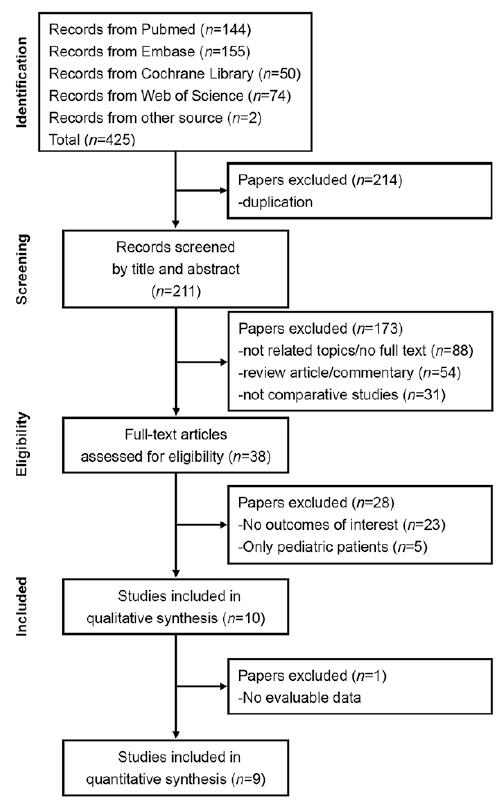
Fig. 1. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow chart of study selection.
1Department of Dermatology, Taipei Medical University Hospital, No. 252, Wuxing St, Xinyi District, Taipei City, 110, and 2Department of Dermatology, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan. *E-mail: living-white@yahoo.com.tw
Accepted Nov 27, 2019; E-published Nov 27, 2019
Acta Derm Venereol 2020; 100: adv00065
Ingrown toenail is a common nail disorder in people of all ages, and the associated pain, oozing, and abscess formation have significantly negative effects on quality of life. Partial nail avulsion with chemical matricectomy is a frequently performed method with a low recurrence rate. Phenol is the most commonly used agent for chemical matricectomy, but other agents, such as sodium hydroxide (NaOH) and trichloroacetic acid (TCA), have shown high success rates for the cauterization of the lateral matrix horn (1). However, only a few head-to-head studies have compared the efficacy of these chemicals. We evaluated the current evidence to determine the most suitable agents for chemical matricectomy using a network meta-analysis (NMA).
A systematic search was conducted in PubMed, Embase, Web of Science, and the Cochrane Library for comparative studies published before 30 May 2019 to evaluate different agents for chemical matricectomy to treat ingrown toenails. Keywords for search included “trichloroacetic acid,” “phenol,” or “sodium hydroxide” combined with “ingrown nails.” The primary outcome was the recurrence rate after partial nail avulsion with chemical matricectomy. For NMA, odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. A random-effects model with an informative prior was used to analyse the direct and indirect comparisons of the NMA. p-values < 0.05 were regarded as statistically significant. Analyses were conducted using NetMetaXL and WinBUGS version 1.4.3 (MRC Biostatistics Unit, Cambridge, UK).
Initially, 425 studies were identified, and after serial exclusion, 10 (3 randomized controlled trials (RCTs), 4 non-RCTs, and 3 retrospective observational studies) studies were included for qualitative synthesis (Fig. 1) (2–11). Table I presents the basic characteristics of all included studies. A final total of 9 studies with adequately evaluable data were calculated in the NMA (2–10). In the pairwise meta-analysis (Table II), both TCA (OR 0.03; 95% CI 0.00–0.26) and phenol (OR 0.18; 95% CI 0.05–0.49) resulted in significantly lower recurrence rates than placebo treatments, but no significant differences in recurrence were detected between NaOH and placebo (OR 0.22; 95% CI 0.04–1.18). TCA showed a trend of lower recurrence rate than phenol, but no significant differences existed between them (OR 0.17; 95% CI 0.02–1.00) (Table II).
Fig. 1. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow chart of study selection.
