QUIZ SECTION
A Child with a Lump in the Neck: A Quiz
Dirk VAN GYSEL1,2, Sherief R. JANMOHAMED2, Hanne LOCY3, Daniel HOHL4 and Katleen DE SMEDT3
1Department of Pediatrics, O. L. Vrouw Hospital Aalst, Belgium, 2Department of Dermatology, Interdisciplinary Unit of Pediatric Dermatology, 3Department of Pathology, Vrije Universiteit Brussel (VUB), Universitair Ziekenhuis Brussel (UZ Brussel), Laarbeeklaan 101, BE-1090 Brussels, Belgium and 4Department of Dermatology, University Hospital CHUV, Lausanne, Switzerland. E-mail: dirk.vangysel@uzbrussel.be
Citation: Acta Derm Venereol 2024; 104: adv18485. DOI https://doi.org/10.2340/actadv.v104.18485.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Published: Jan 8, 2024
A 6-year-old boy with no significant past medical history presented with a lump in the neck. Apart from having many warts on the feet, which was the primary reason for the consultation, he was otherwise healthy. The lesion was first noticed at the age of 4 years as a small nodule with subsequent slow growth up to the current size.
On physical examination, he was found to have a firm non-tender dermal lump 1.5 cm × 0.5 cm. The even and smooth overlying skin had an orange-brown discoloration (Fig. 1). An excisional biopsy was performed. The epidermis was slightly acanthotic, orthokeratinized and showed no atypia. The dermis revealed a nodule composed of multiple nests with intervening connective fascicles. These nests consisted of spindle-shaped cells with a regular nucleus, surrounded by a halo (Fig. 2). Immunohistochemical staining for CD10, smooth muscle actin (SMA), microphtalmia-associated transcription factor (MiTF) and calponine were weakly positive, staining for CD63 (also known as NK1/C3) strongly positive (Fig. 3). Stains for S100 and neurone-specific enolase (NSE) were negative.

Fig. 1. Firm dermal lump in the neck.
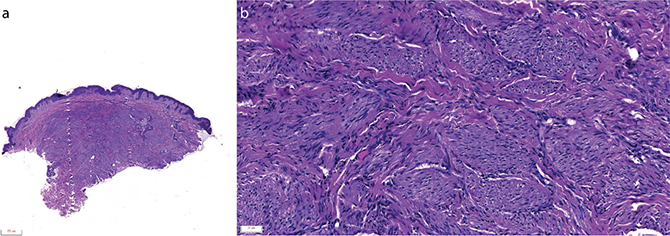
Fig. 2. Histology shows dermal nodules composed of multiple nests with intervening connective fascicles (Fig. 2a: Haematoxylin & eosin (H&E) stain, magnification: 2×). These nests consist of spindle-shaped cells with a regular nucleus, surrounded by a halo (Fig. 2b H&E stain, magnification: 20×).
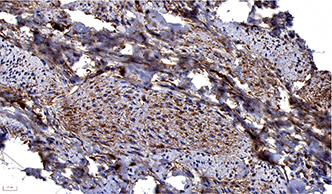
Fig. 3. Immunohistochemistry shows strongly positive staining for NK1/C3 (magnification: 40×).
What is your diagnosis?
Differential diagnosis 1: Cellular neurothekeoma
Differential diagnosis 2: Dermatofibroma
Differential diagnosis 3: Cervical adenopathy
Differential diagnosis 4: Leiomyoma
See next page for answer.
ANSWERS TO QUIZ
A Child with a Lump in the Neck: A Commentary
Diagnosis: Cellular neurothekeoma
The clinical features, pathology, and immunohistochemical (IHC) pattern are diagnostic of cellular neurothekeoma. Neurothekeoma is a rare, benign, cutaneous neoplasm with a very low incidence during childhood (1), that was first described in 1969 by Harkin & Reed as nerve sheath myxoma (2). In 1980 Gallager & Helwig published the first large series and introduced the name “neurothekeoma” (3) to connote both the histological nested (theque) appearance and the purported nerve sheath differentiation. To date, there is general agreement that true nerve sheath myxoma is distinct from neurothekeoma, as cellular neurothekeoma stains for fibrohistiocytic markers and Preferentially expressed Antigen in MElanoma (PRAME), while nerve sheath myxoma stains for neural markers (4, 5).
