QUIZ SECTION
Telangiectatic Macules Spreading During More Than 30 Years: A Quiz
Italo Francesco AROMOLO1, Eleonora DI MICHELE1, Francesca Laura BOGGIO2, Angelo CATTANEO3 and Angelo Valerio MARZANO1,3
1Department of Pathophysiology and Transplantation, Milan University, 2Pathology Unit and 3Dermatology Unit, Fondazione IRCCS, Cà Granda Ospedale Maggiore Policlinico, Milan, Italy. E-mail: italo.aromolo@unimi.it
Citation: Acta Derm Venereol 2024; 104: adv18429. DOI: https://doi.org/10.2340/actadv.v104.18429.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Published: Jan 25, 2024
A 65-year-old woman presented to our Dermatologic, Clinic of Ospedale Maggiore, Milan with asymptomatic skin lesions that had been present for approximately 35 years. The lesions started on her lower limbs and gradually spread to her abdomen. Her medical history revealed allergic asthma and early-stage osteoporosis, and she was not taking any medications. Examination revealed numerous isolated telangiectasias and erythematous blanching macules, and patches with telangiectasias within them on her abdomen and lower limbs (Fig. 1). A skin biopsy of the abdominal lesions, revealed dilated small vessels in the papillary dermis with an eosinophilic, thickened, wall (Fig. 2). Periodic acid–Schiff stained the hyaline material seen in blood vessel walls, while Congo red staining was negative. Routine blood tests, autoimmune panels, and coagulation profiles were all within normal limits. Venous Doppler ultrasonography was also normal.
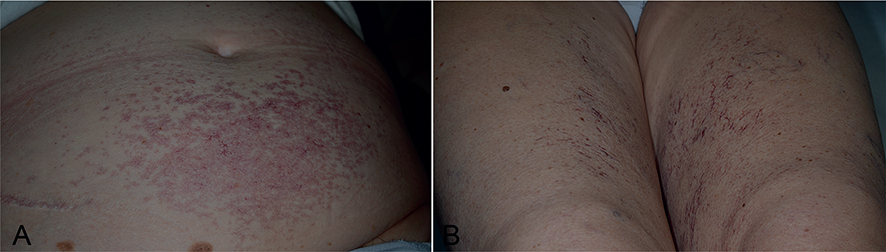
Fig. 1. (A) Erythematous blanchable macules and patches with telangiectasias located symmetrically on the lower abdomen. (B) Isolated linear telangiectasias located symmetrically on the inner thighs, without surrounding erythema.

Fig. 2. (A) Histopathology showing dilated blood vessels in the papillary dermis, with vascular walls thickened by eosinophilic hyaline material (haematoxylin and eosin, original magnification 25×). (B) Periodic acid–Schiff staining of hyaline material in blood vessel walls (original magnification 40×).
What is your diagnosis?
Differential diagnosis 1: cutaneous collagenous vasculopathy
Differential diagnosis 2: hereditary haemorrhagic telangiectasia
Differential diagnosis 3: generalized essential telangiectatic
Differential diagnosis 4: telangiectasia macularis eruptiva perstans
See next page for answer.
ANSWERS TO QUIZ
Telangiectatic Macules Spreading During More Than 30 Years: A: A Commentary
Diagnosis: Cutaneous collagenous vasculopathy
Cutaneous collagenous vasculopathy (CCV) is a rare idiopathic microangiopathy first described in 2000, with fewer than 50 cases reported to date worldwide (1). CCV primarily affects Caucasian adults, with a slightly higher prevalence in females, and has a mean onset age of 62 years. Only 1 paediatric case has been reported to date, in a 16-year-old patient. No familial cases have been reported to date (2). While the term “telangiectatic macules” is often used generically to describe CCV lesions, the clinical presentation comprises distinct lesions: blanching erythematous macules or patches with visible macroscopic telangiectasias (2), erythematous macules or patches lacking macroscopic telangiectasias (3), and isolated linear or pin-point telangiectasias without surrounding erythema (1, 2). Different types of lesions can coexist within a patient, potentially representing stages of the same process. Petechiae and ecchymosis are occasionally observed. The macules may darken gradually (4). Symmetrical lesions typically begin on the lower limbs, spreading progressively to the abdomen and trunk and, less commonly, to the upper limbs. Facial involvement is anecdotal (2). A singular case has been reported to originate bilaterally on the breasts (5). Mucous membranes and nail beds are unaffected. Lesions are often asymptomatic, although approximately 10% of patients report mild pruritus. Patients do not exhibit photosensitivity or seasonal variation. CCV is not associated with systemic manifestations, and routine laboratory tests and autoimmune panel are within normal ranges (2).
