SHORT COMMUNICATION
Burden of Skin and Subcutaneous Diseases in Indonesia 1990 to 2019
Faida Ufaira PRAMESWARI1, Farizal Rizky MUHARRAM2, Trisniartami SETYANINGRUM3 and Cita Rosita Sigit PRAKOESWA3*
1Faculty of Medicine, Universitas Airlangga/Dr Soetomo General Academic Hospital, Surabaya, Indonesia, 2Harvard Medical School, Harvard University, Boston, MA, USA and 3Department of Dermatology and Venereology, Faculty of Medicine, Universitas Airlangga/Dr Soetomo General Academic Hospital, Jl. Mayjen. Prof. Dr. Moestopo No. 6–8 Surabaya 60131, Indonesia. *E-mail: cita-rosita@fk.unair.ac.id
Citation: Acta Derm Venereol 2023; 103: adv18291. DOI: https://doi.org/10.2340/actadv.v103.18291.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: Oct 24, 2023; Published: Dec 19, 2023
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Skin and subcutaneous diseases place a significant burden on people of all ages and socioeconomic backgrounds in Asia and may have a significant impact on the quality of life of patients. The burden of diseases within the Asian population vary between countries, especially in countries in the Southeast Asian region, which are reported to have emerging infectious diseases. Furthermore, the burden of skin diseases varies greatly regarding socioeconomic and geographical distributions. It is crucial that efforts to reduce the burden of skin diseases are country-specific (1).
Indonesia, as the world’s largest island nation (approximately 6,000 inhabited islands) and the fourth most populated country, lacks studies on the quantitative impact of skin diseases, more specifically the epidemiology and burden of skin diseases at the regional level (1–3). By focusing on the Indonesian population, the burden of skin and subcutaneous diseases can be explored from a tropical country’s perspective. Moreover, skin diseases associated with neglected tropical diseases have become an even bigger problem since the emergence of COVID-19 (SARS-CoV-2) and need to be reviewed as a major public health problem in Indonesia (2, 4).
Interventions aimed at skin and subcutaneous diseases should be directed to areas with high disability-adjusted life years (DALYs). Reviewing the DALYs of skin and subcutaneous diseases over time is useful as a guide in healthcare planning, identifying root causes, improving health disparities, and even initiating action at the policy-maker level (1).
This observational study aimed to assess the regional burden of skin and subcutaneous diseases in Indonesia by trend analysis of the burden, in DALYs, of skin diseases in Indonesia from 1990 to 2019 (Fig. 1 and Fig. S1).
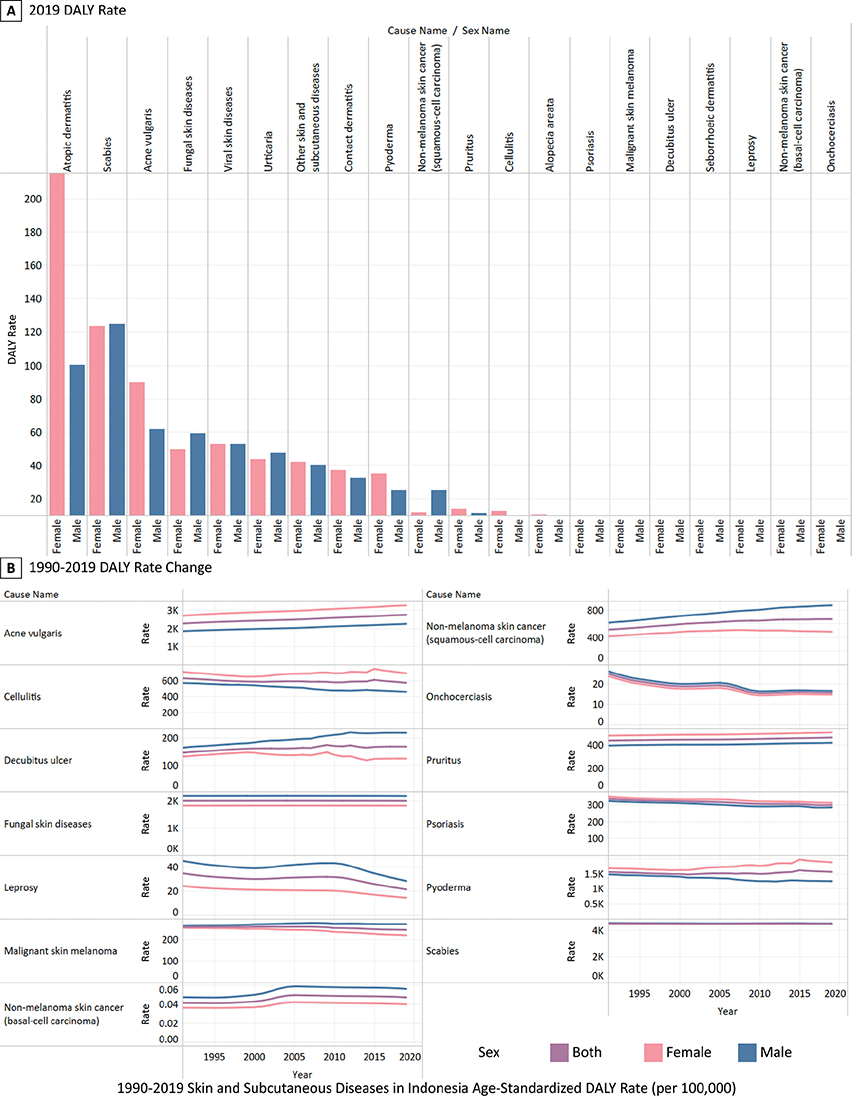
Fig. 1. Age-standardized disability-adjusted life year (DALY) rate (per 100,000) for selected skin and subcutaneous disease subcategories by sex in Indonesia. (A) DALY rate in 2019. (B) Change in DALY rate from 1990 to 2019.
MATERIALS AND METHODS