Clinically, neurothekeomas present as asymptomatic, slow-growing, solitary, reddish dome-shaped lesions affecting the upper parts of the body, such as face, neck, and arms. Occurrence in the oral mucosa, paranasal sinuses, and eyelids has occasionally been reported (6). Tumour size ranges from 0.3 to 2.0 cm, but giant lesions up to 6 cm have been described (1). The clinical differential diagnosis includes pyogenic granuloma, keloid, juvenile xanthogranuloma, dermatofibroma, epidermal cyst, neurofibroma, cellular blue naevus, Spitz naevus, melanoma, basal cell carcinoma, leiomyoma, cutaneous lymphoid hyperplasia and lymphomatoid papulosis (7).
As the clinical presentation tends to be non-specific, the distinct histopathological findings are imperative for diagnosis. Neurothekeomas are composed of distinct lobules of epithelioid and spindle cells separated by fibrous connective tissue with a plentiful myxoid matrix. Traditionally 3 main subcategories, cellular, myxoid, and mixed, have been described, based on the amount of mucin, cellularity, growth pattern, and IHC profile (8). The form designated “cellular neurothekeoma” is composed of ill-defined nests of epithelioid cells associated with scant mucin. Cellular (and mixed) neurothekeomas have negative S100 staining, indicating they are not of Schwann cell origin. They are also negative for epithelial membrane antigen (EMA), indicating they are not of perineural cell origin either. Indeed, cellular neurothekeomas are now thought to be of fibrohistiocytic origin (9).
The histological differential diagnosis of neurothekeoma includes low-grade epithelioid malignant peripheral nerve sheath tumour (MPNST) of the skin and subcutis, melanocytic lesions, cutaneous leiomyoma, epitheloid Spitz naevi and plexiform fibrohistiocytic tumours. In contrast with cellular neurothekeoma, nerve sheath tumours and melanocytic naevi are both positive for S-100. Cutaneous leiomyoma shows a characteristic intersecting fascicular pattern and is desmin-positive. Plexiform fibrohistiocytic tumour has biphasic appearance and a plexiform growth pattern. MiTF can be helpful to distinguish these 2 entities, as it can be partially positive in neurothekeomas, whereas in plexiform fibrohistiocytoma the marker is negative.
Neurothekeomas are essentially benign tumours; however, atypical transformation is possible, leading to an aggressive and invasive behaviour (10).
As for treatment, wide local excision with frozen-section–margin control is recommended in order to prevent recurrence and local invasion (6).
To conclude, neurothekeomas are rare, benign tumours that most often occur on the head, neck, or upper extremities. Despite their rarity, they should be taken into consideration in the differential diagnosis of dermal nodules in infants and children. Histopathology and immunohistochemistry are imperative to confirm the putative diagnosis.
REFERENCES
- Papadopoulos EJ, Cohen PR, Hebert AA. Neurothekeoma: report of a case in an infant and review of the literature. J Am Acad Dermatol 2004; 50: 129–134.
- Harkin JC, Reed RJ. Tumors of the peripheral nervous system. Atlas of Tumor Pathology. Washington, DC: Armed Forces Institute of Pathology; 1969, p. 60.
- Gallager RL, Helwig EB. Neurothekeoma – a benign cutaneous tumor of neural origin. Am J Clin Pathol 1980; 74: 759–764.
- Navarrete-Dechent C, Curi-Tuma M, Marin C, Gonzalez S, Sandoval-Osses M. Cellular neurothekeoma: case report and its (un) relation with nerve sheath myxoma. An Bras Dermatol 2015; 90: 156–159.
- Cesinaro AM, Piana S, Paganelli A, Pedroni G, Santandrea G, Maiorana A. PRAME expression in cellular neurothekeoma: a study of 11 cases. J Cutan Pathol 2022; 49: 338–342.
- Ward JL, Prieto VG, Joseph A, Chevray P, Kronowitz S, Sturgis EM. Neurothekeoma. Otolaryngol Head Neck Surg 2005; 132: 86–89.
- Cavicchini S, Guanziroli E, Del Gobbo A, Scaparro M, Gianotti R. Neurothekeoma, a hard to diagnose neoplasm among red nodules. Australas J Dermatol 2018; 59: e280–e282.
- Massimo JA, Gasibe M, Massimo I, Damilano CP, De Matteo E, Fiorentino J. Neurothekeoma: Report of two cases in children and review of the literature. Pediatr Dermatol 2020; 37: 187–189.
- Stratton J, Billings SD. Cellular neurothekeoma: analysis of 37 cases emphasizing atypical histologic features. Mod Pathol 2014; 27: 701–710.
- Kose D, Ugras S, Harmankaya I, Ciftci I, Koksal Y. Neurothekeoma in childhood: a benign tumor mimicking malignant disease. Turk J Pediatr 2014; 56: 208–211.