ORIGINAL REPORT
A Qualitative Tool to Guide in the Interpretation of the Numerical Rating Scale for Pruritus Intensity in Patients with Atopic Dermatitis
Ignasi FIGUERAS1, Marta FEITO2, Marta GARCÍA-BUSTINDUY3, Emilio MONTE-BOQUET4, Sandra ROS5, Violeta ZARAGOZA6, África LUCA DE TENA7 and Francisco Javier ORTIZ DE FRUTOS8
1University Hospital of Bellvitge, Hospitalet de Llobregat, Barcelona, 2Department of Pediatric Dermatology, La Paz University Hospital-UAM, Madrid, 3Department of Dermatology, University Hospital of Canarias, University of La Laguna, Tenerife, Canary Islands, 4Pharmacy Service, La Fe University Hospital, Valencia, 5Department of Dermatology, Hospital of Santa Creu and Sant Pau, Autonomous University of Barcelona, Barcelona, 6Department of Dermatology, University General Hospital of Valencia, Valencia, 7Association of People Affected by Atopic Dermatitis, Spain, and 8Department of Dermatology, 12 de Octubre University Hospital, Complutense University of Madrid, Madrid, Spain
Atopic dermatitis is a cutaneous inflammatory disease characterized by intense pruritus, which is often underestimated despite its direct impact on patients’ health-related quality of life and the high burden it poses. The authors’ goal was to design a qualitative tool to guide patients and healthcare professionals in their assessment and interpretation of pruritus intensity using a numerical rating scale. The draft of this tool, henceforth “guideline”, was developed based on a systematic literature review and focus groups comprising patients and a scientific committee. This draft was validated with an independent group of patients and the final version was designed following their feedback. According to the results of the systematic review, pruritus impacts 6 health-related quality of life domains: sleep quality; emotional status; overall health-related quality of life; physical function; social/sexual activity; productivity, particularly affecting sleep quality and the emotional domain. Patients considered that physical function was the most strongly affected domain, followed by sleep quality and emotional well-being, establishing that a minimum pruritus intensity of 4 and 7 points impacts moderately and severely, respectively, on the different domains of patients’ health-related quality of life. The guideline may help patients and healthcare professionals to interpret and assess pruritus intensity using a numerical rating scale and to understand the impact of pruritus on patients’ health-related quality of life.
Key words: atopic dermatitis; atopic eczema; pruritus; quality of life; rating scale.
SIGNIFICANCE
Atopic dermatitis is a skin disease characterized by intense itching. Atopic dermatitis impacts on different domains of patients’ quality of life but is often underestimated. Pruritus intensity evaluation using numerical scales is subjective and can be difficult to interpret for both clinicians and patients. In this context, a tool or “guideline” has been developed to assist healthcare professionals and patients to assess itch intensity using a numerical rating scale and to understand the impact of itching on patients’ quality of life.
Citation: Acta Derm Venereol 2024; 104: adv18255. DOI https://doi.org/10.2340/actadv.v104.18255.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Submitted: Jul 17, 2023; Accepted: Feb 26, 2024; Published: Apr 2, 2024
Corr: Francisco Javier Ortiz de Frutos, Department of Dermatology, 12 de Octubre University Hospital, Complutense University of Madrid, C/ Dr. Tolosa Latour, s/n., ES-28041, Madrid, Spain. E-mail: javierortiz@aedv.es
Competing interests and funding: IF and EMB have received honoraria from Abbvie to undertake the present study. MGB has received honoraria from Almirall, Abbvie, Cellgene, Galderma, Janssen, LEO Pharma, Lilly, Novartis, Pfizer, Sanofi, and UCB. MF, SR, VZ, AFT, and FJOF declare that they have no conflicts of interest.
INTRODUCTION
Atopic dermatitis (AD) is a common, chronic, and recurrent cutaneous inflammatory disease characterized by intense pruritus, pain, and dry skin (1, 2). AD onset usually occurs in childhood, affecting up to 20% of children worldwide (3, 4) and can persist in up to 10% of adults (5,6).
