeneity in BMI, which explains the high heterogeneity in hypertension, dyslipidaemia and metabolic syndrome. This fact could explain the magnitude of the correlation these authors found, which may be overestimated (32).
The objective of the current study was to assess the association between HS and NAFLD.
Patients and study design
This was a transversal, cross-sectional study, assessing NAFLD by hepatic ultrasound. Patients aged 35–64 years with moderate to severe HS (Hurley stage II or III exclusively) and with at least 5 years of disease duration, were consecutively recruited from our HS clinic from January 2018 to December 2018. A qualified dermatologist (JCP) diagnosed patients with HS based on clinical examination and diagnostic criteria, including a history of recurrent inflammatory nodules, abscesses, and draining sinuses on inverted areas (33). HS-related variables included age at onset of HS, duration of the disease, severity of the disease as assessed by the Hurley classification, Sartorius score (34), and International Hidradenitis Suppurativa Severity Score System (IHS4) (35), association with pilonidal cyst, number of involved areas, Dermatology Life Quality Index (DLQI), pain and pruritus (assessed by visual analogue scale from 0–10, with 0 representing no pain or pruritus, and 10 being the worst pain or pruritus they could imagine). A control population was selected from the healthy companions of patients who came to dermatology consultations, and patients with HS were matched for age (± 5 years), sex and categorized BMI (normal BMI < 25 kg/m2 vs overweight/obese ≥ 25 kg/m2), in acknowledgement that age and overweight/obesity are well-known factors associated with NAFLD (30).
Exclusion criteria were the presence of hepatitis B surface antigens, hepatitis C virus antibody seropositivity, autoimmune hepatitis, or drug-induced liver disease; frequent alcohol intake, defined as more than 2 standard drinks per day (in Europe: 341 ml bottle of 5% alcohol beer, cider or cooler; 43 ml shot of hard liquor; or 142 ml glass of 12% wine (36)) in women or more than 3 standard drinks per day in men; and any other chronic inflammatory conditions, such as psoriasis, systemic lupus erythematosus or inflammatory bowel disease. The institutional review board of the University Hospital Alicante reviewed and approved the study protocol (2018/62), and all participants provided written informed consent.
Demographic and clinical (classic cardiovascular risk factors) data were recorded for all patients. Metabolic syndrome was defined using the National Cholesterol Education Program Adult Criteria Treatment Panel III Criteria (37). A complete blood count and blood differential were undertaken to determine biochemical parameters, including glycaemia, sodium, potassium, total cholesterol, high- and low-density lipoprotein cholesterol, triglycerides, alanine aminotransferase (ALT), ?-glutamyl transferase (GGT), aspartate aminotransferase (AST), albumin, insulin, glycated haemoglobin, and the high-sensitivity C-reactive protein (hs-CRP) inflammatory biomarker, among others.
Assessment of non-alcoholic fatty liver disease
Two board-certified radiologists, blinded to participants’ details, performed hepatic ultrasound in all participants, using a Toshiba Aplio 300 ultrasound scanner with a 6-MHz Convex abdominal probe (Canon Medical Systems S.A. Spain). Diagnosis of hepatic steatosis was based on characteristic ultrasonographic features (18, 21), and NAFLD was classified as mild, moderate, or severe (20).
Statistical analysis
Descriptive statistics were used to summarize the data. Categorical variables were compared between patients with HS and controls (presence of NAFLD and explanatory variables including age, sex, and metabolic syndrome) using the χ2 test of homogeneity. Crude odds ratio (ORs) and 95% confidence intervals (95% CIs) were calculated to estimate the magnitude of associations between explanatory variables and NAFLD. All variables yielding a p-value of < 0.25, or having a plausible theoretical association with the outcome, were included in a saturated, multivariable logistic regression model. Successive models were then fitted using backward elimination, deleting the variables with the lowest contribution to the model and without any confounding effect. Analyses were adjusted for traditional risk factors, age, and sex. All analyses were performed using STATA software (version 12, Stata Corporation, College Station, TX, USA).