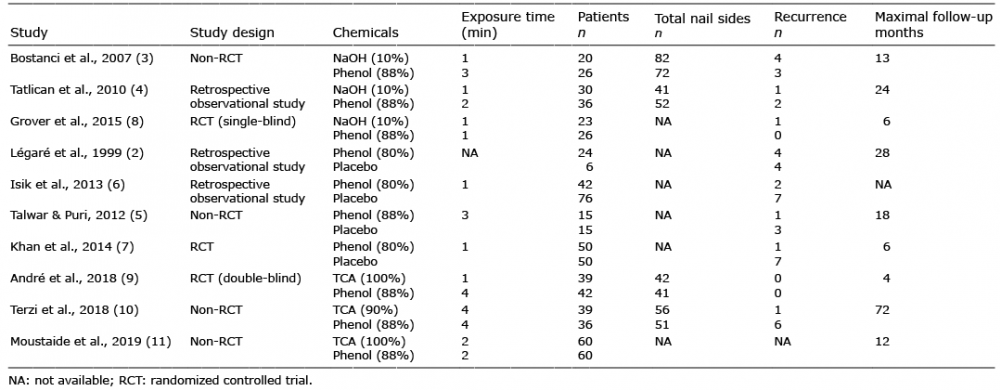
Table I. Basic characteristics of included studies in network meta-analysis
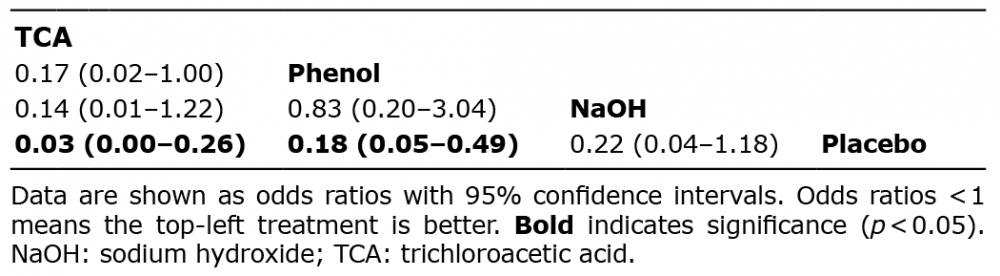
Table II. League table of network meta-analysis comparing the effects of chemical matricectomy with different agents after partial nail avulsion on recurrence rates of ingrown toenails
Partial nail avulsion combined with phenolization was confirmed to prevent the recurrence of ingrown toenails more effectively than surgery alone (9). However, local and systemic toxicities may occur after phenolization, and phenol is contraindicated for patients or clinical practitioners who are pregnant. Conversely, TCA causes no systemic toxicity, since it neutralizes itself after reacting locally with the skin (12, 13). Our results indicate that TCA is comparable to phenol for chemical matricectomy for reducing recurrence of ingrown toenail.
In addition to the recurrence rate, an ideal agent for chemical matricectomy should enable a lower degree and shorter duration of pain, shorter period of postoperative drainage, lower inflammation or infection rates, and faster healing time. However, few studies are available to perform a pooled analysis of the postoperative morbidities occurring after treatment with TCA or phenol. We could only summarize the results from the individual articles. For postoperative pain, most patients experienced only mild pain with TCA or phenol, and similarity in incidence, duration, and severity of pain were noted between these 2 agents. Controversy existed regarding the post-treatment drainage, inflammation, and infection between TCA and phenol (9–11). Only one study indicated significantly shorter healing time in the TCA treatment group than in the phenol treatment group (11). Additional studies are warranted to elucidate the aforementioned inconsistency.
Some limitations of the current study included inherent bias regarding the design in the recruited studies, insufficient data for the analysis of post-treatment complications, and variations in the follow-up interval and application times of chemical matricectomy.
In conclusion, the present NMA indicates that TCA is comparable to phenol for chemical matricectomy after partial nail avulsion to reduce the recurrence rate of ingrown toenails. TCA could therefore be considered as a safe agent for chemical matricectomy in clinical practice.
The authors have no conflicts of interest to declare.