SHORT COMMUNICATION
Use of Dermatoscopy in Lesions Suspicious for Melanoma: Two Case Reports
Kevin JANCZURA, Iwona CHLEBICKA, Aleksandra A. STEFANIAK, Andrzej BIENIEK and Jacek C. SZEPIETOWSKI*
Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Chalubinskiego 1, PL-50-368 Wroclaw, Poland.
*E-mail: jacek.szepietowski@umed.wroc.pl
Citation: Acta Derm Venereol 2023; 103: adv18654. DOI: https://doi.org/10.2340/actadv.v103.18654.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: Sep 19, 2023; Published: Nov 16, 2023
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Melanoma is the most aggressive skin neoplasm. It originates from melanocytes located in the basal layer, which produce melanin, a pigment that absorbs ultraviolet (UV) radiation. Although early diagnosis and prompt surgical treatment of melanoma can result in high survival rates, it is frequently diagnosed and treated too late, resulting in a high mortality rate (1). The ability of melanoma to proliferate rapidly and spread further exacerbates mortality rates (2). Hence, increased awareness of skin cancer and regular dermatoscopic examination of suspicious lesions by medical professionals are crucial. We report here 2 patients who were referred with a suspicion of melanoma for examination of skin changes by dermatoscopy and potential further treatment.
CASE REPORTS
Case 1. 40-year-old woman presented with a single, bicolour lesion, approximately 15×10 mm on her right subclavian region (Fig. 1a). The patient reported that the lesion had originally been brown, smaller, and had been present for many years, with no changes or subjective symptoms, such as pain and itch. Recently the patient had noticed that the lesion was changing and a red spot, which grew rapidly, appeared alongside the brown colour. Dermatological examination revealed a flat lesion, well-defined in the pigmented part, and less clearly defined in the remainder of the lesion. The patient had Hashimoto’s disease, but was otherwise healthy, with no prior history of cancer or family history of skin tumours. Dermoscopy revealed 2 distinct cell populations that maintained distinct borders (Fig. 1b). This pattern was consistent with a collision tumour, which is comprised of 2 or more different cell populations. Total excision with an appropriate margin of healthy tissue was performed and the specimen was submitted for histopathological examination. The diagnosis was established based primarily on dermatoscopy examination, then confirmed by histopathology, with a junctional melanocytic naevus and basal cell carcinoma detected.
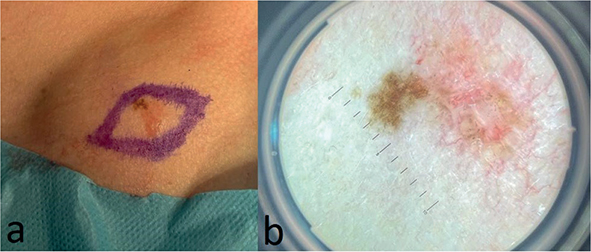
Fig. 1. Case 1. (a) Bicolour lesion before surgery(clinical examination). (b) Dermoscopic image of the lesion: brown reticular pattern coexisting with arborizing vessels and featureless areas. (magnification x10).
Case 2. A 52-year-old man presented with a single, 20×15 mm, multicoloured, lesion on his left shoulder (Fig. 2a). The patient reported that he had first observed the lesion 2 months previously and reported no itching or soreness. The patient was referred to our department of dermatology with a suspicion of melanoma. He was otherwise healthy, with no prior history of cancer or family history of skin tumours. Dermoscopic examination revealed featureless areas, pigment aggregates at the periphery, pigmented oval nests and arborizing vessels resembling tree branches, characteristic of basal cell carcinoma (3) (Fig. 2b).
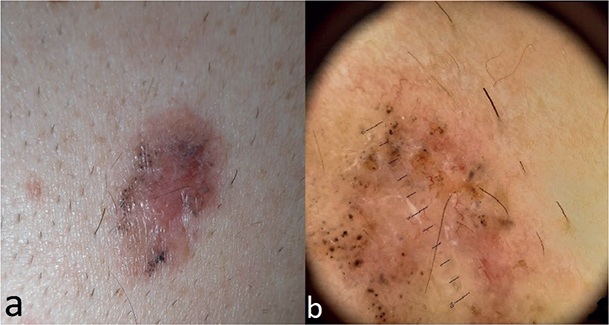
Fig. 2. Case 2. (a) Multicoloured lesion before surgery (clinical examination). (b) Dermoscopic image of the lesion: featureless areas, pigment aggregates at the periphery, pigmented oval nests and arborizing vessels (magnification x10).
