QUIZ SECTION
Pruritic Palpable Purpura on the Lower Legs: A Quiz
Shin IINUMA1,2, Takahiro KOBAYASHI1 and Akemi ISHIDA-YAMAMOTO2
1Department of Dermatology, Japanese Red Cross Kitami Hospital, North 6, East 2, Kitami, 090-8666 and 2Department of Dermatology, Asahikawa Medical University, Asahikawa, Japan. E-mail: iinuma@asahikawa-med.ac.jp
Citation: Acta Derm Venereol 2023; 103: adv18366. DOI https://doi.org/10.2340/actadv.v103.18366.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Published: Sep 14, 2023
A 64-year-old Japanese man presented with a 5-year history of recurrent pruritic papules on the lower legs. Physical examination revealed multiple palpable purpura and haemorrhagic vesicles irregularly distributed on his lower legs (Fig. 1). Skin biopsy of the affected area showed perivascular inflammatory infiltrates composed predominantly of eosinophils throughout the dermis. Leukocytoclastic vasculitis was also observed, comprising fibrinoid degeneration, leukocytoclasia, and erythrocyte extravasation from the dermal vessels (Fig. 2). Direct immunofluorescence showed immunoglobulin M and C3 deposition within the dermal vessel walls and was negative for immunoglobulins G and A. Laboratory studies revealed normal peripheral eosinophils levels (220/μl). Antinuclear antibody, rheumatoid factor, anti-cyclic citrullinated peptide antibody, proteinase-3, myeloperoxidase-antineutrophil cytoplasmic antibodies (ANCA) and cryoglobulins tested negative. Serum complement levels were normal. The patient had no history of allergic diseases, such as bronchial asthma or allergic rhinitis. No other clinical signs, symptoms, or laboratory findings were associated with internal organ involvement.

Fig. 1. Clinical presentation. (A) Multiple palpable purpura distributed irregularly over the lower legs. (B) Palpable purpura and haemorrhagic vesicles of various sizes.
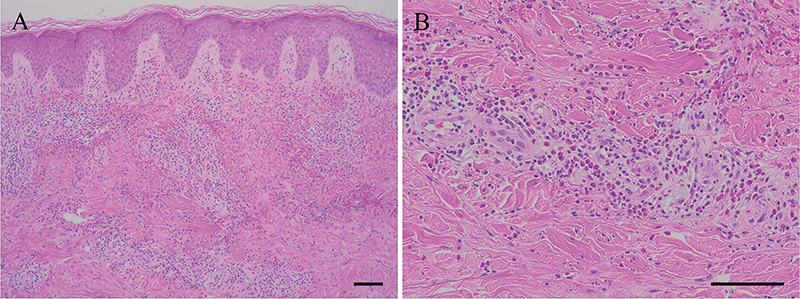
Fig. 2. Histopathological finding. (A) Perivascular inflammatory infiltrate composed predominantly of eosinophils throughout the dermis (haematoxylineosin, scale bar: 100 µm). (B) Leukocytoclastic vasculitis of the dermal vessels with marked infiltration of eosinophils (scale bar: 100 µm).
What is your diagnosis? See next page for answer.
ANSWERS TO QUIZ
Pruritic Palpable Purpura on the Lower Legs: A Commentary
Diagnosis: Recurrent cutaneous eosinophilic vasculitis
Based on these findings, the patient was diagnosed with recurrent cutaneous eosinophilic vasculitis (RCEV). A lack of a history of bronchial asthma, allergic rhinitis, and peripheral blood eosinophilia ruled out the possibility of eosinophilic granulomatosis with polyangiitis (EGPA). Furthermore, the absence of persistent peripheral blood eosinophilia and lack of systemic disease excluded hyper-eosinophilic syndrome (HES). The skin lesions were limited to the lower legs; therefore treatment with high-potency topical corticosteroids was initiated to alleviate the lesions. The lesions were recurrent; however, they improved after treatment with topical corticosteroids. The patient was followed up for 10 years without systemic corticosteroids; however, no systemic involvement was observed.
