SHORT COMMUNICATION
Necrotic Ulcers from Occlusive Vasculopathy Associated with Monoclonal B Cell Lymphocytosis
Delwyn Zhi Jie LIM1, Shang-Ian TEE1, Ling CAO2 and Ding Yuan WANG1
1National Skin Centre, 1 Mandalay Rd, Singapore 308205 and 2Department of Haematology, Tan Tock Seng Hospital, Singapore. E-mail: delwynlim@outlook.com
Citation: Acta Derm Venereol 2023; 103: adv18371. DOI https://doi.org/10.2340/actadv.v103.18371.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: Oct 9, 2023; Published: Nov 28, 2023
INTRODUCTION
Dermatological manifestations in B-cell lymphomas commonly include skin-coloured to pink papules, nodules or plaques on the trunk or extensor surfaces of extremities secondary to direct lymphomatous infiltration. We present here a case of necrotic ulcers due to occlusive vasculopathy from IgM paraproteinaema and cold agglutinin disease, in a patient with newly diagnosed chronic lymphocytic leukaemia-like monoclonal B cell lymphocytosis (CLL-like MBL).
CASE REPORT
An 82-year-old female with a past medical history of hypertension, hyperlipidaemia and well-controlled gout was admitted to hospital due to breathlessness and leg swelling. She subsequently developed worsening tender ulcers over the left arm. Examination revealed stellate ulcers over the left forearm (Fig. 1A, B) with necrotic eschars and faint adjacent retiform purpura.
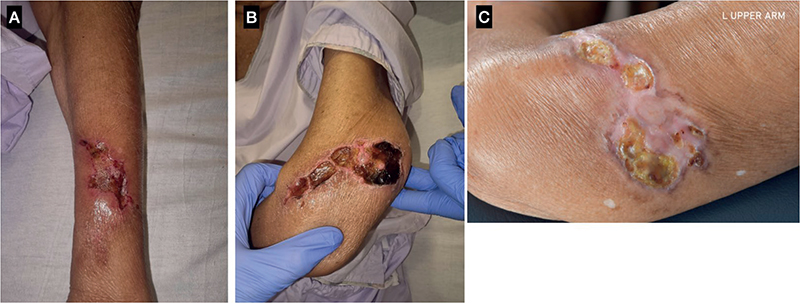
Fig. 1. Clinical photographs. (A) Necrotic ulcers with overlying haemorrhagic crusts over the left forearm and (B) left elbow. (C) Healing, dried crusts over left elbow.
A skin biopsy was performed (Fig. 2). Histologically, the superficial vessels showed occlusion by red cells along with an amorphous material, which was strongly positive on IgM immunoperoxidase stain, suggestive of an occlusive vasculopathy.
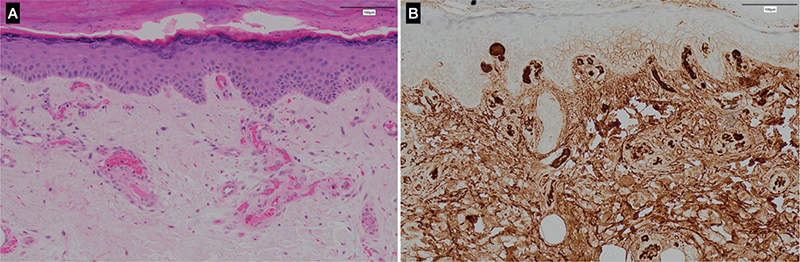
Fig. 2. Histopathology. (A) Blood vessels in the superficial dermis show complete occlusion by red blood cells admixed with an amorphous eosinophilic material. There is a surrounding sparse perivascular lymphocytic infiltrate (haematoxylin and eosin (H&E), original magnification 200×). (B) The eosinophilic material stains positive with immunoglobulin M (IgM) immunoperoxidase stain.
Further investigation revealed anaemia (haemoglobin (Hb) 5.0 g/dL) and thrombocytopaenia (28×109/L) with a normal lymphocyte count (2.3×109/L). Peripheral blood film showed marked red cell agglutination. Direct Coombs test was positive for anti-C3d. Serum electro-phoresis and immunofixation showed a weak immunoglobulin M (IgM)-kappa monoclonal band with raised serum IgM level at 2.6 g/L (normal range 0.40–2.30 g/L). Her cold agglutinins returned positive with a titre of 128 μg/mL, but cryoglobulins were negative. A whole-body computed tomography scan did not reveal any enlarged lymph nodes or splenomegaly.