Histologically, CCV is characterized by dilated post-capillary venules located in the papillary dermis, with a vascular wall thickened by eosinophilic hyaline material. Perivascular inflammatory cells are usually absent, but a few lymphocytes can occasionally be observed (6). Extravasated erythrocytes or hemosiderin are minimal to none. Leukocytoclastic debris or fibrinoid necrosis of vessel walls are not seen (1). The material within blood vessel walls is positive for Periodic acid–Schiff staining but negative for Congo red and elastic staining. Blood vessel walls show positive staining with Masson trichrome (4), indicating accumulation of collagen fibre, and are also highlighted via immunohistochemistry for type IV collagen (7). Direct immunofluorescence is negative (5). Electron microscopy reveals a characteristic basal lamina reduplication in post-capillary venules (6). The first reports of CCV exhibited Luse bodies, which are collagen with an abnormal ultra-structural banding pattern. However, they lack specificity and may be sometimes absent in CCV (8).
The aetiopathogenesis of CCV is unclear. Several hypotheses have been proposed, including a primary genetic defect of collagen production in the microvasculature, systemic diseases, and medications (1). The more widely accepted theory suggests that there is endothelial cell damage that would lead to reparative fibrosis by hyperplastic endothelial cells and/or activated wall veil cells, resulting in abnormal and disorganized collagen deposition within blood vessel walls (6). Histologically, the rare observation of intravascular organizing fibrin thrombi supports the hypothesis of endothelial damage (8). However, the trigger event that causes endothelial cell damage is unknown (8).
When presented with diffuse telangiectasias, consideration of CCV and its differential diagnoses, such as generalized essential telangiectasia (GET), hereditary haemorrhagic telangiectasia (HHT), telangiectasia macularis eruptiva perstans (TMEP), and telangiectasias associated with drug administration is essential. A definitive diagnosis relies on histological examination, as none of these entities exhibit thickened vessel walls with eosinophilic deposition.
The course of CCV is benign, with a disease history ranging from weeks to years until diagnosis (2). Lesions spread slowly over time, lacking systemic progression, but potentially causing patient distress. The current case had a 35-year history, the longest reported in the literature (2), confirming the benign nature of this disease. Most patients reported in the literature did not receive therapy. In 1 case, a 585-nm pulsed dye laser was used for aesthetic purposes, resulting in some lesional fading (10). In conclusion, CCV is an idiopathic microangiopathy of dermal blood vessels with distinct histopathology. It is likely to be underdiagnosed and under-reported due to its benign and asymptomatic nature, as well as its clinical similarity to GET, which could potentially result in misdiagnosis.
ACKNOWLEDGEMENTS
The study was conducted in accordance with the ethics standards of the responsible committee on human experimentation (institutional and national, Cà Granda Ospedale Maggiore Policlinico, Milan, Italy), with the principles of the Declaration of Helsinki 1975, revised 2000, and the Taipei Declaration.
Written informed consent was obtained from the patient in this study, including for publication of photographs.
Anonymized data will be shared upon reasonable request from any qualified investigator for purposes of replicating procedures and results.
REFERENCES
- Salama S, Rosenthal D. Cutaneous collagenous vasculopathy with generalized telangiectasia: an immunohistochemical and ultrastructural study. J Cutan Pathol 2000; 27: 40–48.
- Castiñeiras-Mato I, Rodríguez-Lojo R, Fernández-Díaz ML, Bal-Nieves F. Cutaneous collagenous vasculopathy: a case report and review of the literature. Actas Dermo-sifiliograficas 2016; 107: 444–447.
- Karimkhani C, Boyers LN, Olivere J, Smith C. Cutaneous collagenous vasculopathy Cutis 2019; 103: E7–E8.
- Stavrou C, Uthayakumar A, Calonje JE, Bunker CB. Cutaneous collagenous vasculopathy. BMJ Case Rep 2021; 14: e241434.
- Borroni RG, Derlino F, Agozzino M, Concardi M, Arbustini E, Brazzelli V. Hypothermic cutaneous collagenous vasculopathy with centrifugal spreading. J Eur Acad Dermatol Venereol 2015; 29: 1444–1446.
- Salama SS. Cutaneous collagenous vasculopathy: a new case series with clinicopathologic and ultrastructural correlation, literature review, and insight into the pathogenesis Am J Dermatopathol 2015; 37: 368–375.
- Motegi SI, Yasuda M, Yamanaka M, Amano H, Ishikawa O. Cutaneous collagenous vasculopathy: report of first Japanese case and review of the literature. Australas J Dermatol 2017; 58: 145–149.
- Salama S, Chorneyko K, Belovic B. Cutaneous collagenous vasculopathy associated with intravascular occlusive fibrin thrombi. J Cutan Pathol 2014;41: 386–393.
- Echeverría B, Sanmartín O, Botella-Estrada R, Vitiello M. Cutaneous collagenous vasculopathy successfully treated with pulsed dye laser. Int J Dermatol 2012; 51: 1359–1362.