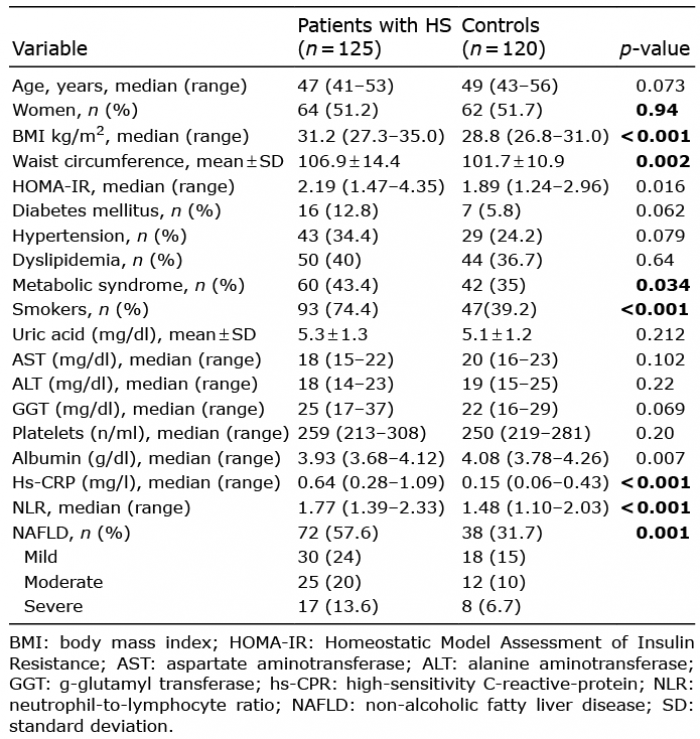
In total, 125 patients with HS and 120 controls were recruited. Their baseline characteristics are shown in Table I. Participants’ mean age was 48 years, and 51.42% were women. As patients from both groups were matched on the basis of categorized BMI (normal vs obese), similar proportions of patients with HS and controls were classified as overweight or obese (HS patients: 112, 89.6% vs controls: 108, 90.0%), but median BMI was higher in patients with HS (31.2 kg/m2 vs 28.8 kg/m2, p < 0.001). The Homeostatic Model Assessment of Insulin Resistance (HOMA-IR) values in patients with HS were also higher than in the control group (median 2.19 vs 1.89, p = 0.016), as were inflammation markers, such as the neutrophil-to-lymphocyte ratio (NLR) and hs-CRP. Likewise, traditional cardiovascular risk factors, such as diabetes, hypertension, and smoking, were more prevalent in the HS patients group; for example, metabolic syndrome was detected in 60 (43.4%) patients with HS, compared with 42 (35%) controls (p = 0.034).
Table I. Demographic, clinical, laboratory and ultrasound findings in patients with hidradenitis suppurativa (HS) and healthy controls
Hepatic ultrasound indicated NAFLD in 72 (57.6%) patients with HS vs 38 (31.7%) controls (p < 0.001). Of these 72 patients, NAFLD severity was classified as mild in 30 (41.6%) patients, moderate in 25 (34.7%), severe in 17 (23.6%). Table II presents the clinical findings related to HS. Median age of onset was 25 years, and median duration of disease was 24 years. Of the 125 patients with HS, 97 (77.6%) were classified as Hurley stage II and 28 (22.4%) as Hurley III. The median number of affected sites was 3; the axilla and groin were the most commonly involved locations.

Table II. Clinical findings in patients with hidradenitis suppurativa
Table III shows the results of the bivariable and multivariable analyses. Crude analyses suggested that HS was a risk factor for NAFLD (OR 2.93, 95% CI 1.74–4.95, p < 0.001), along with age, BMI, waist circumference and cardiovascular risk factors, such as hypertension, dyslipidaemia, diabetes, insulin resistance and metabolic syndrome. Blood biomarkers associated with NAFLD in bivariable analyses were hs-CRP, AST, ALT, and GGT. Multivariable logistic regression analysis confirmed that HS significantly increases the risk of developing NAFLD (adjusted OR 2.79, 95% CI 1.48–5.25, p = 0.001), even after adjusting for the independent effects of age (adjusted OR 1.05, 95% CI, p = 0.012), BMI (adjusted OR 1.17, 95% CI, p < 0.001), ALT levels (adjusted OR 1.04, 95% CI, p = 0.016), and hypertension (adjusted OR 2.83, 95% CI 1.42–5.64, p = 0.003). The current study also attempted to define specific HS-related variables associated with NAFLD. However, so significant association was observed with disease-related variables, such as duration of HS, severity, number of affected sites, or symptoms.
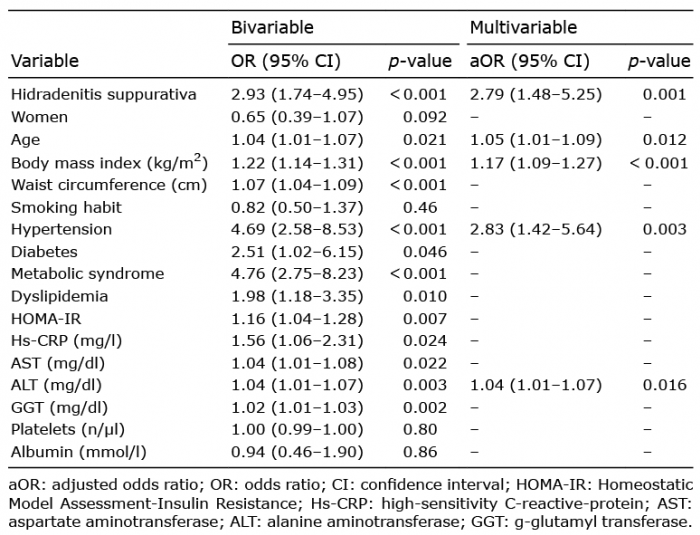
Table III. Odds of developing non-alcoholic fatty liver disease, according to explanatory variables (bivariable and multivariable analysis)
These results provide new evidence that NAFLD is highly likely to develop in patients with HS. Risk on healthy population of developing this disease is increased in patients with HS nearly three-fold, even after adjusting for age, BMI, ALT levels, and hypertension. NAFLD was diagnosed in 57.6% of patients with HS vs 31.7% non-HS patients.