The main symptoms of AD can interfere with patients’ activities, negatively impacting their health-related quality of life (HRQoL) (7, 8). In this regard, pruritus is one of the main drivers of impaired HRQoL in patients with AD (7, 9). In fact, it has been reported that approximately 86% of patients with AD experience itching every day of the week and 63% during at least 12 h a day (7). In addition, pruritus is often intense, and approximately 60% of patients consider it severe or unbearable (7). Consequently, pruritus impacts different HRQoL domains, deteriorating patients’ sleep quality (10) and increasing anxiety and depression among patients with AD (11). Thus, pruritus is one of the main symptoms affecting patients with AD (2); however, it is often underestimated due to its subjective nature (2).
To date, pruritus severity assessment is usually based on patient reports and is measured using intensity scales such as the visual analogue scale, the verbal rating scale, and the numerical rating scale (NRS) (12, 13). The NRS has proven to be a good measure in evaluating pruritus intensity in patients with AD, providing a reliable and accurate assessment of pruritus (14). However, these tools provide patients’ vision of the disease, which, although invaluable, is entirely subjective (13–15). In addition, these tools can be difficult to interpret clinically for both healthcare professionals (HCPs) and patients (15).
Considering the above, we aimed to develop a qualitative tool, henceforth referred to as a “guideline”, to facilitate use and interpretation of the NRS for pruritus intensity by HCPs and patients with AD.
MATERIALS AND METHODS
Project design
The project consisted of five phases: (i) a systematic literature review, (ii) first focus group with the scientific committee (SC), (iii) focus group with patients, (iv) second focus group with the SC, and (v) semi-structured interviews with patients.
Patients’ participation was anonymous, complying with data protection regulations. Patients received the patient information sheet and agreed to participate in focus groups and interviews. No informed consent was required. Given that the project did not use patients’ clinical data, evaluation by a Review Board or Ethics Committee was not required.
Systematic literature review
A systematic literature review was performed in international and Spanish databases (PubMed/Medline, Scopus, MEDES, and IBECS), and in the grey literature (Google Scholar, ProQolid, BiblioPro) during August 2022 in order to identify specific HRQoL domains negatively impacted by pruritus in patients with AD and pruritus evaluation tools. The search was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) recommendations (16) and Cochrane guidelines (17), using search filters and standardized terms (Tables SI and SII). Systematic reviews, meta-analyses, expert consensus, and observational studies published in English or Spanish between 25 August 2017 and 25 August 2022 were reviewed. Clinical trials, opinion articles, letters to the editor, and congress communications were excluded.
Two independent researchers selected the studies and extracted the data. Discrepancies were resolved by consensus or by involving a third researcher.
The quality of the observational studies reviewed was evaluated using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) criteria (18), while the level of evidence was determined using the level of evidence scale developed by the Oxford Centre for Evidence-Based Medicine (OCEBM) (19).
First focus groups with the scientific committee
The strategy of using focus groupwork relies on the dynamic of interaction and discussion among participants to gather different points of view reflecting the participants’ opinions, beliefs, convictions, ideas or experiences (20). Focus groups generally consist of 4–12 members to ensure an adequate number for discussion without overcrowding (20).
The focus group was composed of the 7 members of the SC (IF, MF, MG-B, EM-B, SR, VZ, and FJOF), who represented different disciplines involved in the management of AD: Dermatology (n = 5), Clinical Pharmacy (n = 1), and Psychology (n = 1).
This focus group was held to identify, from a clinical perspective, relevant aspects of pruritus and its impact on HRQoL based on the results obtained in the literature review. The SC selected and prioritized the most relevant HRQoL domains affected by pruritus in AD for their inclusion in the guideline.
Focus groups with atopic dermatitis patients
Patients with AD (n = 9) were identified and invited to participate in the online focus group by the Spanish Association of People Affected by Atopic Dermatitis (Asociación de Afectados por la Dermatitis Atópica; AADA). Adolescent (13–17 years old, n = 4) and adult (≥ 18 years old, n = 5) patients with a heterogeneous sociodemographic and clinical profile were selected; patients with moderate–severe AD were prioritized to ensure the presence of different levels of pruritus intensity. The focus group’s objective was to explore pruritus impact on HRQoL domains in the day-to-day life of patients with AD.