Bone marrow aspiration and trephine was done to look for possible lymphoproliferative disease (LPD). Flow cytometry found a small population (1.1%) of clonal small B cells with a non-specific phenotype. They were kappa-restricted, CD5-/ CD10-/ CD23dim/ CD20+/CD22+/CD79b-dim/CD38- with asynchronous CD27+/smIgm-/CD200+/CD305-/CD39dim expression. Immunophenotyping from the flow cytometry favoured a diagnosis of lymphoplasmacytic lymphoma (LPL) or marginal zone lymphoma (MZL). However, the bone marrow biopsy showed adequate haematopoiesis with nodular paratrabecular aggregates of small lymphocytes positive for CD20/ CD5/ CD23 /BCL2/ LEF1, negative for CD21/ CD10/ BCl6/ CD3/ cyclin D1/ SOX11, which favoured a diagnosis of chronic lymphocytic leukaemia (CLL) or small lymphocytic lymphoma (SLL). However, the patient did not fulfil the criteria for diagnosis of CLL or SLL as she did not have any lymphadenopathy, organomegaly or lymphoma-related cytopaenias. In addition, her peripheral blood B-lymphocytes were persistently <5 ×109/L. Her tests for CLL fluorescence in situ hybridization (FISH) panel and TP53 mutation were negative, supporting the lack of any high-risk genetic mutations.
In view of the high specificity of LEF1, the diagnosis of CLL-like MBL was made. The haematology team decided to manage the patient as CLL-like MBL with cold-agglutinin disease (CAD), complicated by skin ulceration from occlusive vasculopathy from her circulating IgM paraproteins and cold agglutinins. Her ulcers were managed conservatively and improved (Fig. 1C) after her first cycle of bendamustine-rituximab.
DISCUSSION
Occlusive non-vasculitic vasculopathies are characterized by retiform lesions, purpuras, ulcers or “purple toe syndrome” (1). Common causes of occlusive vasculopathies include embolization, platelet plugging, cryoglobulinaemia, vessel-invasive microorganisms and systemic or vascular coagulopathies.
There is a paucity of information in terms of cutaneous manifestations of MBL. However, common cutaneous manifestations of mature B cell lymphomas include reddish or violaceous skin papules, plaques, or nodules localized preferentially on the trunk or arms (2). These lesions typically reflect direct lymphomatous involvement in the skin. Reports of retiform purpura and necrotic skin ulcers in patients with mature B cell lymphomas from cryoglobulinaemia are well documented within the literature (3, 4) but our patient did not have cryoglobulins detected in her serum.
Our patient’s presentation of stellate ulcers with surrounding retiform purpura was due to direct luminal deposition of circulating monoclonal IgM, as well as cold agglutinin disease causing red cell agglutination, leading to occlusive vasculopathy. Paraproteins, specifically of the IgM subclass, owing to its pentameric structure and high molecular weight, may induce hyperviscosity leading to purpura and ulcers from vaso-occlusion (5).
To our knowledge, this is a novel report of non-cryoglobulinaemic occlusive vasculopathy of the skin in a patient with CLL-like MBL. Treatment should be directed at the underlying blood dyscrasia given that the cold agglutinins and IgM paraprotein are all secondary phenomena. Our patient’s ulcers showed significant improvement following treatment for her underlying disease. Clinicians should be cognizant of the various aetiological factors that may predispose patients with haematological malignancies to such cutaneous manifestations.
ACKNOWLEDGEMENTS
Patient consent has been obtained for the purpose of medical research, teaching or publications. The patient understands that he/she will not be identified by name in any such use of these photographs and patient anonymity is preserved.
The authors have no conflicts of interest to declare.
REFERENCES
- Llamas-Velasco M, Alegría V, Santos-Briz Á, Cerroni L, Kutzner H, Requena L. Occlusive nonvasculitic vasculopathy. Am J Dermatopathol 2017; 39: 637–662.
- Rossi D, Bertoni F, Zucca E. Marginal-zone lymphomas. N Engl J Med 2022; 386: 568–581.
- de Lorenzo-Pinto A, Pinilla Llorente B. Successful treatment with Bosentan for digital ulcers related to mixed cryoglobulinemia: a case report. Am J Ther 2016; 23: e1942–e1943.
- Gan C, Howard MD, Mulcahy A, Yazdabadi A. Painful ulcerations: the sole clinical sign of mixed cryoglobulinaemia secondary to marginal zone lymphoma. BMJ Case Rep 2022; 15: e247780.
- Appenzeller P, Leith CP, Foucar K, Scott AA, Bigler CF, Thompson CT. Cutaneous Waldenstrom macroglobulinemia in transformation. Am J Dermatopathol 1999; 21: 151–155.