This cohort study comprised a secondary data analysis of the Global Burden of Disease Study 2019 (GBD 2019). GBD 2019 was used to obtain data on DALYs of skin and subcutaneous diseases in Indonesia from 1990 to 2019. The data collection methods of GBD are explained in detail in the GBD 2019 publication (5). For this study, the selected disease categories were acne vulgaris, alopecia areata, atopic dermatitis, cellulitis, contact dermatitis, decubitus ulcer, fungal skin diseases, leprosy, malignant skin melanoma, non-melanoma skin cancer (basal cell carcinoma), non-melanoma skin cancer (squamous cell carcinoma), pruritus, psoriasis, pyoderma, scabies, seborrhoeic dermatitis, urticaria, viral skin diseases, and other skin and subcutaneous diseases, each selected with the consideration of the data availability. Other skin and subcutaneous diseases classified various skin conditions that are less common or lack data availability (Table SI). Neglected tropical diseases with cutaneous manifestations were also included because Indonesia is heavily burdened by tropical diseases (6).
DISCUSSION
Skin and subcutaneous diseases were the fourth largest cause of non-fatal disease burden and disability worldwide in 2010 and 2013 (7). In 2016, skin diseases were known to be one of the 3 leading diseases contributing to DALYs for the age group 5–14 and 10–19 years in Indonesia (8). These data showed the significant impact of skin and subcutaneous diseases burden worldwide.
DALY rates varied in every province and can be affected by numerous factors, such as socioeconomic status, access and quality of dermatological care, insurance coverage, public health screening and prevention programmes, demographic characteristics, migration patterns, weather and climate, and environmental exposures (9). The need for targeted interventions in in regional and provincial levels to manage health inequality is justified by large disparities in DALYs despite the establishment of national health insurance (10).
Differences in age-standardized DALY rates between men and women were significant in several diseases. Skin cancers were found to have higher DALY rates in men than women, which may be associated with poor sun-protective behaviours (sunscreen application, wearing wide brim hats, limiting outdoor activity, and seeking shade), outdoor work, delayed screening and diagnosis, and less concern about recurrence (9).
Indonesia was also faced with the problem of neglected tropical diseases. Skin-associated tropical diseases can cause disability, disfigurement, stigmatization, and other socioeconomic problems (6). Diseases observed in the neglected tropical diseases category were scabies, leprosy, and fungal skin diseases. Each disease had a very different impact on the population compared with the other neglected tropical diseases. Scabies was observed to have the second highest DALY rate, followed by fungal skin diseases on thefourth highest DALY rate, while leprosy’s DALYrates were on the lowest 5 rank across the years (Table SII). The progress of each neglected tropical disease was widely different; therefore interventions unique to each disease and disease group are necessary to achieve the desired outcome in every disease (6).
Papua had the highest burden of skin and subcutaneous diseases in the country. Poorer health outcomes may be associated with poorer economic status (11). Papua has a low socioeconomic status, from having the highest percentage of urban slum households, the lowest percentage of decent sanitation access, and the fifth lowest access to decent and sustainable drinking water services (12). The lack of decent living standards, sanitation, and clean water greatly affected health outcomes and is associated with poor health (7).