The patient focus group dynamic was structured in two main phases. An initial phase aimed to present the HRQoL domains affected by pruritus, which had been identified in the literature review and by the first focus group with the SC. Subsequently, a debate was conducted to explore the most relevant aspects of those affected by pruritus and AD from the patients’ perspective. In the second phase, patients scored (on a scale from 0 to 10) the minimum intensity at which pruritus caused a moderate or severe impact in different domains of HRQoL.
Second focus group with the scientific committee
The final focus group with the SC aimed to define the main aspects to be considered when preparing the first draft of the guideline.
Semi-structured interviews with patients
The first draft of the guideline was assessed by an independent group of patients, who did not participate in the first focus group.
Semi-structured interviews (n = 6) were conducted to gain insight into patients’ perceptions of the guideline’s user-friendliness and level of usefulness. The information gathered in this interview was used to design the final version of the guideline. These patients were also asked to score the minimum intensity at which pruritus moderately or severely affected the different domains of HRQoL. These results were pooled with those obtained in the patient focus groups to better define the pruritus intensity thresholds.
Patients were identified and invited to participate by the AADA.
RESULTS
Literature review
The search yielded a total of 456 references. After removing duplicates and applying the inclusion and exclusion criteria, 29 publications were selected (Fig. 1). Of these, 10 publications evaluated the impact of pruritus on HRQoL (Table SIII), while the remaining 19 publications showed a total of 12 tools used to assess the impact of pruritus on HRQoL (Table SIV). The evaluation of the quality of the evidence showed that most of the reviewed studies met 60% of the essential aspects defined by STROBE and an OCEBM level of evidence of 4 (see Table SIII).
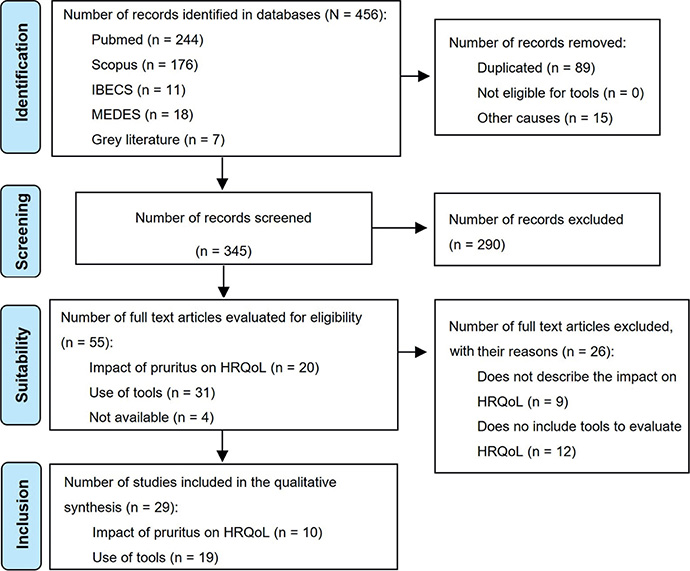
Fig. 1. PRISMA diagram showing the study selection process.
All publications (n = 10) assessing the impact of the disease included patients presenting with AD; however, only three of them (30%) focused exclusively on patients with AD. Most (80%) of the identified studies had a cross-sectional design, while 20% presented post hoc analyses in a clinical trial. Of the 12 tools identified, three (25%) were designed specifically for AD patients: Eppendorf Pruritus Questionnaire, Atopic Dermatitis Itch Scale and Severity of Pruritus Scale. The nine remaining tools targeted patients with pruritus and dermatological diseases, including AD (42%), as well as patients presenting with chronic pruritus regardless of aetiology (33%).