In the general population, worldwide, NAFLD affects 30–40% of men and 15–20% of women (38). Prevalence of NAFLD increases with age as well as with overweight/obesity, with several observational studies showing that patients with a BMI of 30 kg/m2 or more presented a significantly higher prevalence than those under this threshold (33.64% vs 12.13%, p < 0.001). The same applies to populations with metabolic risk factors, such as diabetes mellitus or hypertension (39). The current controlled cross-sectional study, matched study groups for age, sex, and BMI categories, in order to minimize the impact of confounders that are independently associated with NAFLD (40).
Currently, NAFLD is considered a multisystemic disease, given the numerous comorbidities associated with it (41). However, NAFLD is also associated with diseases that have a high systemic inflammatory burden, such as psoriasis. In a meta-analysis including 7 case-control studies, Candia et al. (24) concluded that NAFLD is twice as prevalent in people with psoriasis as in those without (OR 2.07, 95% CI 1.62–2.64). Moreover, cohorts with psoriatic arthritis or more severe or long-lasting psoriasis have also been shown to carry a higher risk for NAFLD.
Although the physiopathology of NAFLD has not been completely elucidated, the multiple hit model posits it as a complex, multistep liver injury. An excess of pro-inflammatory cytokines circulating in patients with psoriasis or HS can trigger insulin resistance, which in turn leads to an accumulation of triglycerides in the hepatocytes. As a result of this steatotic state, the liver becomes susceptible to inflammatory damage. Hepatic steatosis can also accelerate the production of pro-inflammatory adipocytokines, and with it a systemic inflammatory process that entails greater insulin resistance. Imbalances are gradually produced between the production and elimination of triglycerides (which sets the stage for the transition from steatosis to steatohepatitis) and between hepatocyte death and hepatic regeneration. The presence of HS or psoriasis might intensify this entire process because of the accompanying state of chronic and systemic inflammation and the alteration in the tumour necrosis factor alpha (TNF-α)/adiponectin relationship, which promotes progression to liver disease (40).
The crucial role of the permanent inflammatory burden in the aetiopathogenesis of NAFLD could explain why HS is associated with NAFLD. The association between these 2 diseases described by Durán-Vilan et al. (33) is noteworthy for its magnitude (OR 7.75, 95% CI 2.54–23.64; p < 0.001), but it could be partly attributable to the fact that they did not match cases and controls for BMI, an important confounder given the frequency of obesity in patients with HS and its role as a risk factor for NAFLD. Durán-Vilan et al.’s study described considerable and statistically significant differences between groups on this parameter (cases: 30.4 SD 6.2 kg/m2 vs controls: 26.1 SD 4.7 kg/m2; p < 0.001). Thus, we consider that the relative risk derived from our data (adjusted OR 2.79, 95% CI 1.48–5.25, p = 0.001) is probably more accurate, as we minimized the risk of confounding due to categorized BMI thorough matching.
An intrinsic limitation of the cross-sectional study design is that the temporal relationship remains unclear, and a direct causal relationship between HS and NAFLD cannot be established. Because the population consisted of participants aged 35–64 years, results may not be generalizable to younger or more elderly populations. However, NAFLD mainly affects middle-aged people, and its prevalence increases with age. Furthermore, in our study there is residual confusion: in addition to the unknown confounders, since the comparison has been made on the basis of the BMI categories, differences still remain between the 2 groups in terms of BMI. We also consider that the size of the groups might be too small to detect some meaningful differences.
In conclusion, the current study found a high prevalence of NAFLD in patients with HS, regardless of the presence of other classic metabolic known risk factors. Moreover, we hypothesize that the association between HS and NAFLD may not be related to severity of HS, because no significant association with any of the disease-related variables was found. The results of this study provide additional evidence about the association between HS and NAFLD, with potentially relevant clinical implications. Physicians involved in the care of patients with HS should be aware of the links between these conditions. An active approach to the diagnosis and management of this co-morbidity seems reasonable.
This study has received a grant from the Institute for Health and Biomedical Research (ISABIAL-FISABIO Foundation).
GJ has been an investigator, consultant, and advisory board member for Abbvie and Novartis and has received unrestricted grants from Abbvie, Leo Pharma, and Novartis. In addition, he has been a speaker and investigator for Leo Pharma; a speaker for Galderma; an investigator for Regeneron; and an advisory board member for Janssen-Cilag, Inflarx, MSD, and Pierre-FAbre. JCP has been an advisory board member for Abbvie. IG-V, CDG, MP, IP, PA, LS-P, IB and JMR have no conflicts of interest to declare.