These results have implications for public health officials and medical professionals to better understand the overall health status and disease burden in Indonesia. Differences were also found in health burdens between provinces, highlighting the need for integrated policies at the provincial and district levels to close the gaps in health outcomes. Improving the quality, reliability, and availability of data at the provincial levels is necessary to increase the accuracy and usefulness of health estimates in addressing health inequalities. Targeted interventions can be developed by examining health variations within provinces at finer geospatial levels (10). Dermatoses with the highest burden in each area (Table SII) should be the main focus of interventions (7). The current study helps identify gaps in dermatology disease conditions and will further reinforce health priority decisions and public policy efforts in Indonesia.
Since it is part of the GBD study, all of the limitations of the GBD methodology affected this study (10). This study was limited by the availability of the latest data, as the data source only provided data up to 2019. The accuracy of the estimates depends on the availability of data by period. The sparsity of data on numerous skin and subcutaneous diseases showed inadequate data reporting and deficiencies in the implementation of the healthcare database in Indonesia, which can alter the DALY rates (9).
In conclusion, the burden of skin and subcutaneous diseases in Indonesia varies by geographical and sex distribution. Gaps in medical interventions for different diseases still exist. Access to healthcare is also an important aspect in controlling the burden of diseases. Provinces in Indonesia had different socioeconomic backgrounds that differently affected the health focus; therefore, interventions should be tailored to the unique geographical and socioeconomic varieties of each province, in order to tackle inequalities at the regional level. Data reporting on skin and subcutaneous diseases in Indonesia was still inadequate and needs to be improved to increase the accuracy and usefulness of health estimates.
REFERENCES
- Urban K, Chu S, Giesey RL, Mehrmal S, Uppal P, Delost ME, et al. Burden of skin disease and associated socioeconomic status in Asia: a cross-sectional analysis from the Global Burden of Disease Study 1990–2017. JAAD Int 2021; 2: 40–50.
- Simanjuntak AM, Dean P, Marbun U, Anggraini YE. Post COVID-19 leprosy infection: the threat of post-pandemic neglected tropical disease for Indonesia. J Ilmiah Mahasiswa Kedokteran Indonesia 2022; 10: 35–44.
- Tan M, Kusriastuti R, Savioli L, Hotez PJ. Indonesia: an emerging market economy beset by neglected tropical diseases (NTDs). PLoS Negl Trop Dis 2014; 8: e2449.
- Fauziyah S, Putri SMD, Salma Z, Wardhani HR, Nisa’ Hakim FK, Sucipto TH, et al. How should Indonesia consider its neglected tropical diseases in the COVID-19 era? Hopes and challenges (Review). Biomed Rep 2021; 14: 1–10.
- Abbafati C, Abbas KM, Abbasi-Kangevari M, Abd-Allah F, Abdelalim A, Abdollahi M, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet 2020; 396: 1204–1222.
- World Health Organization (WHO). Ending the neglect to attain the Sustainable Development Goals: a road map for neglected tropical diseases 2021–2030. 2021 [cited 2023 Mar 10]. Available from: https://www.who.int/publications/i/item/9789240010352.
- Chu S, Mehrmal S, Uppal P, Giesey RL, Delost ME, Delost GR. Burden of skin disease and associated socioeconomic status in Europe: an ecologic study from the Global Burden of Disease Study 2017. JAAD Int 2020; 1: 95–103.
- Gani A, Budiharsana MP. The Consolidated Report on Indonesia Health Sector Review 2018. 2019 [cited 2023 Mar 10]. Available from: https://www.unicef.org/indonesia/reports/consolidated-report-indonesia-health-sector-review-2018
- Laughter MR, Maymone MBC, Karimkhani C, Rundle C, Hu S, Wolfe S, et al. The burden of skin and subcutaneous diseases in the United States from 1990 to 2017. JAMA Dermatol 2020; 156: 874–881.
- Mboi N, Syailendrawati R, Ostroff SM, Elyazar IR, Glenn SD, Rachmawati T, et al. The state of health in Indonesia’s provinces, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Glob Health 2022; 10: e1632–45.
- McMaughan DJ, Oloruntoba O, Smith ML. Socioeconomic status and access to healthcare: interrelated drivers for healthy aging. Front Public Health 2020; 8: 231.
- Hikmah IR, Hikmah Y. Spatial panel modeling of factors affecting health in Papua Province. J Data Analysis 2020; 2: 96–108.