Six HRQoL domains were identified by these studies: sleep quality and emotional well-being were each reported by 6 studies, while physical, social and sexual activity, and productivity were each reported by 1 study. The identified tools covered the following HRQoL domains: sleep quality (75%), emotional well-being (67%), physical activity (50%), social and sexual activity (50%), and productivity (50%) (Fig. 2).
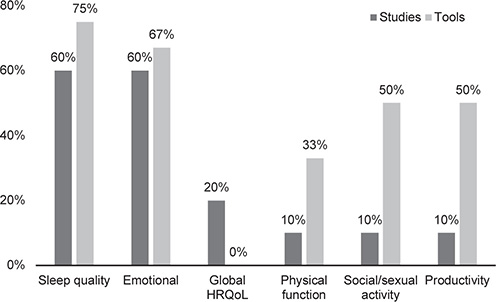
Fig. 2. Health-related quality of life (HRQoL) domains affected by pruritus and tools identified in the review. Studies: n = 10; tools: n = 12.
First focus group with the scientific committee
The SC agreed that sleep quality and the emotional domain were those most affected by pruritus in patients with AD and should, therefore, be included in the guideline. Additionally, it was considered that pruritus affects physical function and social activities due to poor sleep quality and scratching, respectively. The SC also agreed that work or academic productivity, as well as social activity and, especially, sexual activity are rarely explored in clinical practice. Therefore, they considered all these domains relevant to include in the guideline. By contrast, overall HRQoL was not included in the guideline as it was considered to be represented in all other domains.
Focus group with patients
Patients considered physical function was the HRQoL domain most affected by pruritus. They complained that, to avoid sweating and the consequent pruritus, they refrained from doing sports and outdoor, leisure or other daily activities.
Furthermore, patients highlighted that sleep quality was mainly affected by pruritus intensity, although lesion location is also a factor affecting this domain. Patients agreed that the emotional domain is affected equally by pruritus and the presence of lesions. Among the numerous feelings reported by the patients, stress and anxiety were the most common, and were directly related to itch intensity.
They also considered that pruritus affects social and sexual activity as well as work/academic productivity, although to a lesser extent.
Second focus group with the scientific committee
To develop the first draft, the SC agreed that the guideline should target patients with AD and would include information regarding the importance of pruritus assessment, barriers hindering its evaluation, and the HRQoL domains affected, as well as a pruritus rating scale and instructions for its assessment.
Additionally, the SC considered that this guideline should be composed of two differentiated sections: one targeted patients with AD and the other HCPs. The section addressed to HCPs would aim to provide a helpful reference in clinical practice, and would include the methodology followed during guideline development as well as a summary of the main results of the systematic review.
Interviews with patients
Patients evaluated pruritus intensity and impact on their HRQoL using the guideline. These results, together with those obtained in the first focus group, were used to set the intensity thresholds at which pruritus affects different domains of patients’ lives; a pruritus intensity of 4–8 points impacts moderately on HRQoL domains, while a score > 7–8 impacts severely (Fig. 3).
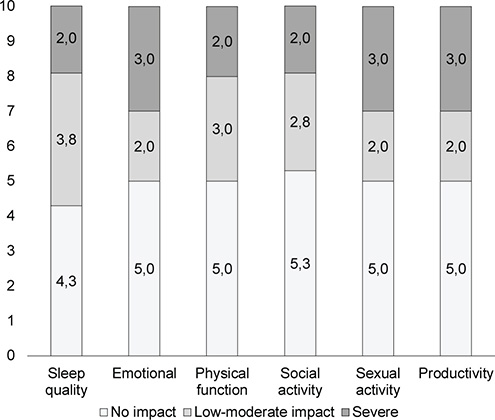
Fig. 3. Intensity of pruritus and impact on Health-related Quality of Life (HRQoL) domains according to patients from the focus and the interview groups.
Patients considered that the guideline was useful and easy to understand, providing a context that would help to score the impact of their pruritus, and that the thresholds in the guideline were in line with their own experience. However, they mentioned that some characteristics of the guideline could be improved. For example, they proposed changes in the content, vocabulary and grammar, eliminating terms such as flare and using conventional terms. Patients also suggested that it would be useful for them if the guideline first described those HRQoL domains that were most affected.