RCEV, also known as recurrent cutaneous necrotizing eosinophilic vasculitis (RCNEV), is a rare disease characterized by necrotizing vasculitis of the dermal small vessels with eosinophilic infiltration (1, 2). The cutaneous manifestations of RCEV include multiple pruritic, erythematous, or purpuric papules, plaques, or angioedema, more commonly affecting the lower extremities. Their pathogenesis remains unclear; however, these lesions have a chronic relapsing course without systemic involvement. The disease is typically associated with peripheral blood eosinophilia; however, the number of eosinophils does not necessarily correlate with the severity of the cutaneous symptoms. The proposed diagnostic criteria for RCEV further support the diagnosis in the current case (3).
The histopathological features of RCEV are characterized by necrotizing vasculitis of small dermal vessels with prominent eosinophilic infiltration (4). An eosinophilic infiltrate was observed around the vascular plexus in the dermis, although the subcutis may have been involved. Fibrinoid degeneration of vessel walls and intraluminal thrombi are common and may be complicated by epidermal ischemic necrosis. Direct immunofluorescence analysis of RCEV typically yields negative results for immunoglobulins and C3 proteins. The current case presented as leukocytoclastic vasculitis with marked eosinophilic infiltration. RCEV typically shows minimal or no leukocytoclasis; however, several reports have described the presence of leukocytoclastic vasculitis, as observed in the current patient. These histopathological findings may be similar to those in EGPA, although there is no evidence of extravascular granulomas in RCEV. Therefore, patients with RCEV may mimic ANCA-negative EGPA and should be followed up. Eosinophilic leukocytoclastic vasculitis (ELV) was also a possible diagnosis in the current patient (5). ELV presents clinically as palpable purpura, indistinguishable from the classic cutaneous leukocytoclastic vasculitis. It can be caused by infections, drugs, or other triggers, similar to the classic cutaneous leukocytoclastic vasculitis. In the current patient, the chronic relapsing nature of the disease supported the diagnosis of RCEV rather than ELV.
RCEV responds well to systemic corticosteroids and/or high-potency topical corticosteroids (3). Oral corticosteroids are the mainstay of treatment; however, relapses often occur during dose tapering. Therefore, long-term maintenance therapy is required in most cases of RCEV. The steroid-sparing therapies include suplatast tosilate, indomethacin, tacrolimus, and dapsone. RCEV typically exhibits a benign chronic course without systemic involvement. The clinical course of the current patient was not progressive; therefore, systemic corticosteroids were not administered. To our knowledge, there are only a few case reports of RCEV treated with topical corticosteroids alone. During the 10-year follow-up, the patient presented with a chronic relapsing course without systemic disease under topical corticosteroid therapy.
In conclusion, we report here a case of RCEV presenting as leukocytoclastic vasculitis with marked eosinophilic infiltration. The patient had a chronic, benign disease course and received topical corticosteroid therapy alone. This case highlights that the clinical and histological manifestations of RCEV are highly variable. In contrast to EGPA and HES, this disease has a benign chronic course with no evidence of systemic involvement. RCEV is a potential diagnosis in patients presenting with cutaneous vasculitis; however, it is rare. Recognition of this disease is essential to ensure appropriate diagnosis and management.
REFERENCES
- Lin TL, Yang CS, Chen YJ. Recurrent cutaneous necrotising eosinophilic vasculitis. Australas J Dermatol 2021; 62: e102–e106.
- Sawada C, Taniai M, Kawashima M, Ishiguro N. Recurrent cutaneous eosinophilic vasculitis. Eur J Dermatol 2016; 26: 108–109.
- Quijano-Gomero EG, Rodríguez-Zúñiga MJM, Sanz-Montero ME, Durand-Buse D. Clinical, dermoscopic and histologic features of recurrent cutaneous eosinophilic vasculitis cases. Actas Dermosifiliogr (Engl Ed) 2019; 110: 590–596.
- Li W, Cao W, Song H, Ciu Y, Lu X, Zhang F. Recurrent cutaneous necrotizing eosinophilic vasculitis: a case report and review of the literature. Diagn Pathol 2013; 8: 185.
- Ratzinger G, Zankl J, Eisendle K, Zelger B. Eosinophilic leukocytoclastic vasculitis – a spectrum ranging from Wells’ syndrome to Churg-Strauss syndrome? Eur J Dermatol 2014; 24: 603–610.