Total excision with an appropriate margin of healthy tissue was performed and the specimen was submitted for histopathological examination, which revealed a pigmented basal cell carcinoma.
DISCUSSION
The presence of melanin in a lesion always increases the vigilance of the physician and raises some concerns; hence it is essential to examine lesions thoroughly. Dermoscopy improves diagnostic sensitivity and specificity compared with naked eye examination alone. In case 1, dermatoscopic examination revealed a melanocytic naevus with a lattice of intersecting brown lines, coexisting with a basal cell carcinoma developed with characteristic arborizing vessels, featureless areas, and additional pigment (Fig. 1b). A collision tumour can be composed of 2 benign tumours, a benign and a malignant tumour, or 2 malignant tumours. Due to the rarity of collision tumours, most dermatologists do not have significant experience with accurate diagnosis. Therefore, it is recommended to examine all 4 quadrants of a lesion for signs of malignancy to ensure that there are no signs of malignancy (4, 5).
In case 2 dermoscopy revealed a pigmented variant of basal cell carcinoma.
The occurrence of melanin in a lesion does not always indicate a melanoma; conversely, some pigmented structures, such as blue-grey globules, dots and ovoid nests, maple leaf-like areas, spoke-wheel structures are highly specific for basal cell carcinoma (BCC) (6). However, the most distinctive feature differentiating pigmented BCC from malignant melanoma is the absence of pigment network (7).
On the other hand, the features that are specific to melanoma in dermoscopy are atypical pigment network, irregular streaks, atypical dots and globules of colour, negative network and blue-white veil (8). This indicates the variability of lesions, that can often appear similar macroscopically, but may present differently under dermoscopy. Hence, knowledge of characteristic patterns in dermoscopy is crucial for planning further management.
BCC is the most common type of cutaneous malignancy; hence, it is expected to be diagnosed more frequently than malignant melanoma. Proper initial diagnosis of skin lesions is crucial due to significant differences in patient survival rates between BCC and malignant melanoma. BCC has a much higher survival and curability rate than malignant melanoma. In the case of BCC, alternative therapeutic modalities, such as cryosurgery, topical 5-fluorouracil, or imiquimod 5% cream can also be used (9, 10). In cases of diagnostic uncertainty, it is advisable to excise the lesion surgically for histological examination (11).
REFERENCES
- Davis LE, Shalin SC, Tackett AJ. Current state of melanoma diagnosis and treatment. Cancer Biol Ther 2019; 20: 1366–1379.
- Liu Y, Sheikh MS. Melanoma: molecular pathogenesis and therapeutic management. Mol Cell Pharmacol 2014; 6: 228.
- Trigoni A, Lazaridou E, Apalla Z, Vakirlis E, Chrysomallis F, Varytimiadis D, Ioannides D. Dermoscopic features in the diagnosis of different types of basal cell carcinoma: a prospective analysis. Hippokratia 2012; 16: 29–34.
- Bulte CA, Hoegler KM, Khachemoune A. Collision tumors: a review of their types, pathogenesis, and diagnostic challenges. Dermatol Ther 2020; 33: e14236.
- Blum A, Siggs G, Marghoob AA, Kreusch J, Cabo H, Campos-do-Carmo G, et al. Collision skin lesions-results of a multicenter study of the International Dermoscopy Society (IDS). Dermatol Pract Concept 2017; 7: 51–62.
- Ungureanu L, Cosgarea I, Şenilâ S, Vasilovici A. Role of dermoscopy in the assessment of basal cell carcinoma. Front Med (Lausanne) 2021; 8: 718855.
- Kinnera B, Devi VN, Satyanarayana VVV. The dermoscopy of pigmented basal cell carcinoma. J Cutan Aesthet Surg 2020; 13: 365–367.
- Holmes GA, Vassantachart JM, Limone BA, Zumwalt M, Hirokane J, Jacob SE. Using dermoscopy to identify melanoma and improve diagnostic discrimination. Fed Pract 2018; 35: S39–S45.
- McDaniel B, Badri T, Steele RB. (2022). Basal cell carcinoma. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023.
- Apalla Z, Lallas A, Sotiriou E, Lazaridou E, Ioannides D. Epidemiological trends in skin cancer. Dermatol Pract Concept 2017; 7: 1–6.
- Telfer NR, Colver GB, Morton CA; British Association of Dermatologists. Guidelines for the management of basal cell carcinoma. Br J Dermatol 2008; 159: 35–48.