Final version of the guideline
A two-section final guideline (Appendix S1) was designed; the patients’ section is intended to objectively measure itch intensity and the HCPs’ section is intended to help them gain a better understanding of pruritus intensity in patients in clinical practice. Fig. 4 shows the section of the guide containing the itch NRS addressed to patients (Fig. 4A) and HCPs (Fig. 4B).
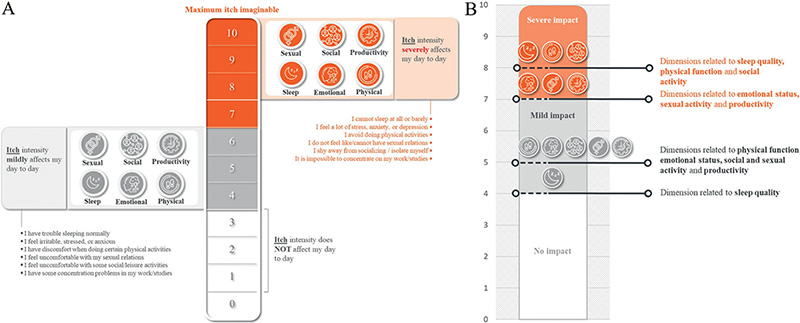
Fig. 4. Pruritus intensity scale for (A) patients and (B) healthcare professionals. Figure adapted and translated from the original version found in Appendix S1.
DISCUSSION
In our project, we systematically reviewed the impact of pruritus on several domains of patients’ HRQoL to develop a guideline that could be used in clinical practice and help both clinicians and patients in evaluating pruritus intensity and impact on their HRQoL. To the best of our knowledge this is the first guideline developed with this aim.
The studies identified in the systematic search showed that pruritus negatively affects different dimensions of a patient’s HRQoL to an important extent. Sleep quality and the emotional domain were the most affected, and most frequently included in HRQoL tools, followed by other dimensions such as sexual activity, physical function and productivity.
Previously published studies have highlighted the relationship between pruritus and sleep quality. Pruritus can worsen at night, resulting in greater difficulty in falling asleep or awakening during the night, which might increase awareness of pruritus and lead to more scratching, and consequent daytime sleepiness (21, 22). Furthermore, it has also been shown that increased disease severity is associated with increased sleep disturbance and reduced sleep quality in patients with AD (21, 22). In this regard, sleep disturbance and/or insomnia can even lead to increased anxiety and depression (23). Indeed, patients with AD, especially those with moderate-to-severe forms of the disease, report high rates of anxiety and depression (24, 25). Our results from the systematic review and those reported from HCPs and patients participating in our project confirm those obtained in previous studies, and highlight the relevance of assessing pruritus in clinical practice.
Pruritus is a known frequent symptom of AD, imposing a great burden on patients (26), and it has previously been reported to affect the day-to-day activities and emotional well-being of patients with AD (27). Despite this, it is a frequently underestimated symptom in clinical practice (28). In this respect, previous studies have shown a lack of agreement between patients with AD and physicians regarding the severity of the disease (29, 30), similar to what has been observed in other skin conditions such as psoriasis (31). Thus, clinicians should be aware of the importance of pruritus and its consequences on patients’ day-to-day lives in order to reduce this symptom, which might lead to better overall HRQoL.
Previous studies have shown that pruritus perception is heterogeneous among patients with AD and can vary with disease severity (32, 33). In this context, this guideline may be a meeting point for both HCP and patients to harmonize their vision of pruritus intensity and its impact on patients’ HRQoL. In addition, our guideline provides counselling on how to use and interpret the results obtained in the questionnaire. It would also be useful for clinicians to assess the impact on the different domains of HRQoL, as patients might need to be followed up by a multidisciplinary team.
Limitations
Our project has some limitations. The guideline was developed by 7 members of the SC and 15 patients. Although this might seem a low number of participants, it is within the recommended range for focus groups. On the one hand, members of the SC had wide expertise in their field as did patients, who were expert patients. On the other hand, the total number of participating patients was rather small to establish pruritus intensity thresholds. However, these were established and validated by two independent groups of patients, including adolescents and adults.
Conclusion
The guideline for interpreting the pruritus rating scale can help both adolescent and adult patients in more objectively assessing pruritus intensity and HCP when evaluating which HRQoL domains might be most affected by pruritus in patients with moderate-to-severe AD. However, further observational studies with a higher number of patients are needed to validate or better define the intensity thresholds generally and for adolescent and adult subgroups.
ACKNOWLEDGEMENTS
The authors would like to thank the patients who participated in the study and the AADA. The authors would also like to thank Outcomes’10 and Héctor D. de Paz, at Outcomes’10, for providing methodological consultancy. This service was funding by Abbvie.
The project was funded by Abbvie. The experts involved in this project expressed the desire to publish the outcomes and finally they requested Abbvie-sponsored writing support. Abbvie was not directly involved on the elaboration of the manuscript. Abbvie have had the opportunity to review the content.
REFERENCES
- Weidinger S, Novak N. Atopic dermatitis. Lancet 2016; 387: 1109–1122.
- Silverberg JI, Feldman SR, Smith Begolka W, Johnson MB, Stanojev C, DiBonaventura M, et al. Patient perspectives of atopic dermatitis: comparative analysis of terminology in social media and scientific literature, identified by a systematic literature review. J Eur Acad Dermatol Venereol 2022; 36: 1980–1990.
- Eckert L, Gupta S, Gadkari A, Mahajan P, Gelfand JM. Burden of illness in adults with atopic dermatitis: analysis of National Health and Wellness Survey data from France, Germany, Italy, Spain, and the United Kingdom. J Am Acad Dermatol 2019; 81: 187–195.
- Weidinger S, Beck LA, Bieber T, Kabashima K, Irvine AD. Atopic dermatitis. Nat Rev Dis Primers 2018; 4: 1.
- Silverberg JI. Atopic dermatitis in adults. Med Clin North Am 2020; 104: 157–176.
- Langan SM, Irvine AD, Weidinger S. Atopic dermatitis. Lancet 2020; 396: 345–360.
- Simpson EL, Bieber T, Eckert L, Wu R, Ardeleanu M, Graham NM, et al. Patient burden of moderate to severe atopic dermatitis (AD): insights from a phase 2b clinical trial of dupilumab in adults. J Am Acad Dermatol 2016; 74: 491–498.
- Sicras-Mainar A, Navarro-Artieda R, Armario-Hita JC. Severe atopic dermatitis in Spain: a real-life observational study. Ther Clin Risk Manag 2019; 15: 1393–1401.
- Barbarot S, Auziere S, Gadkari A, Girolomoni G, Puig L, Simpson EL, et al. Epidemiology of atopic dermatitis in adults: results from an international survey. Allergy 2018; 73: 1284–1293.
- Kaaz K, Szepietowski JC, Matusiak Ł. Influence of itch and pain on sleep quality in atopic dermatitis and psoriasis. Acta Derm Venereol 2019; 99: 175–180.
- Silverberg JI, Gelfand JM, Margolis DJ, Boguniewicz M, Fonacier L, Grayson MH, et al. Symptoms and diagnosis of anxiety and depression in atopic dermatitis in U.S. adults. Br J Dermatol 2019; 181: 554–565.
- Ständer S, Augustin M, Reich A, Blome C, Ebata T, Phan NQ, et al. Pruritus assessment in clinical trials: consensus recommendations from the International Forum for the Study of Itch (IFSI) Special Interest Group Scoring Itch in Clinical Trials. Acta Derm Venereol 2013; 93: 509–514.
- Storck M, Sandmann S, Bruland P, Pereira MP, Steinke S, Riepe C, et al. Pruritus Intensity Scales across Europe: a prospective validation study. J Eur Acad Dermatol Venereol 2021; 35: 1176–1185.
- Yosipovitch G, Reaney M, Mastey V, Eckert L, Abbé A, Nelson L, et al. Peak Pruritus Numerical Rating Scale: psychometric validation and responder definition for assessing itch in moderate-to-severe atopic dermatitis. Br J Dermatol 2019; 181: 761–769.
- Reich A, Szepietowski JC. Pruritus intensity assessment: challenge for clinicians. Expert Rev Dermatol 2013; 8: 291–299.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021; 372: n71.
- Higgins J, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane Handbook for systematic reviews of interventions, 2nd ed. Chichester, UK: Wiley, 2019.
- von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol 2008; 61: 344–349.
- Howick J, Chalmers I, Glasziou P, Greenhalgh T, Heneghan C, Liberati A, et al. The 2011 Oxford CEBM Levels of Evidence (Introductory Document). Oxford Centre for Evidence-Based Medicine. [Accessed October 2023] Available from: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence.
- Barbour R. Doing focus groups, 2nd ed. The SAGE Qualitative Research Kit, 2018.
- Chang YS, Chiang BL. Sleep disorders and atopic dermatitis: a 2-way street? J Allergy Clin Immunol 2018; 142: 1033–1040.
- Bawany F, Northcott CA, Beck LA, Pigeon WR. Sleep disturbances and atopic dermatitis: relationships, methods for assessment, and therapies. J Allergy Clin Immunol Pract 2021; 9: 1488–1500.
- Hertenstein E, Feige B, Gmeiner T, Kienzler C, Spiegelhalder K, Johann A, et al. Insomnia as a predictor of mental disorders: a systematic review and meta-analysis. Sleep Med Rev 2019; 43: 96–105.
- Marron SE, Tomas-Aragones L, Boira S, Campos-Rodenas R. Quality of life, emotional wellbeing and family repercussions in dermatological patients experiencing chronic itching: a pilot study. Acta Derm Venereol 2016; 96: 331–335.
- Salfi F, Amicucci G, Ferrara M, Tempesta D, De Berardinis A, Chiricozzi A, et al. The role of insomnia in the vulnerability to depressive and anxiety symptoms in atopic dermatitis adult patients. Arch Dermatol Res 2023; 315: 1577–1582.
- Fasseeh AN, Elezbawy B, Korra N, Tannira M, Dalle H, Aderian S, et al. Burden of atopic dermatitis in adults and adolescents: a systematic literature review. Dermatol Ther (Heidelb) 2022; 12: 2653–2668.
- Armario-Hita JC, Artime E, Vidal-Vilar N, Huete T, Díaz-Cerezo S, Moro RM, et al. Patient-reported outcome measures in real-world atopic dermatitis studies in Spain: a systematic review. Actas Dermosifiliogr 2022; 113: 685–704.
- Kantor R, Dalal P, Cella D, Silverberg JI. Research letter: Impact of pruritus on quality of life – a systematic review. J Am Acad Dermatol 2016; 75: 885–886.e884.
- Wei W, Anderson P, Gadkari A, Blackburn S, Moon R, Piercy J, et al. Discordance between physician- and patient-reported disease severity in adults with atopic dermatitis: a US cross-sectional survey. Am J Clin Dermatol 2017; 18: 825–835.
- Torrelo A, Ortiz J, Alomar A, Ros S, Prieto M, Cuervo J. Atopic dermatitis: impact on quality of life and patients’ attitudes toward its management. Eur J Dermatol 2012; 22: 97–105.
- Paul C, Bushmakin A, Cappelleri J, Mallbris L, Mamoto C. Do patients and physicians agree in their assessment of the severity of psoriasis? Insights from tofacitinib phase 3 clinical trials. J Dermatol Clin Res 2015; 3: 1048.
- Chee A, Branca L, Jeker F, Vogt DR, Schwegler S, Navarini A, et al. When life is an itch: what harms, helps, and heals from the patients’ perspective? Differences and similarities among skin diseases. Dermatol Ther 2020; 33: e13606.
- Takeuchi S, Oba J, Esaki H, Furue M. Non-corticosteroid adherence and itch severity influence perception of itch in atopic dermatitis. J Dermatol 2018; 45: 158–164.